
Abstract
Background
Tobacco use is considered one of the largest public health threats facing the world. The estimated number of current smokers in the world exceeds 1.3 billion, which means that one third of the world's population above 15 years are smokers. Smoking prevalence is increasing in the developing world but monitoring of this trend is poor in these countries. Studies on smoking in Iraq are scarce, with the current smoking prevalence rate reported to be 15–25% for males and 1–10% for females in surveys conducted in the past ten years.
Objectives
This study aimed to find the prevalence of smoking among Karbala University students in Iraq and determine its associations with participants' demographic and other related predictors, including other substance use behaviors, to help inform and develop future prevention and control programs.
Material and Methods
A categorical random sample included 2298 students at Karbala University in Iraq who answered a self-completed questionnaire. The questionnaire was based on the Drug Abuse Program questionnaire and was piloted before implementation. Descriptive and analytic statistical tools (SPSS-20) were used to assess significant associations at P < 0.001 to compensate for multiple comparisons.
Results
The prevalence of current smoking among Karbala University students was 10.5%, shisha smoking 4.4% and previous smoking (having ceased smoking for more than 30 days) 1.0%. Approximately half of the smokers surveyed (45.7%) started smoking before the age of 18. Smoking was positively related to male gender, increasing age, being unmarried, college, drinking alcohol, having a positive attitude toward smoking and higher fathers' educational level.
Conclusion
Lifetime smoking prevalence was found to be approximately two out of ten students. Significant positive association was found between smoking and other substance use behaviours. Additionally it was associated with positive attitudes toward substance use.
Significant predictors were determined. Further studies are needed to explore the prevalence of smoking among Iraqi youths to find trends and help to guide the implementation scientifically based control and prevention programs.
Introduction
Tobacco use is considered one of the largest public health threats the world has ever faced, and there are more than 1.3 billion smokers in the world. Smoking results in about six million deaths per annum (9% of total world deaths) and this number is expected to exceed ten million by 2020. The World Health Organization (WHO) graded tobacco use only second to hypertension among major death causes. 1
Although smoking prevalence is decreasing in high-income countries, it is increasing in middle- and low-income countries, 2 with prevalence trebling between 1970 and 2000 in developing countries. 3
Scientific resources for surveys in developing countries are scarce and preventive and curative resources are deficient. A report from the Eastern Mediterranean Region Office of the WHO (EMRO) concluded that current smoking prevalence increased 24% between 1990 and 1997. 4 The report estimated that half of adult males in the Middle East are smokers, with Egypt showing the highest number of people that use tobacco. The report showed that in the states of the Gulf Cooperation Council, 50% of students aged 14 to 18 years smoke, and around 25% of smokers started between the ages of 10 and 15 years. 4
Additionally, the recent increasing prevalence of shisha (water pipe) smoking, especially among both male and female youths, represents a further serious concern. The habit appears to be common in females, because they are aggressively targeted as potential shisha users with advertising in fashion magazines. These advertisements emphasize the perceived benefits of independence, stylishness, weight control, sophistication and power. Compounding this problem are the infectious diseases associated with common mouthpiece use and the substances added with tobacco (flavoured, sweetened tobacco, and many illicit drugs).5–12
The prevalence rate of shisha smoking among university students was 53% in Syria and 31% in Jordan.5,13
Male predominance in smoking behavior is a global phenomenon, with smaller gaps in developed countries and wide but decreasing gaps in developing countries. This is consistent with the epidemiological model proposed by Lopez et al in 1994. 14
Association with age is dynamic and, in most settings, smoking initiation usually occurs during adolescence. Smoking prevalence continues to increase until early or middle adulthood, beyond which smoking declines with age. The reasons for this decline with age are the cumulative impact of smokers quitting and dying prematurely over time.15,16
In Iraq, scientific resources documenting substance use have been scarce and limited information and studies were found. The reasons are mostly related to the low financial and manpower resources allocated for research. The few available published studies were about smoking.
