
Abstract
Background
Smoking is a serious risk to health globally. Health care professionals play a key role in the prevention of smoking as they are considered a role model by patients.
Objectives
The aims of this study are to evaluate smoking rate among physicians and dentists from Sulaymaniyah, Iraqi Kurdistan, Iraq, and to understand their knowledge and attitudes toward tobacco smoking.
Methods
A cross-sectional web-based survey was conducted involving physicians and dentists working in both University of Sulaimani and Sulaymaniyah Teaching Hospitals. A questionnaire created based on World Health Organization Global Health Professional Survey with slight modifications was emailed to the study participants and the responses received were analyzed.
Results
Incidence of smoking among physicians and dentists was 26.5%, with a significantly higher rate among male compared to female health care professionals. The mean age of starting smoking was 22.3 (±4.8) years. Only 7.3% of health care professionals received formal training on smoking cessation. All responders agreed that smoking is harmful to health. However, ever smokers compared to never smokers were less likely to agree that health care professionals should set a positive impact by not smoking.
Conclusion
Smoking rate is high among physicians and dentists from Sulaymaniyah city/Iraq, and at the same time, there is a low rate of training on smoking cessation.
Introduction
Worldwide, tobacco use represents one of the major causes of death and the main preventable cause of lifestyle-related diseases, such as lung cancer, chronic obstructive pulmonary disease, and coronary heart disease.1,2 It is also one of the risk factors of oral cancer. 3 The detrimental effects of tobacco use on oral health are extensively documented in studies focusing on changes in the oral mucosa4,5 and periodontal tissues.6,7
Although the damages of smoking are well known, several studies have shown a high prevalence of smoking habits among health care professionals,8–12 which always sets a bad example to their patients.13,14 It is also evident that health care professionals could better persuade patients to stop smoking if they themselves are not smokers. 15 High rates of smoking among doctors and other health care workers and limited availability of help for de-addiction from smoking may compromise the ability of physicians to effectively treat patients addicted to smoking. 16 Several studies have demonstrated the efficacy of smoking cessation programs and the importance of physician's advice to their patients.17,18 Physicians should be encouraged to assist smokers to quit, especially considering that almost half of former smokers indicate health conditions as the main reason to stop smoking. 19
As medical professionals can play a key role in the process of smoking cessation both as advisers and behavioral models for the citizens, it is necessary to have information on the habits and attitudes of health care professionals toward smoking, especially concerning their role to provide help to smokers, who wish to quit smoking. 20 Dental professionals play a significant role in identifying smokers, as they may notice intraoral signs, such as odor, tooth stains, and oral hygiene problems, earlier than other health care professionals; hence, dentists are in a better position to offer preventive care. 21
Incidentally, smoking rate among health care professionals in most developing countries22–26 is high compared to that in developed countries.16,27 Smoking prevalence rates of 26.5%, 30.9%, and 12% were recently reported among adult Iraqi population, 28 male health physicians of Hilla (another Iraqi city), 29 and medical college students of University of Sulaimani, Sulaymaniyah, 30 respectively. However, studies analyzing smoking rate, knowledge, attitude, and practices among health care professionals in Sulaymaniyah or other Iraqi city are inadequate; in addition, antismoking campaigns are lacking in Sulaymaniyah. Hence, we conducted this study with the following aims:
To evaluate the smoking rates among a sample of health care professionals in Sulaymaniyah, the second largest city in Iraqi Kurdistan located in northern Iraq.
To know the extent of tobacco cessation training in medical school and public health places.
To estimate the degree of knowledge and attitude of health care professionals (physicians/dentists) toward tobacco smoking between ever and never smokers.
Methods
A cross-sectional study was conducted over a three-week period (1–22 November, 2015) in Sulaymaniyah, using a web-based questionnaire created using Google form service. The questionnaire was based on the World Health Organization (WHO) Global Health Professional Survey with slight modifications by researchers to make it more amenable for filling via web (as it is a web-based survey) and suitable for use by the physicians and dentists of Sulaymaniyah. The questionnaire was piloted among 30 physicians and dentists of the same study group to ensure clarity of the questions; the pilot sample results were not included in the main study results. The research proposal was approved by the scientific and ethics committee at the Faculty of Medical Sciences, University of Sulaimani, Iraq.
The required sample size was calculated according to the expected prevalence rate of smoking, which indicated the requirement for at least 323 participants, with 5% margin of error at 95% level of confidence.
The study population consisted of a group of physicians and dentists with different grades and specializations (including general practitioners, residents, and different specialists) working at the University of Sulaimani and Sulaymaniyah Teaching Hospitals.
