
Abstract
Background
Elderly men and women who smoke for many years are more likely to sustain fractures after minimal trauma than are nonsmokers. The two major risk factors for fractures are low bone mineralization density (BMD) and a propensity for falling in smokers known to have poorer neuromuscular function compared with nonsmokers. Smokers are weaker and have poorer balance, gait, and integrated physical function. Older people who smoke cigarettes have significantly lower BMD than those who do not. Cadaveric studies show that a decrease of BMD by 10% results in decrease of bone strength by three-fold. Thus, it is reasonable to expect an increased incidence of fractures among smokers on the basis of BMD level alone.
Aim
The aim of the study is to find the effects of cigarettes smoking on the time of healing in comparison with nonsmoker patients with colles fracture.
Patients and Methods
A cross-sectional study was done in AlKindy Teaching Hospital, AlKarkh General Hospital, and AlJarah Private Hospital in the period between March 1999 and February 2006.
280 patients with colles fracture were included and divided into two groups (smokers and nonsmokers).
Age, sex, causes of the trauma type of the fracture, number of cigarettes smoking, body mass index, time of healing and others were studied.
Results
Group A
Male to female ratio was 1:2.29.
The commonest age group was between (60–69) years 64.3%.
Body mass index (BMI), 50% of patients were within 20–24 score and 25% were within 25–29 score.
The type of fracture was 86.6% displaced fracture.
The time of healing was 61.6% within 4 weeks and 33.93% healed within 5–6 weeks.
Group B
Male to female ratio was 1:2.36.
The commonest age group was 50–59 years 52.4.
The type of fracture was 86.9% displaced.
Regarding BMI, 51.2% of patients were within score less than 20, and 34.5% were within 20–40 score.
The time of healing was 67.3% within 5–6 weeks and 18.5% healed within 4 weeks.
Conclusion
Cigarette smoking increases the time of healing in elderly individuals with colles fracture.
Introduction
Since the release of the first surgeon general report on smoking and health in the united states in 1964, about 10 million people have died from smoking-related diseases e.g. heart disease, lung cancer, emphysema and other respiratory diseases. If current smoking patterns continue, an estimated 25 million Americans will die prematurely from a smoking-related illness, 1 according to a 2003 report, an estimated 23.4% of adult Americans smoke. The risk varies by age, ethnic group and geographic location. 2
Cigarettes presumably contain over 4,000 chemicals, of which only 109 known chemicals including, nicotine, benzene, tar, etc which harm the individuals. Nicotine has a significant negative role on musculoskeletal system, it causes peripheral vasoconstriction, tissue ischemia, decrease oxygen tension, and also it depresses osteoblastic activity. 3
Smoking also lowers bone mineral density due to decreased calcium absorption associated with secondary hyperparathyroidism and increased bone resorption. 4
Studies have shown that the numerous toxins contained in cigarette smoke can undermine fracture and ligament repair following injury. In addition, fracture healing problems and bone infections and smoking have been shown to impair soft tissue wound healing.
Studies funded by the national institutes of health examined the effect of smoking on fracture and ligament healing in mice and found that healing of both types of injuries were delayed. 5
The effect of smoking on hip fracture is most evident among thin, elderly women. Forsen reported that among female smokers older than 50 years showed increase risk of such fracture by 50%, the risk increased three-folds among smokers than nonsmokers. 6
Smokers are not only more susceptible to fracture, but also more likely to have recurrent fractures. 6 Healing of fractures is delayed in smokers due to the abnormal maturation of the regenerating bone thus nonunion or malunion is more frequent. Smoking impairs formation of new bone, and women who smoke are at high risk for loss of bone density and osteoporosis. 7 Postmenopausal women who smoke have a significantly greater risk for hip fracture than those who do not. 7 Older men and women who have smoked for many years are more likely to sustain fractures after minimal trauma than are nonsmokers. Fracture occurs most frequently at the hip, wrist and spine, but any bone with low BMD\is more susceptible to fracture. The two major risk factors for osteoporotic fractures are low BMD and a propensity for falling in smokers known to have poorer neuromuscular function compared with nonsmokers. 8 Another study showed that moking alone does not increase the frequency of falling in elderly or the likelihood of injury after falling. 9
Evidence regarding the relationship between cigarette smoking and wrist fractures are limited. Among thin women who had never taken postmenopausal estrogen, the risk of forearm fracture was found to be more than five-fold greater among smokers than among non-smokers. 10 Estrogen use was highly protective in this group of smokers. Among women who had used estrogens as a replacement therapy the risk of fracture was not associated with either cigarette use or body weight. 11
Cigarette smoking is the most preventable cause of premature death, and is responsible for one in five deaths from all cause. Millions of other people are living with serious illnesses caused by smoking. Smoking has been linked with many health problems including the array of orthopaedic conditions and complications. 12 Colles fracture is a fracture–-dislocation of the lower radio-ulnar joint which is first described by Abraham Colles of Dublin in 1814. Mechanism of injury includes falling onto the outstretched hand. The deformity includes fracture of lower radius, fracture ulnar styloid, and dislocation of inferior radio-ulnar joint. 13
The aim of the study is to find the effect of smoking on the prevalence of fractures and the time of healing of Colles fracture patients in comparison with non-smokers.