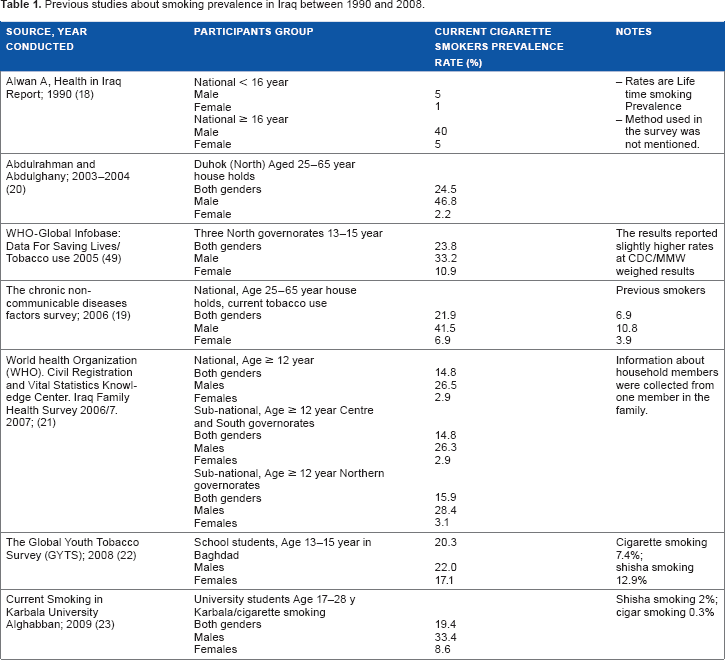
Smoking prevalence in Iraq in the last ten years ranged between 5% and 47% among males and between 1% and 10% among females, as shown in Table 1, which summarises the results of previous surveys conducted in Iraq between 1990 and 2009. The reasons behind these wide ranges are mostly related to the methods used in the surveys. For example, household surveys collect information about all occupants from one person in the family.
Previous studies about smoking prevalence in Iraq between 1990 and 2008.
Because of the profound known harm caused by tobacco, the scarcity of available studies in Iraq, and indices pointing to increasing prevalence, a cross-sectional study was performed to improve the gaps in our knowledge regarding current prevalence and associated demographic characteristics.
Material and Methods
Ethical approval was obtained from the Karbala University Scientific Board before starting the study. All colleges in the University were included in the study.
The study goals were to find the prevalence of tobacco product use among a sample of university students and to improve understanding about the main predictors of smoking and its interaction with other substance use, including alcohol and illicit drugs.
A self-completed questionnaire was designed based on the Global Assessment Programme on drug abuse published in Toolkit Module III. 17 The questionnaire was piloted amongst 20 students in the medical college in the same university and minor corrections performed. Pilot sample results were not included in the main study results.
The required sample size was calculated according to the expected prevalence rate of smoking, which indicated the requirement for at least 1788 students (accepting a 95% confidence interval of two).
All the students in the university are distributed into fixed study halls (lecture rooms). All study halls represented the sampling frame and one third of these halls were chosen randomly. All selected halls were visited by a researcher during lecture hours. An introductory talk asked the students to participate voluntarily in the study, with stress on the anonymity and confidentiality of the study. Participants were informed that completing the questionnaire represented acceptance to participate in the survey.
Univariate and bivariate analysis was done, followed by logistic regression analysis using standard statistical tools (IBM-SPSS-20). As most variables were categorical, a chi-squared test was the main test used to determine statistical significance at a level of p < 0.001. Logistic regression models were used to calculate the odds ratio of predictor variables. All variables having significant association with the main output variables were joined in the models. Some other non-significant variables shown to have an effect in published studies were also included in the models (Table 3).
Results
A total of 2298 students participated voluntarily in the study and the response rate was >99% of the total students in selected halls.
The sample represented approximately one third of the total number of students in the university (approximately 7000 students).
The mean age of the participant students was 21.2 (SD = 2.7 years, CI = 18.4–23.9) and the median was 21 years (Interquartile range 22–24). Females formed 52% of the sample.
The prevalence rate of current smoking was 10.50%, whilst the previous smoking rate was 1%. These rates did, however, differ significantly between colleges. Significant gender difference was found (21% in males, 0.6% in females) and the small number of female smokers was kept in mind during the analysis and the proper statistical tests were applied.
More than one half of the smokers (53%) smoked ≥20 cigarettes daily while one third (35%) smoked ≤10 cigarettes daily. The mean number of cigarettes smoked was 17.6 cigarettes (SD = 10.9) per day and the shisha was smoked at a mean number of 3.4 (SD = 6.3) times per week.
