
Abstract
Background:
For health professionals, personal and contextual factors influence addressing patients’ smoking habits. The objective of the study was to describe frequency of addressing patients’ smoking in 2002 and 2014 and to analyse factors related to addressing patients’ smoking habits.
Methods:
Data of physicians from 2 postal cross-sectional surveys were used (n = 4140 in 2002, n = 5666 in 2014). The number of respondents was 2747 in 2002 and 2903 in 2014. The corrected response rate was 67.8% and 53.1%, respectively. Age-standardized frequency of addressing patients’ smoking during the last 7 days was determined. Distribution of other variables along with confidence intervals (CI) was calculated. Logistic regression was used to analyse association of addressing patients’ smoking with attitudes and perceived barriers regarding addressing patients’ smoking and with background factors. Fully adjusted odds ratios (OR) with 95% CIs were calculated.
Results:
The age-standardized prevalence of addressing patients’ smoking habits among men was 84.4% (95% CI 80.3–88.5) in 2002 and 88.3% (95% CI (84.5–92.2) in 2014, among women 82.1% (95% CI 80.2–83.9) and 89.0% (95% CI 87.2–90.8), respectively. According to logistic regression analysis, in 2014, significantly more physicians agreed that it is doctors’ responsibility to convince people to stop smoking (among men, OR 2.32; 95% CI 1.19–4.54, among women OR 1.41; 95% CI 1.06–1.88), that smoking prevention should form part of health professionals’ training, that physicians should have smoking related hand-out materials, and that lack of time was a barrier to addressing patients’ smoking. Addressing patients’ smoking was significantly associated with attitudes and perceived barriers regarding addressing patients’ smoking, age, and other background factors (among women only).
Conclusions:
Addressing patients’ smoking habits was more common in 2014 than in 2002, but the change was significant among women only. Compared to 2002, in 2014 physicians’ attitudes regarding addressing patients’ smoking were more approving. Results of this study are useful for policymakers and institutions involved in organization and development of smoking prevention training and cessation services.
Keywords
Introduction
It is recommended that health professionals screen all patients for tobacco use and provide advice to quit, assistance and follow-up to patients who are tobacco users. 1 A brief advice from a physician on quitting increases quit rates from 2–3% to 4–5% when compared to no advice,2,3 and is seen as an effective use of health care resources when incorporated into routine visits. 4 Delivering smoking cessation advice is especially important among groups with low socio-economic position as nicotine dependence in these groups tends to be higher and intention to quit, lower. 5
In assisting patients with smoking cessation, often the 5 As approach is recommended: asking about smoking; advising to quit; assessing willingness to quit; assisting in quitting; arranging follow-up and support. Yet still addressing patients’ smoking by physicians varies greatly across countries. In Europe, 62% (Netherlands) to 98% (United Kingdom) of general practitioners asked all new patients about their smoking status only during the first visit. Prevalence of routinely asking all regular patients about smoking was lower (28% in Belgium and 63% in England). 6
Physicians’ personal and contextual factors influence addressing patients’ smoking habits. For example, physician’s higher age is associated with being more likely to ask about patients’ smoking. 7 In terms of medical specialty, general practitioners were more likely to ask about patients’ smoking habits. 8 Physicians’ smoking status also plays a role as smoking physicians were less likely to address patients’ smoking habits compared to non-smoking colleagues.6,7,9 Physicians report lack of time8,10,11 and training8,12 as barriers to delivering smoking cessation care. Also, insufficient knowledge 10 and personal attitudes, like finding smoking cessation an important task or feeling comfortable giving smoking cessation related information, affect addressing patients’ smoking.6,10–12
Smoking surveys among physicians in Estonia have been carried out in 1978, 1982, 2002 and 2014. Smoking prevalence among physicians has declined during that time. Among men, the prevalence of current smoking was 20.9% in 2002 and 14.3% in 2014. Among women, the decrease was from 8.0% in 2002 to 5% in 2014. 13 Smoking prevalence among general population in Estonia was higher. Among men, in 2002, 52.2% and in 2014, 39.4% were current smokers. Among women, it was 23.7% and 22.7%, respectively.14,15
In Estonia, since 2000s, the developments in tobacco policy have been substantial. Estonia joined the worldwide Convention on Tobacco Control in 2005. The Estonian Tobacco Act, in its present form was also enforced in 2005 and has been complemented almost yearly. Latest changes included tobacco product display prohibition and forbiddance to use flavoring substances in electronic cigarettes. Also, the smoking cessation services are being further developed and were added to the national health insurance benefits list in Estonia in 2019. Currently there are no national clinical guidelines for smoking cessation services in Estonia. However, a budget impact analysis of smoking cessation interventions was published in 2019. 16 To further promote smoking cessation among population, information on aspects to consider when designing smoking cessation services is needed.
