
Abstract
Introduction
Smoking by health professionals is a very negative habit not only for their own health, but also because it diminishes their capacity to influence their smoker patients to quit their habits.
Objective
The aim of this study was to assess the trend of the smoking prevalence, as well as the impact of the 2005 Spanish Smoking Act, among healthcare professionals.
Methods
Participants were asked about their smoking consumption in the baseline and the follow-up questionnaires in a Spanish dynamic prospective cohort of university graduates (the SUN Project) from 1999 to 2008. Non-conditional logistic regression models were fit to assess the relationship between type of profession and prevalence of smoking.
Results
The proportion of current smokers at the entrance into the cohort was 16.4% for physicians, 20.8% for pharmacists, 23.4% for nurses and 24% for other university graduates. The risk of being current smoker (adjusted OR [95% CI]) was lower in physicians (0.68 [0.61–0.76]) but not in pharmacists (0.94 [0.84–1.06]) or nurses (0.94 [0.84–1.05]) compared to other university graduates. All professional groups presented a statistically significant decline of smoking prevalence from 1999 to 2008. This decline might be at least partly due to the impact of the Spanish legislation on their smoking habits.
Conclusion
This study shows a decline in smoking prevalence among Spanish physicians. This decline has reached lower levels than what is current among other professionals and the general population. However, there is still a high number of smokers among health professionals, thus more efforts are needed to achieve lower levels of tobacco consumption.
Introduction
According to the World Health Organization (WHO), tobacco use is a risk factor for six of the eight leading causes of death in the world; it is even estimated that it could kill one billion people during the twenty first century. Moreover, smoking is considered a growing epidemic by the WHO since the number of smokers worldwide is expected to increase in the following years. Paradoxically, tobacco is also the “single most preventable cause of death in the world today” and for this reason the WHO has developed the MPOWER package which describes six policies to reverse this tobacco epidemic. 1 One of these policies consists in offering smokers help to quit, making this intervention highly dependent on the participation of well-respected health professionals with whom tobacco users may have a good relationship.
Health professionals have an exemplary role on public health issues such as smoking because, since they are perceived as most knowledgeable in health matters, they are expected to behave according to this knowledge. 2 This role model function is very important since physicians could best influence their smoker patients to quit their habit if they did not themselves smoke. 3 Several studies have shown that healthcare providers who smoke are less likely to initiate cessation interventions.4,5 There is only limited evidence on the association between the smoking status of healthcare professionals and the success related to smoking cessation interventions. A French study found no difference in the effectiveness of a smoking cessation trial among smoking and non-smoking general practitioners. 6 However, a later quasi-experimental study found that patients who received a smoking counseling intervention from a non-smoking general practitioner were more likely to benefit in comparison to patients who were counseled by a smoking general practitioner. 7 Therefore, smoking among health professionals may be one of the obstacles when trying to involve health professionals in tobacco control.
Several studies have been published about the smoking prevalence among health professionals such as physicians,8–10 nurses, 11 or dentists. 12 Smith and Leggat showed that smoking prevalence in the medical profession varies widely around the world but a steady decline can be found in countries such as the United States, Australia and the United Kingdom. 13 This gradual decline is similar to what is happening among the general population in high-income countries. 1 A reason for this general decline is the growing number of tobacco control policies developed in many countries. 14 Thus, the increasing number of preventive measures can also explain the decline of smoking prevalence among health providers. 15
The existing cross-sectional studies that deal with smoking prevalence among health professionals in Spain have some drawbacks, such as data not being recent, that the survey was focused on professionals from specific regions, or that the sample size was very low.16–20 A more recent study on the impact of the 2005 Spanish Smoking Act (which came into force in 2006), has yet another limitation: participants are hospital workers and not specifically heath professionals. 21
The aim of this study is to show the contemporary trend of the smoking prevalence, as well as the impact of the 2005 Spanish Smoking Act among health professionals.