For the type of smoking, it was noticed that cigarette smoking was the main type, used by 57%, while shisha smoking was reported by the rest.
The mean age at which smokers started smoking was 17.5 years (SD = 2.90) with a range of 10–29 years.
The results of bivariate analyses showed that gender and age impose significant effects on smoking (Table 2). In addition, students' smoking was associated with a higher fathers' educational level (p = 0.007), but did not show such association with the mother's educational level.
Current smoking prevalence among different demographic categories of Karbala University students.
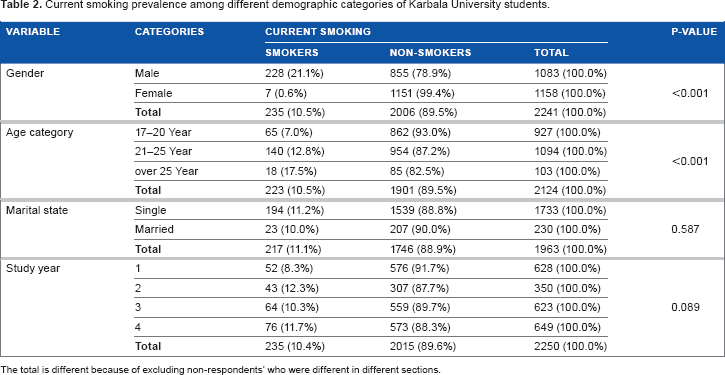
The total is different because of excluding non-respondents' who were different in different sections.
Disapproval of smoking behavior was indicated by the majority of participants, with 10% reporting a positive attitude toward smoking. Similarly, only a minority reported a positive attitude toward alcohol drinking (2%) and illicit drug use (2%). In comparison, smokers had significantly higher proportions of positive attitudes toward smoking behaviour compared to non-smokers (32% vs. 7%, p < 0.001). Smokers had similarly higher positive attitudes towards alcohol drinking (42% vs. 9%, p < 0.001) and illicit drug use (36% vs. 9%, p < 0.001).
A logistic regression model to determine the significant predictors of current smoking was used. Included potential predictors were gender, age category, marital state, parents' educational level, attitude toward smoking, alcohol drinking and illicit drug use. The odds ratio of current smoking was significantly higher among males compared to females (OR = 53.79). Other significant predictors were negative attitudes toward smoking (OR = 0.31) and abstinence from alcohol drinking (OR = 0.05). Some other predictors were not significant (older aged, higher father's educational level and being married) (Table 3). The shisha smoking model showed almost similar findings but it showed a low goodness of fit (p = 0.04).
Odds ratios and 95% CI of significant predictors for current (cigarette and shisha) smoking logistic regression model (reference category non-smokers) among Karbala University students in 2005.

Model fitting chisq (8) = 312.98, P < 0.001. Goodness of fit probability Pearson chisq (139) = 160.07, p = 0.107.
Discussion
The prevalence rate of current smoking was lower than previous survey results, 18 and more recent studies in the country.19–22 A similar sample population in Karbala University studied by Alghabban (2009) reported a higher current smoking prevalence rate of 19%. 23 However, this study had several shortcomings, including administering questionnaires outside study halls (potentially allowing repeat answers by the same student) and covering only two colleges in the university. The estimated number of University students in Iraq is nearly 500,000 so with about 20% lifetime smoking prevalence, there are about 100,000 undergraduate smokers in the country. Additionally, higher prevalence rates of smoking are expected among youths not enrolled in routine education. The serious health and economic consequences of the problem could be estimated and these are expected to be on the increase.
The difference in smoking prevalence might be a real difference or may be related to a difference in the methodology, including the characteristics of the population surveyed and how information was collected. For example, in household surveys, information was obtained from one household member about all members' behaviour.
The smoking prevalence rates found in this study were consistent with other studies in Saudi Arabia and Iran.7,24,25,27 These rates were, however, low in comparison to most studies in adjacent countries, including Jordan, 28 Lebanon, 29 Syria, 30 Egypt, 31 Saudi Arabia, 32 Turkey, 33 and Iran. 6
The difference in smoking prevalence may be related to differences in social context or methodological reasons mentioned for differences with studies in Iraq.