In 2002, about 80% of physicians in Estonia asked about their patients smoking habits at least once a week. The result was similar to their Finnish colleagues at that time. 17 In 2014, the proportion of physicians in Estonia who addressed their patients smoking habits at least once a week was close to 90%. 18 In both years, lack of time was the most reported barrier to addressing patients smoking habits.17,18 Present paper provides insight to changes in addressing patients smoking habits. The objective of this study was to describe frequency of addressing patients’ smoking in 2002 and 2014 in Estonia and to analyse factors related to addressing patients’ smoking habits.
Methods
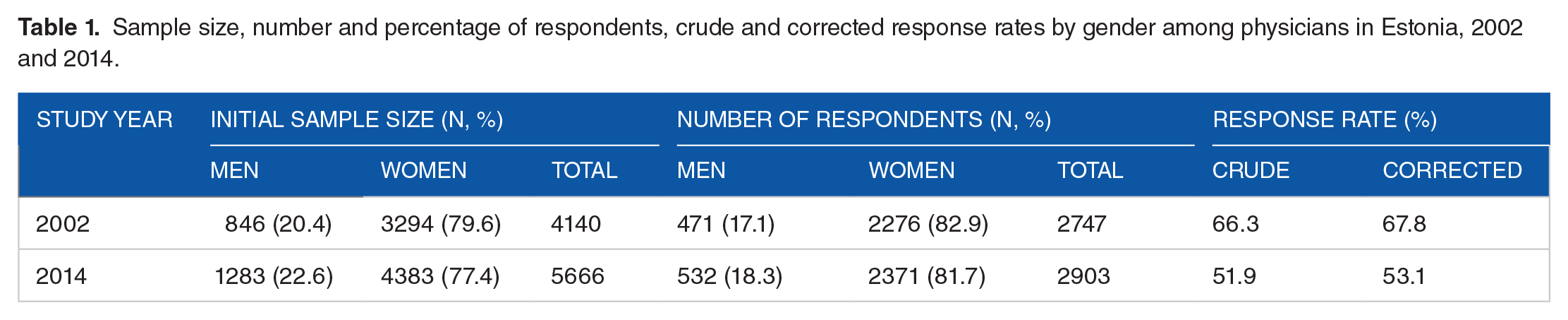
The present study relies on data from postal cross-sectional surveys conducted in 2002 and 2014. All practicing physicians in Estonia were eligible for sampling (n = 4140 in 2002, n = 5666 in 2014; Table 1). In 2002, the physicians’ data were drawn from database of Estonian Health Insurance Fund. The questionnaires were mailed to physicians’ workplace. In 2014, the physicians’ data were drawn from the Estonian Health Care Professionals Registry. The questionnaires were mailed to physicians’ home addresses which were retrieved by linking the data with Population Registry in Estonia. In 2002, 2747 physicians responded and in 2014, there were 2903 respondents. Crude response rates were 66.3% and 52.0%, respectively. Corrected response rates (excluding physicians who were unavailable, retired, had an incorrect address, had left Estonia or had died) were 67.8% and 53.1%, respectively. Present study sample consisted of physicians who were under 65-years old. The questionnaires with answers to the question regarding asking patients about smoking during the last 7 days were included (n = 2488 in 2002, n = 1791 in 2014). There were 7 respondents who reported that their job does not involve the opportunity to ask patients about their smoking habits.
Sample size, number and percentage of respondents, crude and corrected response rates by gender among physicians in Estonia, 2002 and 2014.
Outcome variable
Outcome variable was addressing patients’ smoking. Addressing patients’ smoking was determined with question ‘How often have you asked your patients about their smoking habits during the past 7 days?’ (never, sometimes, every other time, often, always). The answers were dichotomized as never; at least once.
