
Abstract
Introduction
We have already suggested that waterpipe (WP) smoking is associated with an increase in saliva cotinine and carbon monoxide in a small number of smokers.
Objective
The primary objective of this study was to confirm the increase in exhaled carbon monoxide (CO) and saliva cotinine equivalents levels in waterpipe smokers in a real smoking environment, compared with cigarettes smokers and never smokers. The secondary objective was to assess the factors associated with WP dependence according to the Lebanese Waterpipe Dependence Scale —11 (LWDS-11).
Methods
Three groups were included in the study: never smokers (n = 43), waterpipe smokers (n = 103), and cigarette smokers (n = 42). A questionnaire was completed for each participant, exhaled CO measured before and after waterpipe or cigarette smoking, and saliva cotinine equivalents dosed one hour after WP smoking or after one cigarette.
Results
Waterpipe smokers, like cigarette smokers, are exposed to nicotine and to CO. We found that levels of saliva cotinine equivalents were lower in waterpipe compared with cigarette smokers, but significantly higher than never smokers. In waterpipe smokers, saliva cotinine equivalents was mainly affected by the number of waterpipes per week and the size of the waterpipe. High levels were again found for expired CO, which increased by 500% in waterpipe smokers, in comparison with 100% in cigarette smokers; in waterpipe smokers, the relative increase in CO was affected by the number of waterpipes smoked before measurements, while it was inversely associated to the number of persons with whom they were sharing the WP and to the WP size. WP dependence was significantly correlated with the number of smokers at home, at work, and the body mass index.
Conclusion
This is a confirmation of real life waterpipe tobacco smoking characteristics in Lebanon. It indicates that nicotine is only marginally retained in the bowl water where smoke passes, and that waterpipe smokers could be exposed to harmful substances, such as CO that was found to be quite high. The level of expired CO and salivary cotinine could be good tools to detect exposure to waterpipe tobacco smoking. In addition, obesity and surrounding smokers could increase the risk of WP dependence.
Introduction
Waterpipe (WP) is a form of tobacco smoking, quickly spreading in Middle Eastern countries and the world.1,2 Details regarding waterpipe smoking can be found in selected studies,3,4 a detailed review published by Knishkowy and Amitai, 5 the report of the WHO 3 and its critique. 6 Two experimental studies were conducted in Beirut, showing that in vitro collected smoke of 100 puffs contained nicotine, tar, and heavy metals in high quantities, in some cases exceeding several-fold those found in a single cigarette.7,8 Harfouche and Geahchan showed that while some nicotine is filtered by the bowl water, the cancer-causing benzo(a)pyrenes were not. 8
According to Shafagoj and collaborators, plasma, saliva and urinary nicotine and cotinine concentrations increased significantly following a single run of waterpipe tobacco smoking. 9 The usefulness of serum cotinine level as a biomarker of any nicotine exposure is well known: a serum cotinine concentration of 10 ng/ml is suggested as a breakpoint threshold to differentiate between smokers and never smokers. Non-invasive alternatives to serum cotinine urine, saliva, or hair measurements (with suggested breakpoints of 200 ng/ml, 5 ng/ml and 0.3 ng/mg respectively.10–14
Another substance, carbon monoxide (CO), is known to be a toxic byproduct of smoking, causing potentially fatal acute and chronic effects. 15 It is also used as a biomarker for active smoking16,17 and passive tobacco exposure. 18 The concentration of CO in end-expired air is highly correlated with carboxyhemoglobin in cigarette smokers.19,21 In waterpipe smokers, CO is elevated to significant levels as well,2,21,22 with a linear relationship between smoking intensity and carboxyhemoglobin concentration. 23
These facts suggest that waterpipe smokers are potentially exposed to the same substances that are harmful in cigarettes. Although studies concerning waterpipe tobacco smoking health effects are of small scale, it has been suggested to lead to cancers, genetic damages, diseases of the lungs and other conditions in active and passive smokers.24–29 Thus, it is now considered by the World Health Organization a global public health threat. 3 However, the WHO report has been criticized, and errors were shown, dealing with the chemistry of smoke, health-related effects, smoking patterns, description and history of the device and its use, gender and underage use aspects, prevention and research needs in this field: 6 the author suggested that many results were drawn in artificially produced and unrealistic conditions in a laboratory, that lead to confusion and overestimation of waterpipe toxicity. 30 This is why studies in real life circumstances are needed to evaluate the persistence of artificially demonstrated issues in a natural environment.