Patients and Methods
A cross-sectional study was done in Al-Karkh General Hospital, Al-Kindy teaching hospital, and Al-Jarah Private Hospital in the period between March 1999 and February 2006. A total number of 280 patients with colles fracture.
All treated conservatively using the same regiem of treatment. The patients were divided into two groups depending on cigarettes smoking.
Group A included 112 non smoker patients while group B included 168 smoker patients. A special questionnaire forma arranged for this purpose, included age, sex, cause of trauma, type of fracture, body mass index, number of daily cigarettes smoking per day (Group B), time of healing, and other aspects of the disease. Statistical analysis was done using Mini Tab soft ware, version 13. Descriptive statistics includes frequencies, percentages, and tables. Inferential statistics includes chi square, test. P value <0.05 considered to be statistically significant.
The Results
Out of 280 patients, males outcome females with a male to female ratio of 1:2.33.
In Group a (None-Smokers group)
male to female ratio was 1:2.29 (Table 1).
Age–-sex distribution.
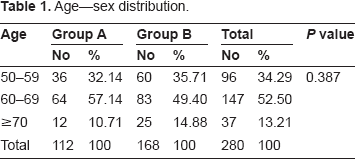
The commonest age group was between (60–69) years 64.3%. The least was (70–79) and (80–89) years, (2.68% and 1.8%) respectively (Table 1).
The cause of trauma was falling on outstretched hand in 85.7% while road traffic and motorcycle accidents accounts 10.7%, and other causes results in 3.6% of fractures (Table 2).
Sex distribution.

4-Regarding body mass index (BMI), 50% of patients were within 20–24 score and 25% were within 25–29 score (Table 4).
The types of fracture were displaced fractures in 86.6%, while in 13.4% were impacted. Comminuted fractures were excluded from the study. Table healing of fractures occurs within 4 weeks in 61.6% while 33.93% healed within 5–6 weeks (Table 6).
While Group B (Smokers group)
Male to female ratio was found to be 1:2.36.
The commonest age group was 50–59 years 52.4% and 60–69 years in (39.3%) (Table 1).
The cause of trauma was in 88.7% due to fall on outstretched hand and 6.54% due to road traffic and motorcycle accidents (Table 2).
The type of fracture was 86.9% displaced while 13.1% impacted fracture (Table 3).
Causes of trauma.

Type pf Colle's fractures.

BMD.
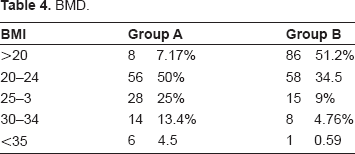
Regarding BMI, 51.2% of patients were below 20 and 34.5% were within 20–24 (Table 4).
Regarding the smoking level, 52.38% of patients, smoke 21–25 cigarettes per day and 13.1% smoke 10–15 per day (Table 5).
No. of cigarette per day.


The time of healing was 67.3% within 5–6 weeks and 18.5% healed within 4 weeks (Table 6).
Discussion
Colles fractures is common in elderly and mostly affect females due to fall on outstretched hand, this is similar to the finding in this study (Tables 1, 2). If we compare the incidence of fracture in both groups we found it is common in age group (60–69) in group A and (50–59) in group B also in Table 4 the incidence is common among thin patients with BMI score of less than 20 in group B patients we reach to the same results of some studies.
