
Abstract
Introduction
Tobacco use remains a significant public health concern worldwide due to its well-established health, economic, and environmental consequences.1-3 Tobacco, whether smoked or used in smokeless forms, causes millions of deaths and illnesses every year. In 2019 alone, more than 8 million people died from tobacco-related diseases such as lung, head and neck, esophageal, and bladder cancers. 4 Cardiovascular diseases, diabetes, and chronic respiratory diseases are also significant contributors to the death toll attributed to tobacco use. 4 The annual death toll linked to tobacco use is expected to continue rising even if the rates of tobacco use decline, as tobacco slowly kills its users and those exposed to its emissions.5,6
Tobacco use has been declining in both males and females globally. 6 According to WHO data from 165 countries, approximately half of men (49.3%) aged 15 years and older were using tobacco in 2000. 7 By 2020, this proportion had declined to 36.7%, and it is projected to further decrease to 34.3% by 2025. 7 The decrease in tobacco use has been attributed to the implementation of tobacco control interventions in WHO member states, which are guided by the WHO Framework Convention on Tobacco Control (FCTC), 8 state laws, and the 2013-2020 Global Action Plan for the Prevention and Control of Non-communicable Diseases (NCD GAP) that focuses on reducing the global prevalence of tobacco use (both smoked and smokeless) by 30% by 2025 compared to 2010. 9
Despite the global decline in tobacco use, developing countries in sub-Saharan Africa (SSA) are experiencing more severe consequences of tobacco use, exacerbated by additional burdens such as malnutrition and infectious diseases. 10 The region’s weak health care systems further strain its ability to manage tobacco-related diseases. 1 This combination of factors highlights the urgent need for further targeted interventions and support to mitigate the impact of tobacco use in SSA and address the broader health challenges facing these countries. 11
Tanzania is among the leading tobacco producers in SSA, utilizing 15% of its arable land for tobacco cultivation.12,13 Most of this production (90%) is for the export market, with the remaining 10% designated for the domestic market. 12 In 2012, Tanzania’s tobacco output reached 126,600 tonnes, making it the country’s second-largest export crop and contributing approximately 30%–35% of its annual exports. 14 Despite the monetary benefits of the tobacco industry, Tanzania has recognized its health, economic, and environmental consequences. Consequently, the country ratified the FCTC in 2007, along with its earlier Tanzania Tobacco Act of 2003 and its regulations of 2014, which serve as the foundation for the nation’s tobacco control policy. 12
Despite national efforts along with widespread campaigns on the consequences of tobacco, tobacco consumption persists among both males and females in Tanzania.15-17 Recent evidence from a tertiary cancer-specialized hospital also indicated that 25% of patients with esophageal, head and neck cancers were tobacco users. 18 Further evidence from the 2018 Global Adult Tobacco Survey (GATS) revealed that overall tobacco use (including smoking and/or smokeless forms) among adults aged 15 years and above was 8.7%. Males accounted for 14.6% of users, while females represented 3.2%, resulting in approximately 17,200 tobacco-associated deaths annually. 12 With the increasing population in Tanzania, this death toll is expected to continue to increase yearly if comprehensive tobacco control programs are not fully implemented. 11
Numerous factors have been linked to tobacco use in populations of various demographics, including age, sex, educational status, marital status, geographical disparities, religion, socioeconomic status, alcohol consumption, and exposure to mass media.19-22 However, there is a paucity of this evidence from the Tanzanian male population, which is known to lead tobacco use by almost 5-fold compared to women in the country. 12 To address this knowledge gap, we aimed to determine the prevalence and factors influencing tobacco use among men in Tanzania utilizing data from the latest Tanzania Demographic and Health Survey and Malaria Indicator Survey (2022 TDHS-MIS). By leveraging this nationally representative dataset, we sought to provide valuable insights into the factors influencing tobacco use among men aged 15-49 years. The findings of this study are intended to contribute evidence that can help policymakers and the public health sector design and implement more effective strategies tailored to the needs of the Tanzanian population.
Methods
Study Design
This was a cross-sectional analysis of the 2022 TDHS-MIS. The 2022 TDHS-MIS is a nationally representative survey that collected information on different health indicators among adult Tanzanians aged 15-49 years.