In a previous pilot study, 31 we had found a significant increase in saliva cotinine and CO in 15 waterpipe smokers in real life circumstances, compared with 20 never smokers and 20 cigarette smokers: mean values of saliva cotinine in water-pipe and cigarette smokers were very close: 77.8 ng/ml (SD = 110.4) and 87.1 (SD = 82.7) respectively. The weight and height of smokers as well as the size of the waterpipe device affected saliva cotinine. However, in waterpipe smokers, CO increased by 300% after 1 hour of smoking, while in cigarette smokers, it only increased by 60%. In non-smokers, exhaled CO was similar to environmental CO (10.2 ppm). 31 We had concluded that waterpipe smokers would potentially be exposed to the same substances that are harmful in cigarettes.
On the other hand, we had validated a dependence scale for WP, the Lebanon Waterpipe Dependence Scale-11 (LWDS-11), composed of four subscales, the first representing nicotine dependence, the second negative reinforcement, the third psychological craving, and the fourth positive reinforcement. 32 The scale was validated in three different samples; the following post hoc analysis was carried out on one of these samples after score validation.
The primary objective of the current analysis was to confirm the increase of exhaled CO and saliva cotinine levels in waterpipe smokers in real smoking circumstances, compared with cigarettes smokers and never smokers. The secondary objective was to evaluate WP dependence determinants according to the LWDS-11 scale.
Material and Methods
Study Design
It was a comparative study that compared measures before and after one hour session of waterpipe or one single cigarette smoking in respective smokers, with a control group of never smokers.
Procedure
Between March and June 2006, a convenience sample of 188 adult individuals was addressed in their houses by four independent interviewers: 103 actual regular waterpipe smokers (arbitrarily defined as smoking 1 waterpipe/week or more), 42 cigarette smokers (defined as more than one cigarette/day) and 43 never smokers. Any mixed smoking of both waterpipe and cigarettes and any previous smoking were exclusion criteria from the study.
We explained the objective of the study to every participant, and they gave an oral consent before we began the procedure: all agreed to participate (100%). Every individual was face to face interviewed separately: a standardized questionnaire was orally administered in Arabic to all participants, which included questions regarding sociodemographic characteristics, detailed active smoking history and characteristics, in addition to the actual smoking description (type and duration of smoking session, size of the waterpipe device, number of persons sharing the waterpipe…), and waterpipe dependence. The latter was evaluated using the Lebanese Waterpipe Dependence Scale (LWDS-11) items, 32 which comprises the following four dimensions: physiological nicotine dependence (4 items), termination of dysphoric states or negative reinforcement (2 items), psychological craving (3 items), and positive reinforcement (encompassing pleasure and social interaction) (2 items).
Measurements
The waterpipe tobacco smoking session typically lasts 60–90 minutes; during this time, the smoker usually takes 50–200 puffs, ranging from about 0.15 to 1 liter each. 33 To keep up with a natural environment conditions, no wash-out period was required before measurements, and no efforts were made to standardize or to keep track of the number or magnitude of puffs; in addition, according to their will, smokers were free to smoke a waterpipe alone or to share it with several other persons. Individuals were asked to change nothing in their smoking circumstances. They were free to choose between the three sizes of waterpipe that are generally available: small (50 cm), median (70 cm) and large (100 cm); in all cases, 20 g of Mu'assel tobacco were used without refill (Mu'assel is the most commonly used type in Lebanon). 34 The charcoal used in all cases was of the commercially available quick-lighting type (1–2 pieces were used/hour). All measurements were carried out indoor.
