
Abstract
Context
Accurate prognostication is important in oncology and palliative care. A multidisciplinary approach to prognostication provides a novel approach, but its accuracy and application is poorly researched. In this study, we describe and analyze our experience of multidisciplinary prognostication in palliative care patients with cancer.
Objectives
To assess our accuracy of prognostication using multidisciplinary team prediction of survival (MTPS) alone and within the Palliative Prognostic (PaP) Score.
Methods
This retrospective study included all new patients referred to a palliative care consultation service in a tertiary cancer center between January 2010 and December 2011. Initial assessment data for 421 inpatients and 223 outpatients were analyzed according to inpatient and outpatient groups to evaluate the accuracy of prognostication using MTPS alone and within the PaP score (MTPS-PaP) and their correlation with overall survival.
Results
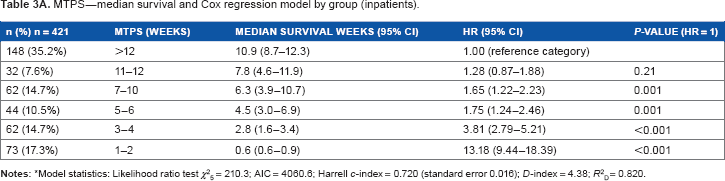
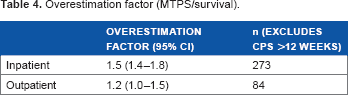
Inpatients with MTPS-PaP group A, B, and C had a median survival of 10.9, 3.4, and 0.7 weeks, respectively, and a 30-day survival probability of 81%, 40%, and 10%, respectively. Outpatients with MTPS-PaP group A and B had a median survival of 17.3 and 5.1 weeks, respectively, and a 30-day survival probability of 94% and 50%, respectively. MTPS overestimated survival by a factor of 1.5 for inpatients and 1.2 for outpatients. The MTPS-PaP score correlated better than MTPS alone with overall survival.
Conclusion
This study suggests that a multidisciplinary team approach to prognostication within routine clinical practice is possible and may substitute for single clinician prediction of survival within the PaP score without detracting from its accuracy. Multidisciplinary team prognostication can assist treating teams to recognize and articulate prognosis, facilitate treatment decisions, and plan end-of-life care appropriately. PaP was less useful in the outpatient setting, given the longer survival interval of the outpatient palliative care patient group.
Keywords
Introduction
Accurate prognostication is a core aspect of oncology and palliative care.1,2 At a time of increasing availability of new and expensive cancer treatments with variable survival benefits, accurate prognostication is important in selecting beneficial treatments and avoiding treatments that may not be in the best interest of the patient.3–5 Timely diagnosis of the end stage of life, coupled with effective communication, is an integral part of palliative management and empowers the patient and their caregivers to become active, effective participants in clinical decision-making and patient care. 6
However, accurate prognostication has proved to be challenging and the tendency for clinicians to be inaccurate and overestimate survival is well documented.7–9 Barriers to prognostication include suboptimal training of clinicians in this clinical skill, with much greater focus on diagnostic and therapeutic skills,1,10 reluctance among clinicians to prognosticate, 10 and a lack of accurate prognostic tools to guide clinicians who are caring for patients with advanced illness.10,11 In recent years, several prognostic tools have been developed to improve prognostication in palliative care patients.12–16 The PaP score is one of two validated prognostic tools for use in patients with advanced cancer that was identified by the steering committee of the Research Network of the European Association for Palliative Care. 2
The PaP score relies heavily upon a clinical prediction of survival (CPS), which is commonly determined by a single clinician. The CPS has the highest partial weight among the components of the PaP score. It is measured in 1- to 2-week intervals up to 12 weeks, after which all estimates are grouped as >12 weeks. Although the CPS tends to correlate with survival, 17 it is twice as likely to be overoptimistic than over-pessimistic and to overestimate the length of actual survival by a factor of between 3 and 5.2,17 It appears that the use of CPS with validated tools affords the greatest accuracy in predicting survival. 18 In addition, early data suggest that a multidisciplinary team prediction of survival (MTPS) is better than the prediction of a doctor or nurse clinician alone. 19
In settings such as the outpatient palliative care clinic in a cancer center, where patients tend to have longer survival, 20 the application of PaP has not been well studied. One prospective study which looked at the survival of 250 Brazilian female outpatients with advanced malignancies found that the PaP score subdivided the study population into three groups according to their survival, consistent with the three groups identified in the validation and subsequent studies of PaP. 21 Given that palliative care is increasingly integrated into the outpatient setting in cancer centers, it is important to have prognostic tools that are useful for this population of patients. 22