The web link to the questionnaire was emailed to the participants (910 physicians and 110 dentists). A reminder email was sent after one week from the first email. The email also included a description of the survey explaining the purpose of the study and specific instructions for completing the questionnaire. Standard procedures of informed consent were used ensuring participants’ anonymity and confidentiality of their response.
The questionnaire consisted of an open-ended question (about the age of starting smoking) and 29 close-ended questions, investigating the following topics:
Personal and occupational data (gender, age group, professional qualification, and department).
Knowledge about smoking (ie, smoking as a risk factor for several diseases and health care professionals as models for citizens).
Attitudes (ie, opinion about nonsmoking policies).
Job setting (ie, presence of nonsmoking signs and smoking among health care professionals in the hospital and clinic).
Clinical activities (asking about patient smoking and nonsmoking policies and training on smoking cessation).
Smoking habits.
Smoking pattern (for smokers only) (ie, smoking habit, willingness to stop, and opinion about any attempt to quit).
A daily smoker was defined as someone who smoked cigarette at the time of the survey (at one or more days during previous 30 days). An exsmoker was someone who smoked daily or occasionally, but did not smoke during the time of the survey. The current smokers and exsmokers were grouped together to ever smokers for further analysis. A never smoker was someone who never smoked at all or had never been a daily smoker.
Statistical Analysis
Data processing and analysis were performed using the statistical software, SPSS version 17. Descriptive analysis was performed using frequencies and percentages for categorical variables, ie, gender, age group, number, ever smokers, and never smokers. Age of starting smoking is represented as mean ± standard deviation. χ 2 tests were performed to evaluate the differences for smoking characteristics, knowledge, and attitudes among ever- and never-smoker physicians and dentists. Smoking status among different specialization was also compared. P-value of <0.05 was considered as statistically significant.
Results
Among 1020 health care professionals (910 physicians and 110 dentists) who received the link of the web-based questionnaire through email, only 430 responded to the questionnaire (359 physicians and 71 dentists), giving a response rate of 42.2% (39.5% among physicians and 64.5% among dentists). In total, 43% of males and 39.4% of females responded to the questionnaire. Eight questionnaires were deleted due to excessive missing information, especially when question about smoking status is missing. Remaining four hundred twenty-two responses were analyzed.
Smoking Behavior
Smoking rate (including current smoker and exsmoker) among the health care professionals studied was 26.5%; the rate was more among male than female patients and higher among professionals with more experiences; these results are statistically significant (Table 1). Smoking behavior among current smokers is presented in Table 2. The mean age at which they started to smoke was 22.3 ± 4.8 years.
Main characteristics of the study sample.

For these characteristics, the results are statistically significant (P-value <0.05).
The characteristics of current smokers regarding the number of cigarettes smoked, question about their smoking behavior, and their feeling about smoking.
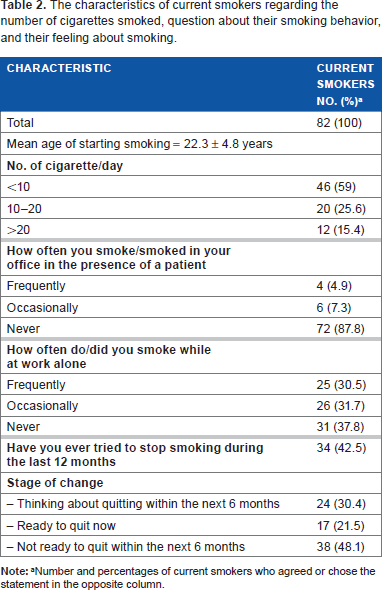
Number and percentages of current smokers who agreed or chose the statement in the opposite column.
Smoking characteristics (ever and never smokers) among different medical specializations were assessed. The highest (40.5%) and the lowest (17.4%) smoking rates (ever smokers) were observed among surgeons and general practitioners, respectively. These differences are statistically significant (P-value <0.05).
Smoking Knowledge
Among the study participants, 91% of them believed that lung cancer is among the most common consequences of smoking, followed by heart attack (55.1%), oral cancer (47.5%), and atherosclerosis (47.3). Only 29% of them chose hypertension and preterm birth as one of the most common consequences of smoking. Interestingly, there was a common agreement that smoking is harmful to health among physicians and dentists in both ever and never smokers with minor differences (Table 3).
Comparisons of ever-and never-smokers with regard to their agreement to the questions between physicians and dentists.