We performed the measures before and after smoking, using a CO—Tester (NG type, F.I.M model). As required by the manufacturer, this tester was calibrated before each use according to every location environmental CO in parts per million. The first exhaled CO measurement was done prior to the beginning of the smoking for the three groups, and the second measurement was taken one hour after the beginning of smoking the waterpipe, or after smoking one cigarette. Without any delay, the individuals were told to exhale in the apparatus after retaining their inspiration for 10 seconds. For pre- and post- smoking CO measurement, the highest value in parts per millions was recorded after three trials.
Subjects were then asked to expectorate into a collection vial and saliva specimens were collected (>5 ml in volume). Nicotine metabolites measurements were thus performed in saliva one hour after the beginning of smoking for waterpipe smokers, at the end of the cigarette for cigarette smokers, and at random for never smokers. The source of cotinine in saliva was the current smoking episode, added to a baseline level from previous smoking episodes and from passive smoking.
A near-patient colorimetric method was used, using a disposable device called Saliva Smokescreen®: the occurrence of a yellow color indicated the presence of nicotine metabolites in their saliva; the darker the color, the higher the concentration of these metabolites. The principles of this method are described in details in the publication of Cope and collaborators; it is stated to have a high sensitivity and specificity, while being of excellent practicability since results are given on the spot. 35 This method confers a semi quantitative measurement for nicotine metabolites, termed cotinine equivalents concentration in micrograms/ml, because the assay detects all nicotine metabolites, including cotinine. The different colors on the chart give the following equivalents: color 1 corresponds to 0 mcg/ml, color 2 to 0–1 mcg/ml, color 3 to 1–1.5 mcg/ml, color 4 to 1.5–2 mcg/ml, color 5 to 2–2.5 mcg/ml, and color 6 to >2.5 mcg/ml. 35 The measurements’ reading was done separately by two research team members, and a consensus result was adopted after discussion in case of disagreement.
Statistical Analysis
Data entry was performed by independent laypersons that were unaware of the objectives of the study. Statistical analysis was performed using SPSS software, version 13.0. A p-value of 0.05 was considered significant. For continuous variables between groups’ comparison, we used ANOVA or Students’ tests for variables with adequate normal distribution. For non normally distributed continuous variables and for non continuous quantitative and ordinal variables, Kruskal-Wallis test was used. For categorical variables, the Chi2 and Fisher exact tests were used when applicable. Pre and post smoking values were compared between groups, in addition to the mean comparison of the relative increases in CO. Body mass index was used to classify patients between normal (BMI < 25), overweight (BMI 25–30) and obese (BMI > 30), despite the fact that it misclassifies as overweight people with large muscle mass.
Multiple linear regressions were carried out to compare measures between the three groups of comparison; measurements were associated to quantitative tobacco exposure variables, taking into account potential confounding variables: gender, city residence, age, height, weight, body mass index, education, work status, marital status and the number of smokers to which a person was potentially exposed (passive smoking at home and work). In addition, multiple regressions were performed for waterpipe smokers subgroup analysis; variables introduced in the model were the followings: performed measurement as a dependent variable, and number of waterpipes smoked before present measurement, time interval from last waterpipe, exact time lapse in minutes from start of present waterpipe, waterpipe size, number of persons with whom he is sharing the waterpipe, waterpipes per week, and the number of persons he is passively exposed to at home and at work as independent variables; in addition, gender, weight, height, body mass index, education, work status, marital status and city residence were taken into account.
A logistic regression was performed to evaluate the factors associated with WP dependence: the dependent variable was WP dependence defined as a score of more than 10 on the LWDS-11, 32 while independent variables were the following: number of smokers at home, number of smokers at work, body mass index, education level, age, marital status, gender, working status, and region type. A stepwise descendent likelihood ratio logistic regression was applied, and the final model was retained.