Methods
The SUN project (Seguimiento Universidad de Navarra (University of Navarra Follow-up)) is a prospective cohort study. A detailed description of the study methods has been previously published. 22 Briefly, recruitment of participants started in December 1999 and is permanently open, as the study was designed to be a dynamic cohort. Most of the participants are health professionals and/or graduates from the University of Navarra. They were recruited through collaborations with Universidad de Navarra Alumni Association and professional associations throughout the country (e.g. regional associations of Physicians, Nurses, Pharmacists, Dentists, and Engineers). The proportion of professionals included in the cohort varies across the years of entrance because it was dependent of the specific agreements reached with specific associations. After the baseline assessment, participants received biennial mailed follow-up questionnaires collecting a wide variety of information about diet, lifestyle, risk factors, and medical conditions. Voluntary completion of the first questionnaire was considered as informed consent and the project protocol was approved by the institutional review board of the University of Navarra.
Participants were asked about their smoking consumption in the basal and the follow-up questionnaires. Smoking status was classified as current, former or never smokers. Current smokers were defined as participants who self-reported smoking at the baseline questionnaire. The dynamic characteristic of the SUN cohort allowed the use of data from participants as multiple cross-sectional studies. Therefore, prevalence of smoking at the entrance of the cohort was compared from 1999 to 2008. The number of participants beginning in 1999 is very low since the cohort started by the end of the year. Participants were asked about their studies at the University and they were classified in four categories: physicians, pharmacists, nurses and other professions. Other covariates included in this study were sex, age, body mass index and working status.
The analysis was carried out using SPSS 15.0 software package. Frequencies were calculated for categorical variables and mean and standard deviations (SDs) for quantitative variables. Non-conditional logistic regression models were fit to assess the relationship between type of profession and prevalence of smoking. Odds Ratios (OR) and their 95% Confidence Intervals (CI) were calculated taking as the reference category those subjects who were not physicians, pharmacists or nurses. Because socio-demographic characteristics of participants varied through the cohort, prevalence of current smokers was adjusted for age and sex. We also fitted multivariate models additionally adjusted for working status (employed/unemployed) and the year of entrance in the cohort. We conducted tests of linear trend (likelihood ratio test) across prevalence of smoking depending on the year of entrance at the cohort. Current smokers were compared with the rest of participants, including those with missing data for smoking. All p values were two tailed, and significance was set at p < 0.05.
Results
By December 2008, the dataset of the SUN Project included 20,197 participants. Characteristics of the participants according to their profession are shown in Table 1.
Characteristics of the participants according to their profession.
Other university graduates.
Mean (standard deviation).
The proportion of current smokers at the entrance into the cohort was 22.3% (4,497 out of 19,675 participants who informed about their smoking status). The prevalence of smoking status by profession type is shown in Table 2. Among them, physicians had the lowest smoking prevalence.
Prevalence of smoking status at entrance into the SUN cohort by profession. *

Total number is lower than 100% because 2.6% of participants had missing data on questions related to smoking. (χ2 test: p < 0.001).
Other university graduates.
Table 3 shows the results of the logistic regression models fitted to evaluate the association between type of profession and the prevalence of current smokers. In the three healthcare professions the odds for being current smoker was lower than for other professions. However, a significantly lower smoking prevalence was only found for physicians in the fully adjusted multivariate regression model. Pharmacists exhibited lower prevalence in the partially adjusted model. Table 3 also shows the result of the multivariate analysis stratified by sex and by year of entrance into the cohort.
Odds ratios and 95% CI of being current smoker at the entrance into the cohort.

Other university graduates.
Logistic regression model adjusted for age and sex. Age did not show a linear relationship with smoking status, a quadratic transformation of age was introduced in the model and the likelihood-ratio test was statistically significant.
Model 1 plus additional adjustment for working status and year of entrance into the cohort.
Adjusted for all variables included in model 2 except sex.
Adjusted for all variables included in model 2 except year of entrance into the cohort.
In an alternative multivariate regression model, we observed that the risk of being smoker was lower among those participants who had entered in the cohort from 2006 onwards, compared to those who entered before this year (adjusted OR = 0.73, 95% CI [0.67–0.80]). This value was adjusted for age of participants, type of profession and working status.
We also observed in an analysis stratified by type of profession that the risk of being current smoker was always lower in participants who had entered in 2006 or later, than in those who entered before this year. The OR (95% CI) was 0.77 (0.59–1.00) for physicians, 0.76 (0.63–0.92) for pharmacists, 0.79 (0.44–1.42) for nurses and 0.69 (0.61–0.78) for other professions. However, the adjusted ORs obtained in the fully adjusted multivariate analysis were not statistically significant.