P-value <0.05 between ever- and never-smokers.
P-value <0.05 between physicians and dentists.
For these statements, the numbers of participants were different, as part of them did not have clinics or waiting room or did not see patients/adult patients routinely (those professionals include: laboratory doctors, some basics, and pediatricians). Patients who chose not applicable option were excluded from the calculation of percentages.
Smoking Attitude
Significant differences were observed between the ever-smoker vs never-smoker group and between the physician vs dentist group about the following statements: (1) duty of health care professionals to convince people, (2) health care professionals who smoke are less likely to advice people, and (3) health care professionals should set a good example by not smoking. For these statements, ever-smokers were less likely to agree with the statements, while for some questions, ever-smoker dentists were less likely to agree in comparison to ever-smoker physicians (Table 3).
Training
For question about training on smoking cessation, in general, 5.6% of health care professionals received formal training on strategies for smoking cessation (Table 3).
Promotion of Smoking Cessation Behavior
When question asked about their practices at hospital or their clinic, after excluding those who do not have waiting room or clinic, significantly higher rate of never-smoker vs ever-smoker physicians persuade their patients to stop smoking in every visit (Table 3). For the question that asked about the situation that prompts to advise the patient against smoking, 62.9% of them advice the patients against smoking when a patient had symptoms or diagnosis of smoking-related diseases, and 9.9% of them advice when patient himself raises the question about smoking.
Discussion
Studies evaluating the rate of smoking and those evaluating the knowledge and attitudes of health care professionals in Sulaymaniyah are scarce. Hence, this study was designed to fill this knowledge gap. The prevalence of smoking among students of the medical college of the University of Sulaimani at 2014 by Ramzi 30 was lower than our observations among health care professionals in this study. The smoking rate in this study was also higher than that reported among a sample of general population of healthy workers in Sulaymaniyah at 2010. 31 The probable reasons for the higher prevalence of smoking among health care professionals may be due to occupational stress, which is considered as a key factor in addition to addiction, enjoyment, and peer influence. 32
Smoking Rate among Physicians and Dentists
In this study, smoking rate was high among physicians, which is consistent with previous reports from some other Asian countries (Iran 22 and Pakistan 23 ). However, our estimate of smoking rate was lower than reports from Kuwait 24 and Jordan 25 and higher than reports from Oman 33 and Turkey. 34
Our finding of smoking rate among dentists was lower than physicians. The rate of smoking among dentists is much lower than reports from Saudi Arabia (33.8%). 26 In a sample of Omani health care professionals (physicians and dentists), 25% of the dentists were smokers, 33 although the Oman study included all forms of tobacco. These variations in smoking rate among neighboring and other Asian countries might be related to real differences or may be due to differences in study protocols, such as study population, method of data collection, forms of tobacco, and/or differences in the definition of smokers between studies.
As noted throughout different studies, smoking rate among health care professionals in most developing countries (Iran, Pakistan, Kuwait, Jordan, and Saudi Arabia)22–26 was higher when compared to developed countries, such as Japan 27 and Italy. 16 Better health system with better education and more antitobacco training program in developed country may be responsible for such lower incidence rate.
Gender and Age
The rate of current smokers among male health care professionals was 33.5%, which is similar to the rate reported from another city in Iraq and wider Mediterranean region [WHO Eastern Mediterranean Region study (WHO EMR)],34,35 Interestingly, compared to other studies, smoking rate among females was significantly lower than males. None of the female physicians were smokers in Hilla study, 34 and 5% of the females were smoker in WHO EMR study. 35 In general, the pattern of smoking in male and female differs between developing and developed countries, which is attributed to cultural differences. Significantly more males (40%–60%) and fewer females (2%–10%) smoke in developing countries when compared to 25%–35% male and female smokers in developed countries. 23 This is largely due to social unacceptability of female smoking behaviors in some developing countries. Consistent with previous studies,16,23,31,34 highest smoking rates were observed in older age group.
Smoking Behavior
The mean age of smoking onset in this study and among Jordanian health care professionals was high in comparison to the two studies from Italy.16,32 Again differences in culture and social life in Europe may explain this difference. The difference may also be due to differences in population sampled as the latter included paramedics. Regarding the number of cigarettes smoked per day, in this study, most of the smokers smoked less than a pack per day similar to a previous report. 34 Average cigarette smoked per day was 16 in WHO survey on health care professionals of EMR, 35 and it was lowest in Saudi Arabia (11 cigarette per day) 35 and highest in Jordan (19 cigarettes per day). 25
A very few studies have addressed the comparison of smoking rate among different medical specializations.27,36 The differences in categorizing medical specialization in different studies make comparisons difficult. In this study, smoking rate was observed to be higher among surgeons similar to previous reports.27,36
Knowledge and Attitude
Consistent with previous reports, 37 there was a common agreement among health care professionals that smoking is harmful to health. In WHO EMR, 35 70% and 83% of ever and never smokers, respectively, agreed that health care professionals who smoked were less likely to advice people to stop smoking.