Study Population and Sample Design
The sample design for the primary survey is detailed in the 2022 TDHS-MIS final report. 23 Briefly, the 2022 TDHS-MIS used a two-stage sample design. In the first stage, 629 enumeration areas (EAs) were selected using a probability proportion to size method, with 211 in urban and 418 in rural areas. In the second stage, 26 households were systematically chosen from each cluster, resulting in a total of 16,312 households. Of the 16,312 households selected, 15,907 were found to be occupied. Among the occupied households, 15,705 were successfully interviewed, resulting in a response rate of 99%. In the subsample (50% of households) selected for the male questionnaire, 6367 men aged 15-49 years were identified as eligible for individual interviews, of whom 5763 were successfully interviewed, yielding a response rate of 91%.
Study Variables
Dependent Variable
The dependent variable for this study was “tobacco use”, which is a self-reported measure of recent consumption of any tobacco product in the past 30 days. An individual was defined as a tobacco user if he reported having smoked or used smokeless tobacco products. The smoked products included manufactured cigarettes, hand-rolled cigarettes, kreteks, pipes full of tobacco, cigars, water pipe sessions, and others. The smokeless products included snuff by mouth, snuff by nose, chewed tobacco, and betel quid with tobacco.
Independent Variables
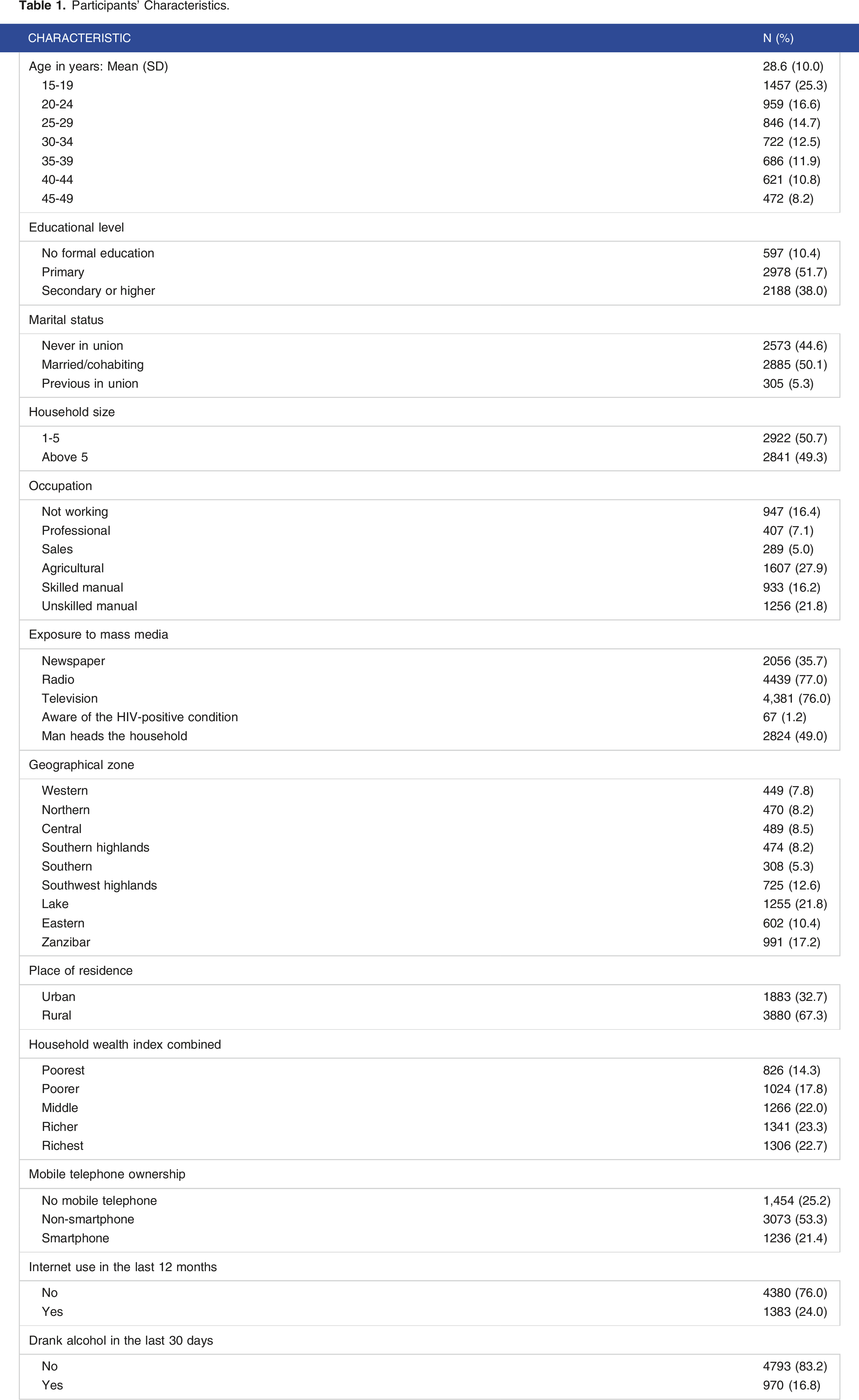
Different independent variables were identified in the literature, and their availability within the 2022 TDHS-MIS dataset was checked. These included age, educational level, marital status, household size, occupation, place of residence, exposure to mass media, household headship, HIV status, household wealth index, telephone ownership, internet use, alcohol consumption, and geographical variations.
Statistical analyses
The data were analyzed using STATA version 18. 24 A descriptive analysis was performed to summarize participants’ characteristics and patterns of tobacco use. The data were weighted using individualized weights and adjusted for clusters and strata to account for the complex sample design employed by the 2022 TDHS-MIS. Both bivariate and multivariable logistic regression analyses were performed to assess the independent variables associated with tobacco use. All variables with P < .2 in the bivariate analysis were included in the multivariable model. Crude odds ratios (ORs) and adjusted odds ratios (aORs) with their corresponding 95% confidence intervals are presented. A P-value of <.05 was considered to indicate statistical significance.