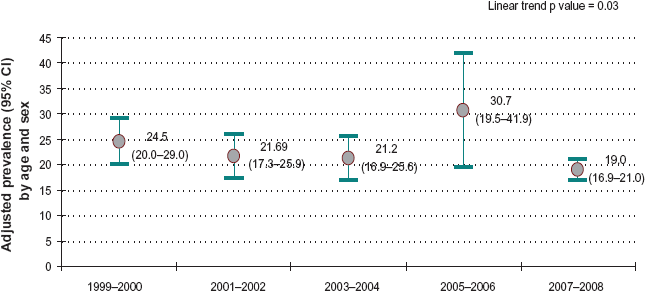
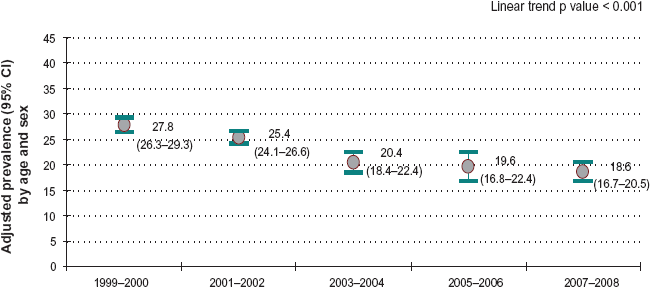
We show in Figures 1 to 4 the adjusted smoking prevalence by profession during the years of entrance into the cohort. All professional groups presented a statistically significant decline in smoking prevalence. For physicians the smoking prevalence was always lower than for any other profession.

Smoking prevalence among physicians at the entrance at the SUN cohort (95% CI).
Smoking prevalence among pharmacists at the entrance at the SUN cohort (95% CI).

Smoking prevalence among nurses at the entrance at the SUN cohort (95% CI).
Smoking prevalence among other professionals at the entrance at the SUN cohort (95% CI).
Since the SUN project is a dynamic cohort, a final analysis was performed with those current smokers with available follow-up information. We found that 972 out of 2381 current smokers (40.8%) gave up smoking during the follow-up period. The quit rate was 46.9% for nurses (136 of 290), 46.5% for pharmacists (73 of 157), 38.6% for physicians (91 of 236) and 39.6% for other professionals (672 of 1698) (p = 0.044). The association between type of profession and quit rate was not statistically significant in a multivariate regression model adjusted for age and sex.
Discussion
This study shows a gradual decline of smoking prevalence among healthcare professionals in Spain from 1999 to 2008. The lowest prevalence, as well as the lowest odds of being current smoker, was found among physicians. Smoking prevalence was not significantly lower for pharmacists or nurses as compared to the participants with other professions when we adjusted for potential confounders. Moreover, during the last year, the prevalence of current smokers adjusted for age and sex was higher for pharmacists than for other professionals. Our results also suggest a smoking decrease among all kinds of professionals; this might be at least partly due to the impact of the Spanish legislation on smoking habits. The proportion of smokers who gave up during the follow-up period was higher among pharmacists and nurses although these differences were not statistically significant after adjusting by potential confounders.