In our center, we calculate the PaP score using the MTPS which is agreed by the palliative care team at a weekly multidisciplinary team meeting. This score is entered into the PaP score with the other five factors and is weighted in the same way as the CPS would have been weighted. The purpose of this study was to describe and analyze this multidisciplinary approach to prognostication in palliative care patients with cancer.
Methods
Study setting and participants
This retrospective study was conducted at the Peter MacCallum Cancer Centre by the Department of Pain and Palliative Care (DPPC) consultative service. Patients are referred to the DPPC by oncologists within multidisciplinary tumor streams for assessment and management of symptoms associated with cancer and its treatment, care coordination and planning, and end-of-life care. Referred patients may be first seen in an inpatient setting of the cancer center, when under the primary care of their oncologist, or while attending outpatient clinics for oncological management and review. The DPPC conduct twice-daily palliative care outpatient clinics, termed Rapid Response Clinics, which enable the same-day review of urgent referrals concurrent with their oncology review, as well as booked reviews.
On first review, all patients undergo comprehensive assessment, by either a palliative care doctor or nurse practitioner, which includes completion of a suite of validated assessment tools, including the Edmonton Classification Scale for Cancer Pain, Palliative Prognostic (PaP) Score, and a pain chart. Other data include demographics such as the date of birth, date of cancer diagnosis, referring tumor stream, performance status measures (Karnofsky Performance Status [KPS]), genogram with a focus on assessment of children and bereavement risk, and pathology parameters (total white blood cell [WBC] and lymphocyte count). The prediction of survival is reached by consensus within the weekly multidisciplinary team (MDT) meeting, with most input from medical and nursing team members. The palliative care MDT at that meeting consists of palliative care specialist doctors, palliative care nurses, a social worker, a pharmacist, and a pastoral care worker. These data are recorded in the DPPC database.
Study inclusion was limited to patients with a solid malignancy who had a first contact by the palliative care team between 1 January 2010 and 31 December 2011 and had deceased before 1 June 2012, when the data were extracted. Patients with an incomplete data set or with primary renal or hematological malignancy were excluded as in the original PaP score study due to possible effects on blood values. 15 Overall survival was defined as time from first encounter by DPPC to death from any cause. If a patient had multiple contacts with the palliative care team, only data from the first contact were included for analysis.
Inpatients were defined as patients who had their first contact with the palliative care team during an inpatient hospital admission. Outpatients were nonadmitted patients who had their first contact with the palliative care team when attending an outpatient clinic or attending for same-day treatments such as radiotherapy, chemotherapy, or apheresis.
Ethics approval was obtained from the Human Research and Ethics Committee at the Peter MacCallum Cancer Center, Melbourne (June 2012 No 12/83).
PaP score
The PaP score consists of six prognostic elements, CPS, KPS, anorexia, dyspnea, total WBC count, and lymphocyte percentage. Each element is assigned a weighted partial score, the sum of which ranges from 0 to 17.5, which then classifies patients with advanced solid malignancy into three risk categories predictive of 30-day survival. These are group A (score ≤5.5), probability >70%; group B (score 5.6–11.0), 30–day survival probability 30%–70%; group C (score ≥11.1), 30–day survival probability <30%.15,23
Statistical analysis
The prognoses estimated by the MTPS and calculated by MTPS-PaP score were each correlated with actual survival. The data for inpatients and outpatients were analyzed separately in view of the different nature of these two populations.
Differences in patient demographics, disease characteristics, MTPS-PaP score, and MTPS by patient cohort were analyzed by chi-squared tests for categorical variables,
To calculate the overestimation factor, each patient was assigned an MTPS using the midvalue from the MTPS interval. Patients who had an MTPS >12 weeks were excluded from this analysis since the midvalue for this category was undefined. The ratio of the MTPS and actual survival was calculated for each patient and then log transformed as the ratio had strong positively skewed distribution. Geometric means and CIs were used when reporting the overestimation factor.
All
Results
The analysis included 644 patients, which was 89.8% of total eligible patients (Fig. 1). Separate analyses were conducted for inpatients ( Screening summary.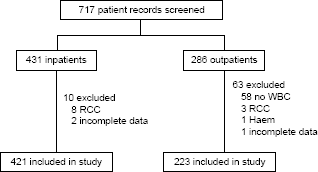
Patient characteristics.