Ethics Approval and Consent
This study used secondary data that is publicly available. 23 Therefore, no formal ethical approval was needed. However, the 2022 TDHS-MIS was conducted after approval from national and international review boards, including the National Institute of Medical Research, the Zanzibar Medical Research Ethical Committee, the Institutional Review Board of the Inner City Fund, and the Centers for Disease Control and Prevention in Atlanta. All participants interviewed were requested to provide verbal informed consent before the commencement of the study. According to DHS program, “verbal informed consent is sought by the interviewer reading a prescribed statement to the respondent and recording in the questionnaire whether or not the respondent consented (or provided assent on behalf of minors). Then the interviewer signs his or her name attesting to the fact that he/she read the consent statement to the respondent”. Thus, in the 2022 TDHS-MIS, the respondents were not asked to sign their name as the interviewer had attested that proper procedures were followed.
Results
Participant Characteristics
Participants’ Characteristics.
The Prevalence of Tobacco Use
The unweighted prevalence of tobacco use was 11.1% (95% CI 10.3%-11.9%), and this proportion remained unchanged after weighting the data to account for cluster sizes and strata in the 2022 TDHS-MIS (adjusted prevalence 11.1%, 95% CI 10.1%-12.3%). Of the 639 tobacco users, 607 (95%) reported smoking different tobacco products, 109 (17.1%) reported consuming smokeless tobacco products, and 77 (12.1%) reported to have consumed both smoked and smokeless tobacco products.
Distribution of Daily Tobacco Product Use (N = 639).

Factors Associated With Tobacco Use
Results of Bivariate and Multivariable Logistic Regression Analysis for the Factors Associated With Tobacco Use.

Discussion
This study provides the first nationally representative estimates of tobacco use prevalence (smoked and/or smokeless) and associated factors among Tanzanian men aged 15-49 years, utilizing data from the 2022 TDHS-MIS. Our analysis revealed that 11.1% of respondents were current tobacco users. Among all tobacco users, approximately 95% of men had smoked various tobacco products, 17.1% had consumed smokeless tobacco products, and 12.1% had consumed both smoked and smokeless products. These findings suggest a significant prevalence of tobacco use among Tanzanian men, with smoking being the predominant form. The observed prevalence underlines the necessity for further targeted tobacco control interventions in Tanzania, focusing primarily on smoked tobacco products.