Results
Socio-Demographic Characteristics
In table 1, we report sociodemographic properties in smokers and never smokers. Never smokers and cigarette smokers groups contained more females than waterpipe smokers (p < 10-4). Cigarette smokers were mainly workers more than 35 years old (p < 10-4) with low education (p < 10-4), while waterpipe smokers were mainly young adult aged 22 to 35 years with high levels of education who were workers or students (p < 10-4). Waterpipe smokers were also more overweight than cigarette or never smokers (p < 10-4). Both waterpipe and cigarettes smokers lived with higher numbers of smokers at home (p = 0.01) or at work (p = 0.04). No significant differences were found for the dwelling region types (p > 0.05).
Sociodemographic characteristics of smokers and never smokers.

Smoking Characteristics
Waterpipe smokers had a mean duration of smoking of 3.55 years (SD = 3.57). (3.9%) had < 1 WP/week, 25(24.3%) 1–2 WP/week, 46(44.7%) 3–6 waterpipes/week, and 28(27.2%) >6 WP/week. 15.5% of WP smokers used the small size WP (50 cm), 79.6% used the middle size (70 cm), and 2.7% used the large WP (100 cm).
Cigarette smokers had a mean smoking duration of 10.42 years (SD = 5.71); 9(22.0%) smoked 2–10 cigarettes/day, 22(53.6%) 11–20 cigarettes/day and 10(24.4%) more than 20 cigarettes/day.
Carbon Monoxide and Saliva Cotinine Equivalents' Measurements
In Table 2, we present results for carbon monoxide and saliva cotinine equivalents in different categories of smokers; significant differences were found for pre-smoking CO, between never smokers and both types of smokers; non significantly higher values were found for waterpipe versus cigarettes smokers. For post-smoking CO and the mean relative increase in CO, values were more elevated in waterpipe smokers versus cigarette smokers: cigarette smoking had a 104% increase of their CO, while waterpipe smokers had a 476% increase. However, cigarette smokers showed moderate to high ranges of saliva cotinine equivalents, while the majority of waterpipe smokers had moderate ranges, and almost all never smokers showed the lowest range of saliva cotinine equivalents (p < 10−4).
Carbon monoxide (CO) and saliva cotinine equivalents measurements.
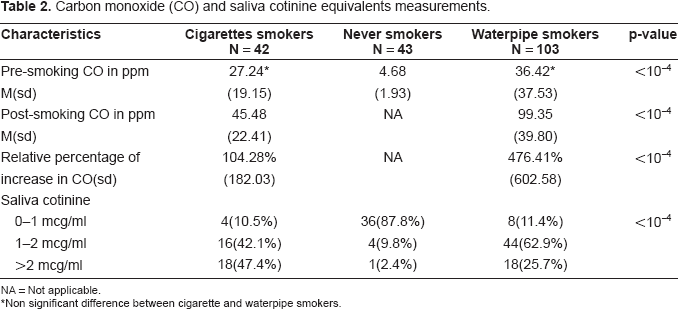
NA = Not applicable.
Non significant difference between cigarette and waterpipe smokers.
Factors Associated with Saliva Cotinine Equivalents and Carbon Monoxide
In multivariate analysis, saliva cotinine equivalents were mainly positively affected by the number of smokers at home, the number of cigarettes per day, the number of waterpipes per week and body mass index. We note that the magnitude of the weekly waterpipe consumption frequency effect on saliva cotinine equivalents was higher than that of daily cigarette consumption frequency, giving a ratio of 8.5 fold. In the waterpipe smokers’ subgroup, saliva cotinine equivalents were positively affected by the number of waterpipes per week and the size of the waterpipe (Table 3).
Multiple regression for determinants of CO and cotinine equivalents’ measurements.