In Eastern Mediterranean Regional Office (EMRO) countries a wide gender gap (4–17 fold) was reported mostly for socio-cultural reasons,34–36 but recent studies have shown that this gap is decreasing.30,37
Cigarette smoking was reported to be the main type of tobacco smoking in most previous studies in Iraq. However, shisha smoking is increasing and this may reflect the wrongly held common belief that it is less harmful than cigarettes. 6
The prevalence of shisha smoking in this study was 4%, whilst the shisha smoking prevalence rate was 2% in both the Alghabban study and in a national survey in Iraq carried out in 2006–7. 19 This was primarily due to the different methodology used, especially as the previous studies were of the general population, whose mean age was higher. Shisha smoking constitutes a growing problem in the Mediterranean region, where higher rates were reported. 4
Globally, the majority of the smokers start smoking before the age of 18, with almost one quarter beginning before the age of 10. 38 Three quarters of the smokers in this study started smoking before 20 years of age, while about half started before 18 years. The high proportion of early starting is mostly related to cheap cost, lack of taxes, lack of prevention of tobacco sale for young persons and uncontrolled advertising. The Ministry of Health and the parliament in Iraq have adopted new prevention regulations, which need to be practically applied.
Alghabban (2009) reported the age of initiation of smoking at 17.02 ± 2.43 years (range 9–22 years) with no significant gender difference and this was similar to the finding in the present study. However, a significantly lower age was found in males in many other studies such as Al-Kubaisy et al (2012) and Maziak et al (2004) in Syria,30,39 and Celikel et al (2009) in Turkey. 40
The association of smoking with higher fathers' education was also reported by Alghabban. 23 A similar association has been reported among university students in many other countries in the region, such as Lebanon, 29 Iran, 27 and Turkey. 34 The explanation of this association possibly relates to the higher socioeconomic level of university graduated fathers, which provides higher financial capability for their children to pay for tobacco. In addition, higher educated fathers may grant more freedom to their children, or this perhaps relates to an unidentified confounding factor. Contrary to this finding, Ozge et al (2006) in Turkey found a reversed negative association. 41 The smoking behavior of parents, siblings and close friends have also been reported to have positive association with smoking,25,37,40,42–48 but these variables were not investigated in this study, because of the need to keep the questionnaire within the limits of the study objectives and ensure a good response rate.
The attitudes toward substance use findings showed that the majority of participants did not approve of any substance use behaviour. These results were similar to studies conducted in Iran and Turkey.27,34
A positive attitude toward substance use might represent the first step to undertake a specific behavior. In addition, substance use behavior has been considered by some researchers to be a spectrum starting at occasional smoking and ending at hard illicit drug use. 50 This finding could explain the positive interaction between different types of substance use found in this study. The confounding influence of attitudes interaction would provide more clear interpretation of the results.
The main strong points of the current study were the use of questions about indicators used in many widely used questionnaires, which allows comparison of the results, and using a wide range of demographic characteristics. Additionally, the high coverage of the university students and the high response rate added to the strength of the study.
Weaknesses include the general weaknesses of self-reported questionnaires, with possible underreporting mostly among females. In addition, the used sampling method spared youths not enrolled in routine education or students absent on the survey day. However, the absenteeism rate was very low and the expected high rate of enrolment in routine education in Iraq reduced the negative effect of these factors. Another limitation was the ignorance of those smoking more than one type of tobacco products.
Future surveys should include questions about peer and parents smoking.
A possible addition of urine or breath testing could have enabled a measure of criterion validity of student reporting of smoking, but this was not feasible due to methodological obstacles including finance and time available.
Conclusion
The prevalence of current smoking was 11% for cigarettes and 4% for shisha, while it was 1% for previous smokers among Karbala University students in Iraq. The high proportion of shisha smokers, similar to the situation across the region, is an alarming risk sign. There was significant positive effect for male gender, increased age, colleges and higher father educational level on smoking prevalence among students. Additionally, significant positive association was found between smoking and other substance use behaviors and positive attitudes toward substance use.
Author Contributions
Conceived and designed the study: AAM. Analyzed the data: AAM. Wrote the first draft of the manuscript: AAM. Made critical revisions: AAM. The author reviewed and approved of the final manuscript.
Footnotes
Acknowledgements
The author would like to acknowledge the help provided by Dr S. Alhasnawi in conducting the study and preparing the questionnaire.
As a requirement of publication the author has provided signed confirmation of compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.