The prevalence of tobacco use in this study was slightly lower than the 14.6% previously reported by the GATS in 2018. 12 This slight decline in prevalence could be attributed to the success of tobacco control programs 25 and increased awareness of tobacco use among Tanzanian men. Another possible factor contributing to this difference could be the differences in the study populations. While the 2022 TDHS-MIS, on which this study is based, included only men aged 15-49 years, the GATS included men aged over 49 years as well. However, the tobacco use prevalence among Tanzanian men in this study was slightly greater than that among men in Haiti (9.8%) 26 and lower than that reported from nationally representative surveys among men in Uganda (15.9%), 19 India (45.5%), 27 and Nepal (52.3%). 20 These variations between countries may reflect cultural disparities and differing tobacco use policies.
Age was identified as an independent factor associated with tobacco use in this study. We found that men in older age groups had greater odds of reporting tobacco use than those in lower age groups. One possible explanation for this finding could be that aging is associated with numerous stressors, including health issues, financial concerns, or the loss of loved ones, which may prompt individuals to turn to substance use, such as tobacco, as a coping mechanism. Additionally, older individuals may have been using tobacco for a longer period without intervention, leading to a greater likelihood of continued use. Our finding aligns with several studies conducted in East Africa19,21 and Asia.20,27 This finding highlights the importance of targeted smoking cessation programs, improved access to counseling services, and heightened awareness and education regarding the health risks associated with tobacco use among older men.
Higher educational attainment was found to be negatively associated with tobacco use in this study. Men with at least a secondary education had lower odds of tobacco use than those with no formal education. This could be because individuals with higher educational levels have a greater awareness of health risks, making them less prone to risky behaviors such as tobacco use. Additionally, higher educational levels are often linked to better access to information on the harms of tobacco use and resources such as smoking cessation programs, which can facilitate quitting or avoidance of tobacco. These observations emphasize the significant role of education in shaping men’s attitudes and behaviors related to tobacco use. Our findings align with similar trends observed in several developing countries in Africa19,28-30 and Asia.20,27,31,32
Consistent with previous studies,22,30,33 occupation type was found to be a predictor of tobacco use in this study. We observed that men who were not working (i.e., not having an occupation during the survey period) had lower odds of tobacco use than men working in various occupations. The category of men identified as not working is more likely to comprise disabled individuals and those with chronic health conditions that make them unable to work. These groups may have limited financial resources, which could make it more challenging for them to afford tobacco products. Consequently, they may be less likely to initiate or maintain tobacco use compared to those with steady incomes. Men who have no occupation may also have fewer opportunities to be exposed to peer pressure to use tobacco, further reducing their likelihood of starting or continuing tobacco use.
Men who were heads of household exhibited lower odds of tobacco use than those who were not. This observation can be attributed to the socioeconomic responsibilities and role modeling inherent in being the head of a household. 34 Men in these roles may be more inclined to prioritize their health and avoid tobacco use to set a positive example for their household members. Additionally, heads of household are likely more conscious of the financial strain that tobacco use can impose on the family budget, thus motivating them to avoid tobacco to allocate funds for other household needs. 35 Furthermore, these men may have greater access to information and resources, such as health education programs or smoking cessation services, which can facilitate tobacco avoidance or cessation. These findings underline the significance of household headship among men in sharping positive behaviors. However, further studies are warranted to decipher how household headship influences tobacco use behavior.
Geographical disparity emerged as another significant factor associated with tobacco use in our study, consistent with findings reported in other populations.21,27,36-38 Our analysis revealed that men residing in the Southern Highlands zone exhibited lower odds of tobacco use, while those in Zanzibar and the Eastern zone exhibited greater odds of tobacco use. One possible explanation for our results lies in cultural norms and traditions, which influence the social acceptability of tobacco use. Smoking could be more socially accepted in the Eastern zone and Zanzibar than in the Southern Highlands zone because the Eastern zone and Zanzibar lie along the Indian Ocean, facilitating interactions among people from different cultural backgrounds, including foreigners. These multifaceted interactions between culture and tobacco use encompass a broad spectrum of influences, ranging from traditional customs and societal norms to modern-day trends and global influences. Thus, additional efforts are needed to understand the interplay between cultural dynamics and tobacco consumption.