Descriptive variables
Study variables describing factors related to addressing patients’ smoking habits were attitudes regarding addressing patients’ smoking and physicians’ perceived barriers regarding addressing patients’ smoking.
Attitudes regarding addressing patients’ smoking were determined based on agreement (yes, no, cannot say) with following statements: (a) It is the doctors’ responsibility to convince people to stop smoking; (b) Physicians should have smoking related materials to give out to patients if needed; (c) My present knowledge is sufficient to advise a patient who wishes to stop smoking; (d) Smoking prevention should form part of the normal training of health professionals.
Physicians’ perceived barriers regarding addressing patients’ smoking were determined based on the answers (yes, no) to the following questions: (a) Is lack of habit a barrier to addressing patients’ smoking? (b) Is lack of time a barrier in addressing patients’ smoking? (c) Is the wish to respect patient’s privacy a barrier to addressing patients’ smoking?
Background variables
Following background characteristics were considered: gender (male, female); age (measured in full years); ethnicity (self-determined, analyzed in 2 groups: Estonian, non-Estonian); medical specialty (family physician, specialist doctor, dentist); smoking status (current smoker, non-smoker), study year (2002, 2014).
Data for men and women were analyzed separately since there are gender differences in smoking prevalence but addressing patients’ smoking is associated with smoking prevalence. Mean age of physicians was calculated along with standard deviations. A t-test was used to test for differences between mean ages. Distribution of sample by background and descriptive variables was determined. As the mean ages among the sample were significantly different in 2002 and 2014, age-standardized prevalence of addressing patients’ smoking habits was calculated using European standard population, 19 along with confidence intervals (CI). 95% CI was calculated for prevalence of attitudes and perceived barriers regarding addressing patients’ smoking.
Fully adjusted multiple binary logistic regression model was used to analyse association between addressing patients’ smoking habits at least once during last 7 days (yes vs no). and descriptive variables like attitudes and perceived barriers regarding addressing patients’ smoking and background factors. Fully adjusted ORs were presented with 95% CIs. Data were analyzed using statistical package STATA. 20
Results