Mckee, et al 14 have done retrospective review of 84 patients who underwent Ilizarov 15 reconstruction to determine the effect of smoking on outcome and complication rates following Ilizarov reconstruction. 16 There was a higher incidence of nonunion in the smoking group. 17 They concluded that smokers has a higher percentage of poor results due primarily to higher complication rates. 18
Smoking is a significant potentially remediable risk factor for failure following Ilizarov reconstruction and cessation strategies are of paramount importance prior to initiating treatment.
While the first suggestion of an association between tobacco smoking and osteoporosis was published in 1976,19,20 several studies have examined the effect of tobacco smoking on bone mineral density and risk of fracture. Smoking is widely considered a risk factor for future fracture. Several biological effects of tobacco may influence the risk of fracture in smokers. Smoking may exert adverse effects on bone strength through direct toxicity of nicotine and non-nicotine components of cigarette smoke on bone cells, as demonstrated in vitro.21,22 Further, smoking may indirectly affect bone strength through decreased intestinal calcium absorption, 23 increased metabolism or decreased production of oestrogen, 24 and through hypercortislism. 25 In addition, smoking may influence the fracture risk through other mechanisms unrelated to osteoporosis, such as poorer balance and physical performance due to neurovascular and peripheral vascular deleterious effects of smoking. 26 Nicotine can counteract the antioxidant effects of vitamins C and E and lead to a significantly higher risk of bone fracture. Recent meta-analyses on the effects of smoking on the bone revealed that current smokers sustained decreased bone mass and increased fracture risk at age 50 years and older. These relationships remained significant after adjustment for the effects of age years since menopause and body weight regardless of sex. The raised risk of fractures was observed to be consistent at all sites. 27
Cigarette smoking is a risk factor for fracture among postmenapausal women, risk decreases after cessation. 15
A meta-analysis based on these studies recently concluded that postmenapausal bone loss is greater in smokers than in nonsmokers and that tobacco smoking increases lifetime risk of high fracture in women by about 50%. 16
BND is low in patients above 50 years especially in women due to many factors like osteoporosis, low estrogen level, etc. Association between BMD, smoking, and risk of fractures was studied. 15 The low BMD accounted for only 23% of the smoking-related risk of fracture. For fractures associated with osteoporosis; the risk ratio increased with age.
In Table 6 we found that the time of healing in group A is different from that in group. About 61.6% of nonsmoker group healed within first 4 weeks while 33.93% healed within 5–6 weeks, in smoker group we found 67.3% healed in 5–6 weeks and 18.5% healed within 4 weeks, also 11.3% within 7–8 weeks and more commonly occurs among women, this mostly due to the effects of tobacco in different ways.
In one study smoker had a significantly higher rate of nonunion than did nonsmoker (18.6% vs. 7.1%). However, the long-term, heavy smoker who have permanent artery damage due to smoking. Delayed or impaired healing of skeletal trauma in patients who smoke has been attributed to vascular responses of nicotine absorption and or a direct effect of nicotine or other smoke components to bone cells in vivo studies indicate variability in osteosynthetic response to nicotine versus smoke inhalation. It has been hypothesized that components of cigarette other than nicotine may be responsible for the adverse skeletal effects of smoking.
The pathophysiological effects are multidimensional, including arteriolar vasoconstriction, cellular hypoxia, demineralization of bone, and delayed revascularization. Nicotin seems to play a significant role in causing the lack of oxygen to the tissues. Research has begun to accumulate evidence linking smoking to difficulty in healing fractures. It has found that smokers have a significant deficiency of oxygen (hypoxia) at the cellular level where the fracture is trying to heal. Fractures heal normally in areas which have good blood supply in the region of the fracture, smoking cessation increased healing rates to near those of nonsmoker. 13
In Table 5, we found 88 patients 52.38% smoke 21–25 cigarettes per day and this reflects the relationship of the number of cigarettes to the prevalence of the fracture among the smokers and the time of healing.
In a recent study done, it was found that smoking has independent, dose-dependent effects on bone loss, which increases fractures risk, and may be partially reversed by smoking cessation. 13 Given the public health implications of smoking on bone health, it is improved that this information be incorporated into smoking prevention and cessation efforts. 19
Conclusion
Cigarette smoking increases the time of healing in elderly individuals with colles fracture.
Footnotes
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author and peer reviewers of this paper report no conflicts of interest. The author confirms that they have permission to reproduce any copyrighted material.