The smoking prevalence found in our research is lower than most results found in previous studies in Spain that focused mostly on physicians and/or nurses. A review of several surveys conducted in Spain found a decreasing trend of the smoking prevalence. In this review, the highest prevalence found was 47.9% in 1985 among a representative sample of physicians and the lowest prevalence was 32.8% in 1992 among a sample of 381 physicians. 16 A cross-sectional descriptive study developed in 1998 showed that 34.7% of the physicians and 43.2% of the nurses were current smokers. 17 Fernandez et al found a smoking prevalence among female physicians of 34.7% in 1998 and 37% in 2001, and among female nurses, the prevalence was 47.6% in 1998 and 47% during 2001. 18 Results from the 2002 Catalan Health Survey show a smoking prevalence of 24.5% among physicians, 35.1% among nurses and 20.4% among pharmacists. 23 Therefore, the lower prevalence found in our study may be partly explained by the decreasing trend of the smoking habit among healthcare professionals participating in a cohort and by the fact that they were probably more health conscious. This finding is consistent with the results from other countries.8,9,11
Notwithstanding, the smoking prevalence found in our study might be underestimating the actual prevalence in Spain since the latest data published in the online Tobacco Atlas shows a smoking prevalence of 37% among Spanish health professionals. 27 This difference may be explained by the fact that our sample is not representative of the healthcare professionals in Spain. They are volunteers in a long-term cohort and, therefore, they are likely to be more motivated in healthcare related issues such as tobacco. Another bias is related to the social undesirability of tobacco and, therefore, participants may report healthier lifestyles. Finally, fluctuations found in the adjusted prevalences may be explained by the differences among participants comprising several waves of the SUN cohort included in our analysis. Participants in the first waves were graduates from the University of Navarra and different reasons could explain their motivation to collaborate with this research. On the contrary, participants in the last waves are mostly health professionals and they can be probably mostly motivated because they themselves were following healthier lifestyles.
Health professionals have a critical role to play in battling the tobacco epidemic because of the potential benefits of smoking cessation advice provided by them.2,24,25 For this reason, it is important to increase their training as well as their engagement in smoking cessation programmes. 26 A good strategy in order to achieve this aim might be to address those barriers that limit this engagement such as their own smoking status. 5 Our results show that Spain is still far away from the low smoking prevalence among health professionals in countries such as Portugal (18%), the United Kingdom (7%) or the US (4%). 27 Therefore more efforts are needed to achieve lowest levels among Spanish healthcare professionals. An important step is the promotion of smoking cessation measures also among health professionals; in this regard, there are helpful initiatives that could be developed, such as by the Tobacco Free Nurses Program, the first national program created in the US with the objective of helping nurses quit. 28 However, it is also important to develop earlier interventions since most people become addicted to tobacco before they decide to become healthcare providers. 2 Results from the Global Health Professions Students Survey conducted among students attending dental, medical, nursing and pharmacy schools from 2005 to 2007 showed that over 20% of the students already smoked, in 18 out of the 31 countries sites surveyed. 29
Finally, our results showed a gradual reduction in smoking prevalence among health professionals and it seems that the Spanish act on smoking had a mild impact on this trend. This finding is coincident with another study which showed a slight change (5 out of 118 smokers), after this law came into force, in the quit ratio among Spanish hospital workers who smoked. 21 Moreover, even if Spain was until 2005 30 one of the less regulated European countries, a gradual decline in smoking habits might be explained by the fact that some legal initiatives had been introduced during the last two decades which specially affected health professionals. Two examples are the smoking restrictions in 1988 in health and educational centers and the National Action Plan for Prevention and Tobacco Control approved in 2003. 31 In fact, a previous study has shown a linear relationship between the increased number of tobacco control policies and the quit ratios in the general population in European countries. 14 However, the long-term effect of this act should be also taken into account in future studies. Moreover, yet another factor might be the influence that the international movement against tobacco, promoted by the WHO and supported by health professional organizations, is exerting on physicians, pharmacists and nurses. 2
As a conclusion, our study shows a decline of smoking prevalence among healthcare professionals and levels below other professions and the general population. However, the proportion of smokers is still very high and more efforts are needed to achieve the low levels of tobacco consumption in other countries. The World Health Organization has recognized the irreplaceable position that health professionals have on tobacco control. The Code of practice on tobacco control for health professional organizations states that health professionals, due to their role-model status, should be encouraged not to use tobacco and to promote a tobacco-free culture. 32
Disclosures
The authors report no conflicts of interest.
Footnotes
Acknowledgements
The SUN Study has received funding from the Spanish Ministry of Health (grant numbers PI042241, PI040233, PI050976, PI070240, PI070312, PI081943 and PREDIMED study 06/0045), the Navarra Regional Government (PI14/2005, PI36/2008) and the University of Navarra, Spain.
The authors are very grateful to all participants of the SUN Study for their continued cooperation and participation. We also thank all members of the SUN Study Group for administrative, technical and material support, and Dr. Rosalia Baena for her contributions in editing the English style of this manuscript.