Men from households with the poorest wealth index were more likely to use tobacco than those from middle-wealth index households, aligning with findings from several studies in developing countries.21,27,37 Individuals from the poorest households often face higher levels of stress due to financial uncertainty, lack of resources, and other socioeconomic challenges. In response to this stress, some individuals may turn to tobacco use as a coping mechanism, seeking temporary relief or distraction from their problems. This finding was not surprising because there is an established relationship between poverty and tobacco use, 39 which is evident in low- and middle-income countries where up to 10% of the family’s disposable income may be spent on tobacco products. 40 This underscores the need for economic empowerment among individuals in the fight against tobacco use.
Our study revealed an intriguing association between mobile phone ownership and tobacco use. Men who owned either a smart or non-smart phone exhibited lower odds of tobacco use than those who did not own a mobile phone. This finding could be attributed to several factors. First, mobile phone ownership may indicate a higher socioeconomic status, which is often linked to lower tobacco use rates.38,41,42 Second, owning a mobile phone provides access to information about the health risks of tobacco use and smoking cessation resources,43,44 potentially leading to more informed decisions. Third, mobile phone ownership may foster social connectivity and a sense of belonging, 45 reducing the likelihood of engaging in socially discouraged behaviors like tobacco use. Overall, these findings suggest a complex interplay between mobile phone ownership, socioeconomic status, health awareness, and social factors influencing tobacco use behavior among men in Tanzania.
Our study indicated a significant association between alcohol consumption and tobacco use among men. Specifically, men who drank alcohol had more than 6-fold greater odds of tobacco use than those who did not drink alcohol. Several factors could explain this finding. First, both alcohol and tobacco are often used together in social settings, 46 where the use of one substance may increase the likelihood of using the other. This could be due to shared social norms that promote the use of both substances. Additionally, individuals who consume alcohol may be more likely to engage in risky behaviors, 47 including tobacco use. Our findings align with several studies conducted in East Africa48,49 and further reinforce the existence of co-use of alcohol and tobacco among men.27,50-52 This study calls for stakeholders in alcohol and tobacco control in Tanzania to collaborate closely to formulate integrated strategies for interventions targeting tobacco use and alcohol consumption among men.
To our knowledge, this study represents the first nationally representative estimates of tobacco use prevalence and associated factors among Tanzanian men aged 15-49 years, utilizing data from the 2022 TDHS-MIS. However, our study is subject to several limitations. First, our analysis was based solely on the data available from the 2022 TDHS-MIS. It is possible that certain variables, such as community factors influencing tobacco use, were not captured during the survey, thus limiting the scope of our study. Second, the outcome variable of tobacco use was self-reported, which may introduce bias due to social desirability. The acceptability of tobacco use can vary significantly within Tanzanian communities, potentially affecting the accuracy of the reported prevalence rates. Finally, the cross-sectional design of our study prevents us from establishing causality.
Conclusion
The current study revealed that in 2022, 11% of men aged 15-49 years were using tobacco products, with 95% being smokers, 17.1% using smokeless tobacco products, and 12.1% using both smoked and smokeless products. Despite a progressive decrease in tobacco use among Tanzanian men, as noted in this study, there is still a pressing need for further efforts to reduce the rate of tobacco consumption. In this study, older age, alcohol consumption, belonging to the poorest households, and residing in the Eastern zone or Zanzibar were associated with greater odds of tobacco use. Meanwhile, attainment of secondary education or higher, lack of occupation, being the head of the household, owning a mobile telephone, and residing in the Southern Highlands zone were associated with lower odds of tobacco use. These findings emphasize the need for innovative, targeted interventions that consider age-specific risk factors and regional variations to further reduce tobacco consumption among Tanzanian men.
Footnotes
Acknowledgements
The authors would like to thank the DHS program for permitting them to use the dataset.
Author Contributions
CHM conceptualized the idea, analyzed the data, interpreted the findings, and prepared the initial draft. LPR conceptualized the idea, analyzed the data, interpreted the findings, and revised the manuscript. All the authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.