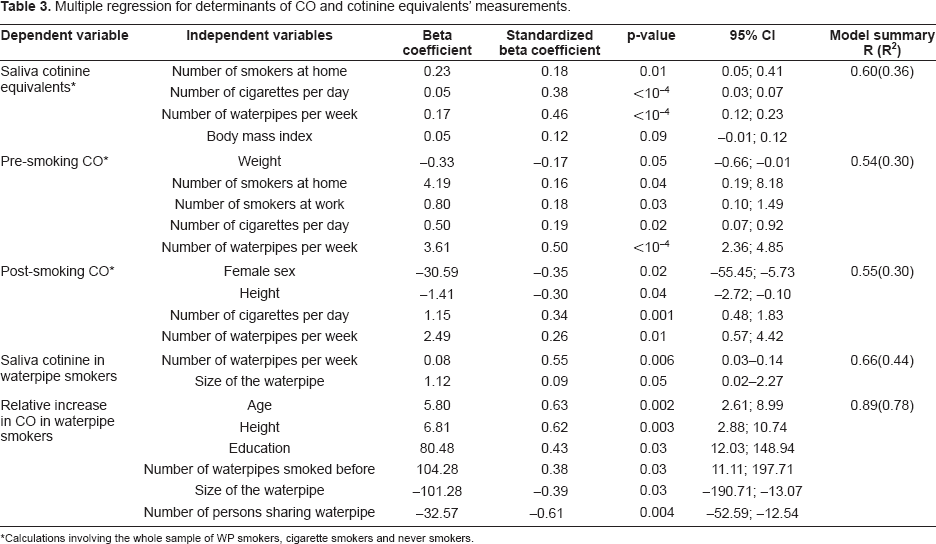
Calculations involving the whole sample of WP smokers, cigarette smokers and never smokers.
Pre-smoking CO was negatively affected by individual weight, but positively by the number of smokers at home and at work, the number of daily cigarettes and of weekly waterpipe. The magnitude of the waterpipe weekly consumption frequency effect on pre-smoking CO was similar that of daily cigarette consumption frequency, giving a 7 fold ratio.
Post-smoking CO was inversely affected by female sex and height, and positively affected by the number of daily cigarettes and weekly waterpipes. In waterpipe smokers’ subgroup, age, height, education, and the number of waterpipes smoked on the same day before measurement raised the relative increase in CO, while the size of the waterpipe and the number of persons sharing it decreased it (Table 3).
For waterpipe smokers, saliva cotinine equivalents were affected by smoking frequency and the size of the waterpipe, while the relative increase in CO was mainly positively affected by smoking frequency, and negatively affected by the actual size of the waterpipe and the number of persons sharing it (Table 3).
Factors Associated with WP Dependence
Out of 103 WP smokers, 24(23.3%) were considered WP dependent. WP dependence was correlated with the following factors: number of smokers at home (an increase by one smoker was associated with a almost a doubling of the risk of dependence), number of smokers at work (an increase by one smoker was associated with a 13% increase in the risk of dependence), and body mass index (one increment of body mass index was associated with a 10% increase in the risk of WP dependence) (Table 4).
Logistic regression for water pipe dependence.

Variables included but not retained in the final model: education, age, marital status, gender, working status, and region type.
Discussion
In this study sample, we found that the waterpipe smokers’ subgroup was mainly composed of unmarried males 22–35 years old, more educated (67% of post college education) and more obese than cigarette smokers, with a higher percentage of students (30.1% vs. 9.5%). This is concordant with a study we performed on a representative sample of Lebanese adults, where we found that the waterpipe smokers subgroup contained a higher percentage of highly educated people and university students 34 and with previous studies done in Lebanon:24,36 in 2001, a 40% smoking prevalence was found in university students, including 21% waterpipe tobacco smoking, 24 whereas in 2003 Chaaya found a 43% smoking prevalence in university students, with 28.3% of current waterpipe tobacco smoking. 36 In addition, a person living with smokers at home or at work has a higher probability of being a smoker, whether for cigarettes and waterpipe tobacco smoking. This is also in line with what was found by Waked and collaborators, where individual smoking habit was also affected by home and work smokers. 34