Chi-squared test for overall group difference,
Chi-squared test for overall group difference,
Accuracy of PaP groups
The MTPS-PaP score subdivided the inpatient cohort into three homogenous risk groups according to survival time (Fig. 2A, log-rank test for trend (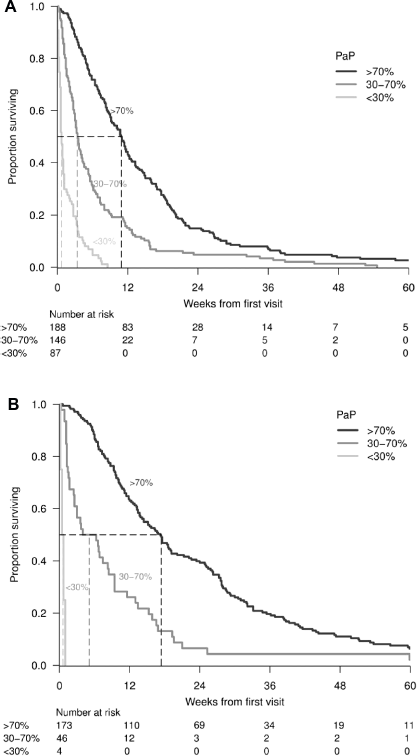


The accuracy of MTPS

Overestimation factor (MTPS/survival).

(
Comparison of survival prediction by MTPS and the MTPS-PaP score
Spearman correlation inpatients and outpatients.

Discussion
In this study, the MTPS-PaP score accurately classified inpatients into three risk groups based on survival. This is consistent with previous studies that have evaluated the PaP score in the inpatient setting.23–27 Our data also confirmed the well-recognized
We further demonstrated that the PaP score is clinically less useful in the palliative care outpatient setting where survival times are generally longer. Our patient distribution was significantly skewed: 75% of the outpatients fell within PaP group A and less than 2% within group C. With evolving models of care that promote the early integration of palliative care, services will be increasingly involved in the care of outpatients in oncology and other illnesses.30–32 For this group of patients where survival is generally longer, other prognostic factors such as cancer type, comorbidities, and performance status may play a more important role.33,34 Prognostic tools designed specifically for palliative care outpatients may be of greater utility than the PaP score in this setting.20,35
While still overestimating actual survival, we found MTPS to be more accurate compared to CPS performed by single clinicians and less accurate than MTPS-PaP. This is consistent with the literature, which recommends the use of CPS in combination with other prognostic factors or scores to improve accuracy of predictions. 2
While improving accuracy of prognostication is important, the focus of our MTPS discussion is not so much about achieving finely tuned prognostic accuracy than about assisting the team to focus on assessing the preparedness of the patient, family, and medical team in coordinating and planning end-of-life care and to ensure that the goals of care are aligned with the estimated prognosis and anticipated outcomes. A multidisciplinary approach to prognostication is in keeping with the overall multidisciplinary approach, which is regarded as the standard of care in oncology and palliative care. We recommend its application as a core activity for palliative care services.
Limitations of this study are its retrospective design with its incumbent risk of bias and missing data. In addition, the data are obtained from a single institution only. The MDT structure varied from week to week; however, it always included palliative care doctors and nurses, who played the major role in determining the prognostic estimate.
Further areas for study include understanding how the MDT arrive at consensus when prognosticating and how each team member contributes to this discussion. A comparison of the accuracy of MTPS versus single-clinician estimate of CPS within the PaP score would be of interest. There is a need to develop prognostic tools that are better suited for the palliative care outpatient setting. Finally, the impact of improving our ability to prognosticate upon our clinical decision-making and patient outcomes has yet to be well studied.
Author Contributions
Conceived and designed the experiments: RM, WS, NM, OS. Analyzed the data: DZ. Wrote the first draft of the manuscript: RM, WS. Contributed to the writing of the manuscript: RM, WS, NM, OS. Agree with manuscript results and conclusions: RM, WS, DZ, NM, OS. Jointly developed the structure and arguments for the paper: RM, WS, NM, OS. Made critical revisions and approved final version: RM, OS. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
We acknowledge the participants and the clinical and research staff at Peter MacCallum Cancer Center. In particular, we thank Catherine Devlin and Martina Johnstone for database assistance.