Training
Very few (5.6%) health care professionals received any formal training on smoking cessations; this was much lower than the Hilla study (33%), 29 which could be due to additional inclusion of seminars besides training on smoking cessations in Hilla study. In the Italian study, specific training on smoking cessation was given to 17% of physicians. 16
The high rate of smoking among physicians and dentists in Sulaymaniyah, together with small percentage of those who were ready to quit, is worrying. Smoking in the presence of a patient (5.5%), absence (53.1%) of no smoking sign in their waiting room, advice of patient only in the presence of symptom or diagnosis of smoking-related diseases (62.9%), and lack of adequate training program are inappropriate attitudes that need considerable improvement. These are alarming signs to the health system to initiate suitable public health measures, by starting more formal training on the adverse effects of tobacco smoking, cessation programs, and antismoking campaigns, with compulsory participation from students and health care professionals in Sulaymaniyah.
Limitation of the Study
The response rate in this study was low (42.2%) in comparison to studies using the paper-based questionnaire (70%, 33 77%, 37 and 86.5% 26 ), while it is high in comparison to another web-based questionnaire study. 38 As implied in other studies, the web-based questionnaire studies are associated with lower response rates (to date, response rates for email surveys appear to be lower than those of traditional mail surveys). As one group of researchers recently observed, the potential of the electronic survey is too great to be ignored, while web-based survey has advantages over paper-based survey, due to its quick reach, flexibility, and cost effectiveness. 39 Sending more reminder emails, with providing initiatives for responding to studies and longer time frame, might increase the response rate. Another limitation of this study is low response rate among older age group, as only 7.3% who respond were above 45 years. This might be related to more busy life, less time spending on the Internet, with less use of modern technology by older age group, especially in our society, as web-based survey is new to our city. However, this may improve with time and adoptability to modern technology. Moreover, sampling frame of physicians and dentists is not completely representative of all health care professionals in the city. Our study sample might apply mostly to highly qualified persons, and hence future studies should include all health care professionals, such as nurses, technicians, and other paramedics. Another limitation of the study as addressed by other cross-sectional studies 30 is the use of questionnaire, which is a self-reported approach and could lead to underreporting and recall bias.
Conclusion
The incidence of smoking among physicians and dentists in Sulaymaniyah was high with low rate of formal training among health care professionals, which is a cause of concern. Steps need to be taken by the health care system against tobacco use, such as strict legislation to prohibit cigarette smoking in health care centers and hospitals and necessary optimal comprehensive campaigns to overcome this problem. The level of awareness should also be raised among health care professionals and students by focusing on smoking cessation techniques and programs and the inclusion of training materials on smoking hazards in the medical school curriculum.
Author Contributions
Conceived and designed the experiments: Darya Saeed Abdulateef, and MIGM. Analyzed the data: Darwn Saeed Abdulateef, AJA, and Darya Saeed Abdulateef. Wrote the first draft of the article: Darya Saeed Abdulateef and Darwn Saeed Abdulateef. Contributed to the writing of the article: Darya Saeed Abdulateef, AJA, Darwn Saeed Abdulateef, and MIGM. Agreed the study results and conclusion: Darya Saeed Abdulateef, AJA, Darwn Saeed Abdulateef, and MIGM. Jointly developed the structure and arguments for the paper: Darya Saeed Abdulateef, AJA, and MIGM. Made the critical revisions and approved the final version: Darya Saeed Abdulateef, AJA, Darwn Saeed Abdulateef, and MIGM. All authors reviewed and approved the final article.
Footnotes
Acknowledgments
The authors would like to thank the following physicians and dentists: Sara Saeed, Shadan Jabar, Kanar Jalal, Professor Mohammed Abdulrahman and Assistant Professor Saeed A-latteef (Vice Dean of Dentistry school), and Shilan Hussein Karim (Vice Dean of School of Medicine) for their help by providing emails (for sending the link of questionnaire) of physicians and dentists’ of Sulaymaniyah Teaching Hospital and School of Medicine and Dentistry at the University of Sulaimani.