We also demonstrated in our study that water-pipe smokers, like cigarette smokers, are exposed to nicotine and to CO. We found that levels of saliva cotinine equivalents were lower in waterpipe compared with cigarette smokers, but significantly higher than never smokers. In waterpipe smokers, saliva cotinine equivalents were mainly affected by the number of waterpipes per week and the size of the waterpipe. These results are highly similar to those obtained by El-Nachef and Hammond for CO, 22 and those we obtained in the pilot study, 31 where the quantitative method showed a mean saliva cotinine of 87.1 ng/ml in cigarette smokers, 77.8 ng/ml in waterpipe smokers, and 29.9 ng/ml for never smokers. 31 Other researchers have also found an increase in saliva cotinine levels in healthy volunteers, but the cotinine levels in their study increased from 0.79 +/- 0.79 ng/ml to 283.49 +/- 75.04 ng/ml after smoking 20 g of Mua'sel for a period of 45 minutes. 9 The fact that their study was experimental on healthy volunteers while ours was in real life smokers may explain the differences in obtained results; in addition, differences in measuring techniques and possible genetic polymorphism distribution in nicotine metabolic pathways 37 between our population and theirs could also explain the results. For never smokers, we found a significant percentage with saliva cotinine >1 mcg/ml (12.2%): this could be an artifact of the semi-quantitative method we used or indicate unreliability of the subjects; it could also be the result of heavy passive smoking, particularly given that the number of environmental smokers highly affected saliva cotinine of never smokers (see Table 3).
In the pilot study, we had found that saliva cotinine in waterpipe smokers was inversely affected by the time interval from the last waterpipe (B = −0.46), the number of persons with whom they were sharing the waterpipe (B = −58.5), while it was positively associated to the waterpipe size in cm (B = 175.36) and the exact time elapsed from the start of the present waterpipe (B = 8.24). 31 In the present study, similar results were found, and saliva cotinine was directly associated with the number of waterpipes smoked per week (B = 0.08) and the size of the waterpipe (B = 1.12). Our findings contradict again the commonly held belief that the water of the waterpipe water pipe renders the smoke harmless, and confirm what was proven experimentally:7,8,33 nicotine content of waterpipe smoke issued from an experimental smoking machine with a common “mua'sel” tobacco was significantly high. Moreover, analysis of the bowl water content showed that there were little amounts of nicotine retained in it, although nicotine is highly soluble in water;7,8,33 thus, water has no repercussion on the amount of nicotine absorbed by the smoker, who in turn is expected to control his nicotine needs by titrating his consumption.
We also found that the effect of the weekly waterpipe consumption on saliva cotinine was higher than the daily cigarette consumption frequency, giving a 8.5 fold ratio; in other words, 1 waterpipe may be equivalent to 8.5 cigarettes in increasing saliva cotinine. Nevertheless, we note that cigarette smokers’ cotinine represents a steady state mean concentration, 38 while that of waterpipe seems to be a steady state peak concentration, given the differences in frequencies of cigarette and waterpipe tobacco smoking, and the known toxicokinetic parameters of cotinine. 38 Further research is needed to depict more clearly the patterns of cotinine formation in Lebanese waterpipe smokers compared with cigarette smokers.