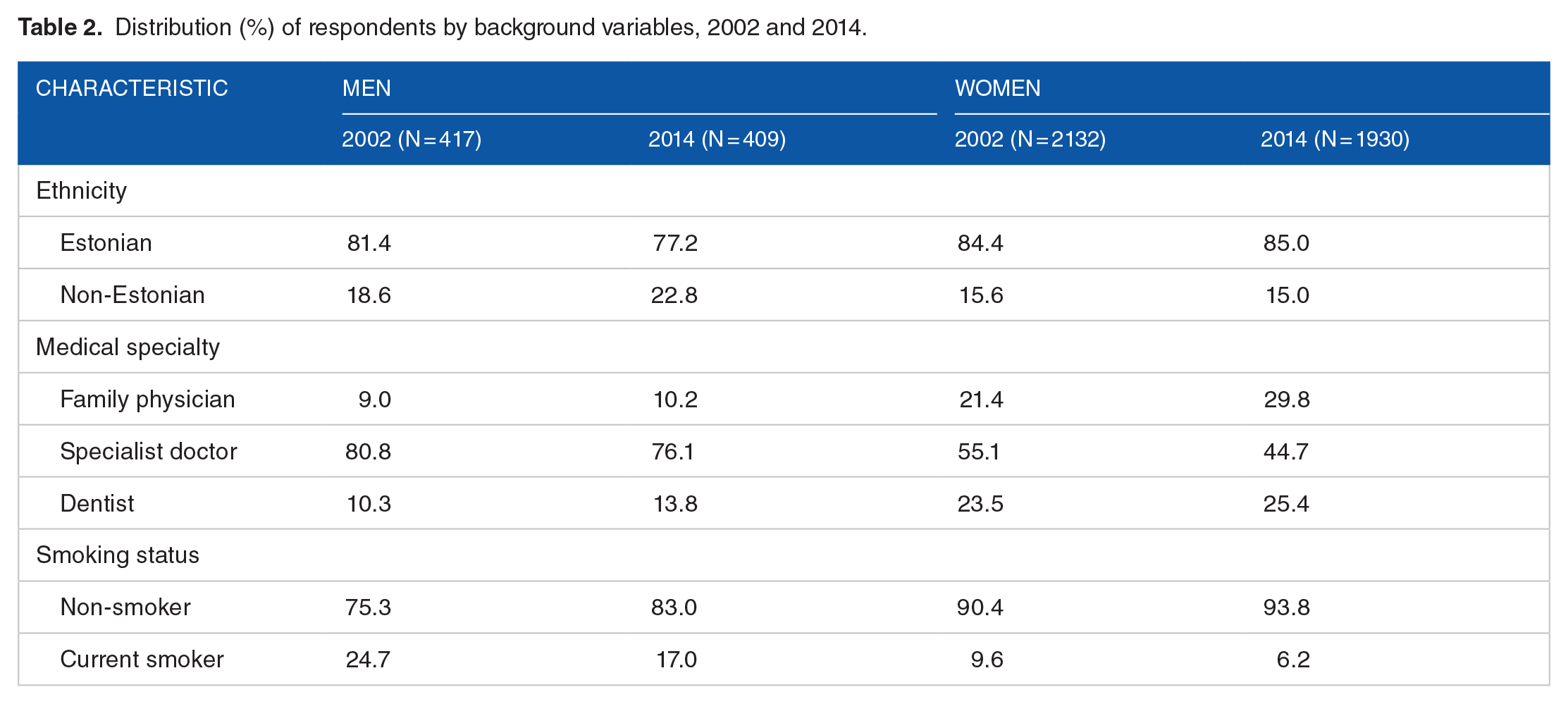
Mean age of men was 45.3 ± 9.8 in 2002 and 46.8 ± 10.9 in 2014 (P = 0.063) and of women 46.3 ± 10.2 and 47.4 ± 11.0 (P = 0.003), respectively. More than 4 fifths of respondents were women (83.7% in 2002 and 82.6% in 2014). In both years, majority of the respondents were of Estonian ethnicity (Table 2). Almost 4 fifths of men and about half of women were specialist doctors. The prevalence of current smoking was 24.7% in 2002 and 17.0% in 2014 among men and 9.6% in 2002 and 6.2% in 2014 among women.
Distribution (%) of respondents by background variables, 2002 and 2014.
Among men and women, the prevalence of addressing patients’ smoking every other time, often and always was slightly higher in 2014 than in 2002. While in 2002, 15.1% of men always asked their patients about smoking, in 2014 the proportion was 16.7% (among women 9.3% and 13.7%, respectively; Figure 1).

Addressing patients’ smoking (%, 95% CI) by Estonian physicians in 2002 and 2014.
The age-standardized prevalence of addressing patients’ smoking habits at least once during last 7 days among men was 84.4% (95% CI 80.3–88.5) in 2002 and 88.3% (95% CI 84.5–92.2) in 2014 and among women 82.1% (95% CI 80.2–83.9) and 89.0% (95% CI 87.2–90.8), respectively.
Among both men and women, in 2014, compared to 2002, significantly more physicians agreed that it is doctors’ responsibility to convince patients to stop smoking, that smoking prevention should be part of the normal training and that physicians should have smoking related materials to give out to patients if needed. Compared to 2002, in 2014 significantly more men and women agreed with the statement that lack of time is a barrier to addressing patients’ smoking (Table 3).
Estonian physicians’ attitudes and perceived barriers regarding addressing patients’ smoking habits, 2002 and 2014.

The results of fully adjusted logistic regression model showed that, among both men and women, addressing patients’ smoking habits was significantly associated with agreeing that it is doctors’ responsibility to convince people to stop smoking and agreeing that physicians should have smoking-related hand-out materials (Table 4). Addressing patients’ smoking was also significantly associated with physicians’ higher age (OR 1.04; 95% CI 1.01–1.07 among men, OR 1.02; 95% CI 1.01–1.03 among women).
Odds of addressing patients’ smoking (yes vs no) among Estonian physicians, 2002 and 2014.

Adjusted to all descriptive variables shown in the table. Significant associations in bold text.
Among women only, addressing patients smoking was significantly associated with agreeing that their current knowledge is sufficient to advise patients who wish to quit, with being unsure whether smoking prevention should be a part of normal training, and with agreeing that lack of time, lack of habit and wish to respect patients’ privacy is a barrier to addressing patients’ smoking. Also, from background factors, addressing patients’ smoking was significantly associated with ethnicity, medical specialty and physicians smoking status among women only. In 2014, women were significantly more likely to address patients’ smoking than in 2002.
Discussion
The study described frequency of addressing patients’ smoking in 2002 and 2014 in Estonia and analyzed factors related to addressing patients’ smoking habits.
Among both male and female physicians in Estonia, the age-standardized prevalence of addressing patients’ smoking habits at least once during last 7 days was higher in 2014 than in 2002. This change was significant among women only. Addressing patients’ smoking has increased among physicians worldwide. For example, while in USA, it was not common for physicians to address patients’ smoking in 1990s and 2000s, 21 then in 2018, 65% of patients were asked about smoking status. 22 In Romania in 2011, more than 80% of patients were asked about their smoking status. 1 In 2009–2010, in Poland, 57.2% and in Russia, 45.4% of patients reported that they were asked if they smoked by a health care provider. 1 The current paper explores changes in addressing patients’ smoking in 2002 and 2014. During this period, the tobacco policy in Estonia went through considerable changes. For example, Estonia joined the worldwide Convention on Tobacco Control in 2005. Reducing tobacco use has been agreed in the National Health Plan and incorporated to other policies and actions. As the awareness of the harms of smoking increased, more attention was paid to promote smoking cessation.
Compared to 2002, in 2014, the agreement that it is doctors’ responsibility to convince people to stop smoking, that smoking prevention should be part of the normal training and that physicians should have smoking related materials to give out to patients if needed, was significantly higher. This indicates a need for more comprehensive training in smoking cessation for physicians. Currently, tobacco control is included in the curriculum of medical students but is covered under different subjects.
Compared to 2002, the proportion of physicians who agreed that lack of time was a barrier to asking patients about smoking was significantly higher in 2014. Lack of time is one of the most common barriers doctors report when asked about addressing patients smoking habits8,10,11,23 thus being a challenge to organization of smoking cessation and other preventative care services. To overcome this challenge, for example teamwork based approach should be used. Especially in primary health care, nurses should be trained to provide brief advice. At the same time, no significant change between study years was found in the agreement that lack of habit or wish to respect patient’s privacy were perceived as barriers to addressing patients’ smoking. As the agreement with both statements was relatively low, this finding shows that perceived barriers to addressing patients smoking are mostly related to practical issues rather than with attitudes.
The results of adjusted logistic regression model showed that among both men and women, addressing patients’ smoking habits was significantly associated with agreeing that it is doctors’ responsibility to convince people to stop smoking and agreeing that doctors should have smoking related hand-out materials. Previous results from a study based on Estonian physicians smoking survey showed physicians in Estonia agreeing that it is important to reduce smoking among the population. 24 Present study results complement this information by showing that physicians were ready to intervene.
Among both men and women, physicians’ higher age was significantly associated with higher likeliness to address patients’ smoking. Previous studies also showed that more senior physicians were more likely to ask about patients’ smoking. 7 Offering advice on smoking cessation has also been associated with having longer work experience 12 suggesting that when smoking cessation counseling is needed, the patient should be referred to more experienced physicians.
Among women, addressing patients’ smoking was significantly associated with physicians agreeing that their knowledge is sufficient to advise on smoking cessation and that smoking prevention should be part of normal training. These results pose questions about whether the associations between addressing patients’ smoking and attitudes regarding addressing patients’ smoking were simply more expressed among women or were some associations left undetected because of the smaller number of men in the study sample. The latter would be more likely as in current sample, more than 80% were women. The gender distribution among physicians’ general population in Estonia was similar to the study sample in both years.
Also, among women, addressing patients’ smoking was significantly associated with perceiving lack of time and wish to respect patients’ privacy as barrier to addressing smoking habits. The results of current study reflect physicians’ readiness to intervene but also a pro-active approach which is crucial in overcoming barriers to addressing patients’ smoking. However, the results also indicate the opportunity to better organize smoking cessation services. For example, how and when brief cessation advice should be provided, when to refer to counseling or how these tasks would be best distributed between different levels of health care or within the team of specialists involved in the service provision. As in the current study, the sample consisted only of physicians, there is no information on how much nurses were involved in smoking cessation in different levels of care.