High concentrations were found for expired CO: pre-smoking CO was much higher in both cigarette and waterpipe smokers than in never smokers; however, the magnitude of effect differs: one waterpipe is equivalent to 7 cigarettes in elevating steady state CO. On the other hand, CO increased by 500% in waterpipe smokers after one hour of smoking, in comparison with 100% in cigarette smokers after one cigarette; in the pilot study, close results were found, with 300% versus 60%, respectively. Sampling fluctuations may explain the observed differences; another explanation may be the use of commercial quick lighting coal instead of natural charcoal. 2 Nevertheless, this is much more than found by Sajid KM and et al. who concluded that the CO hazard is as high with waterpipe tobacco smoking as with cigarette smoking. 21
In waterpipe smokers, the relative increase in CO was affected by the number of waterpipes smoked before measurements, while it was inversely associated to the number of persons with whom they were sharing the waterpipe and to the waterpipe size. This was found in our pilot study, 31 and was also reported in other studies, where CO amounts in waterpipe depended on the type of coal used and the size of the waterpipe, the highest amounts obtained with small size waterpipe. In fact, the increase in the size of the waterpipe (i.e. volume of air in water base, bowl volume, pipe length, etc.) reduced the CO amounts significantly (P < 0.001).21,39 Furthermore, CO concentration in the expired air may be affected by other subject-dependent factors, such as emphysema, 19 variable ventilation during sleep or exercise, and environmental confounders (traffic, heating and cooking emissions). 40
The generated multivariate models explained variations of both saliva cotinine and CO in a satisfactory way (high R2). Thus, as for cigarette smokers,41,42 saliva cotinine and CO may be useful indicators of exposure to waterpipe in exclusive smokers in clinical application during smoking cessation programs; taking into account individual covariates and passive smoking would give precise equations, in particular for waterpipe smokers. Our results may also suggest that waterpipe tobacco smoking may predispose its consumers to serious health risks, as serious as those caused by cigarette smoking. This is especially true for CO hazard, that appears to be really high in waterpipe smokers, where values up to 125 ppm were found; this level increases the risk of acute neurological and cardiovascular effects such as headache, flushing of the skin, in addition to chronic health effects; 15 equilibrium carboxyheamoglobin concentrations of up to 15% could be found in these circumstances, which may affect exercise, sensorymotor and neurobehavioral performance and vigilance. 43
On the other hand, we found WP dependence in around one quarter of WP smokers. Dependence was mainly affected by a higher number of surrounding smokers at home and at work, in addition to obesity. Obesity could be an indicator of sedentarity in these individuals. These results confirm what was found in a representative sample of Lebanese smokers, 34 and are in line with the finding that social interaction is a component of waterpipe dependence. Chaouachi for example has thoroughly delineated that waterpipe tobacco smoking has a specificity that differentiates it from cigarette smoking, which is the conviviality of sharing it between several smokers and the long duration of a smoking session, generating situations of inter-individual communication and social cohesion. 44
Finally, given the large number of people who smoke waterpipe, it is essential to study the health effects of water pipe smoking with renewed emphasis. 45 The additional key question of public health concern is exposure to toxic combustion products other than CO, such as the many carcinogens that are generated by tobacco smoke. It is the latter type of measurements that are really needed to make statements about the harm of waterpipe tobacco smoking in otherwise healthy adolescents or young adults, taking into account that the majority of waterpipe tobacco smokers smoked less than one waterpipe per day. Thorough studies to evaluate these effects are necessary; in case of causality proving, eventual information and believes’ changing would be necessary to control the possible disguised hazard that is becoming particularly common in Lebanon and neighboring countries.
We are aware that the study design could have generated systematic errors: a selection bias is possible due to the convenience sample of our study; particularly since it comprised people addressed at their home, who could differ in their socio-demographic profile from waterpipe smokers in cafέs. 31 However, our results were largely similar to those of the pilot study we had previously performed in a cafέ, which could decrease the risk of this selection bias. A recall bias is also possible for smoking history and passive smoking reporting, and measurement errors could occur for CO and for saliva cotinine equivalents: the semi-quantitative cotinine equivalents measurement may be less precise than quantitative measurements. However, these errors are expected to be non-differential, and could only bias the obtained results towards the null. In addition, we could have left over some confounding variables, which may have generated some residual confounding.
However, we have no reason to believe that the essential of the obtained results would change, given particularly that the obtained results confirm previous ones.31,33,34 Nevertheless, we suggest further large-scale studies for unanswered issues, particularly serum measurements of toxic products other than CO and cotinine, in addition to health effects of waterpipe tobacco smoking.
Conclusion
This is a confirmation of real life waterpipe tobacco smoking characteristics in Lebanon. It indicates that nicotine is far from fully retained by water in the bowl where smoke passes, and that waterpipe smokers could be exposed to harmful substances, such as CO that was found to be quite high. In addition, obesity and surrounding smokers could increase the risk of WP dependence. The level of expired CO and salivary cotinine equivalents could be good tools to detect exposure to waterpipe tobacco smoking.
Disclosure
The authors report no conflicts of interest.