Among women only, addressing patients’ smoking was significantly associated with ethnicity, medical specialty, smoking status, and study year. Cultural background has been associated with being more likely to provide cessation advice. 7 However, in the context of present study, the possible reasons might be related to other factors, like, for example, age, and would need a more detailed exploration. Non-smoking women were significantly more likely to ask patients about smoking compared to current smokers. The fact that physicians who are smokers, might more often fail to address patients’ smoking habits, has also been reported in studies elsewhere.6,25 Compared to dentists, family physicians and specialist doctors were significantly more likely to address patients’ smoking habits. Studies have previously shown that the most common setting for smoking cessation advice is primary care and that family physicians were more likely to ask patients about smoking.2,8,26 The results of the logistic regression model confirmed the findings of prevalence of addressing patients’ smoking – in 2014, women were significantly more likely to ask about patients’ smoking habits than in 2002.
The limitations of current study include, firstly, survey response rates of 67.8% in 2002 and 53.1% in 2014. The response rates in postal surveys conducted among health professionals were predicted to decline already in 2009. 27 Low response rates might lead to non-response bias. However, in present study, the eligible sample consisted of all practicing physicians, and the respondents were similar to physicians’ population in terms of gender distribution of doctors in Estonia. Secondly, the study data was drawn from self-reported surveys. In the context of present study, this poses a possible bias since information on addressing patients’ smoking relies on recalling and not on observation. Also, data concerning smoking status might be underestimated because physicians might be prone to giving socially acceptable answers like for example underreporting on their smoking habits. Thirdly, the mean ages of the sample were significantly different in 2002 and 2014. To alleviate the possible effect related to this, age-standardization was used. Despite these limitations, Estonian physicians smoking survey serves an excellent opportunity to analyse attitudes and perceived barriers regarding addressing patients’ smoking among a homogenous group as the similarity of survey questions in 2002 and 2014 allowed to make comparisons.
Conclusions
Majority of Estonian physicians addressed patients’ smoking habits at least once in last 7 days in 2014. Compared to 2002, the prevalence of addressing patients’ smoking was higher among both genders in 2014, but the change was significant among women only. Among both men and women, addressing patients’ smoking habits were significantly associated with attitudes regarding addressing patients’ smoking, and physicians’ age. Among women only, addressing patients’ smoking was associated with ethnicity, medical specialty, smoking status, and study year. Results of the present study are useful for policymakers and other institutions involved in organization and development of smoking prevention training and cessation services.
Practice implications
Further training in smoking prevention is needed to enable physicians to routinely address patients’ smoking. In development of smoking cessation counseling services in Estonia, factors related to addressing smoking habits should be considered. For example, barriers to asking about patients’ smoking could be addressed by developing best practice guidelines to normalize attending to patients’ smoking habits. Smoking cessation counseling could be further organized by introducing teamwork-based approach, for example involving nurses in such preventive services.
Footnotes
Acknowledgements
The authors thank the entire team involved in designing and conducting the survey in 2002 and 2014.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The design of the Estonian physicians’ smoking survey and the collection, analysis, and interpretation of the data were supported by the Estonian Research Council (grant numbers PUT-299, IUT34-17).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
MP: performed the statistical analysis, interpreted the data, drafted the manuscript and has been involved in revising the manuscript critically. KP: made a substantial contribution to the conception and the design of the study, interpreted the data and has been involved in revising the manuscript critically. Both authors have read and approved the final manuscript.
Ethics approval and consent to participate
The surveys in 2002 and 2014 were approved by the Research Ethics Committee of the University of Tartu (decisions no. 87/1 and 235/T-12, respectively). An informed consent form including a description of the study design and how the collected data would be used was sent to the recipients with the questionnaires. The form explained that participation in the study would be considered to constitute consent. Additional written consent was not obtained.
Consent for publication
Along with the questionnaires, the recipients were sent a description of the study design and an explanation of how the collected data would be used. Respondents were informed that participation in the study would constitute consent.
Availability of data and materials
The datasets used and analyzed during the current study are available by request from Kersti Pärna.