
Abstract
Background:
The growing number of patients diagnosed with advanced cancer increases the pressure on health systems, especially in lower-middle-income countries. Telemedicine palliative care consultation is innovative in providing quality cancer care while reducing costs. However, there is a lack of randomized controlled studies that evaluate the effects of digital consultations in the palliative treatment of cancer patients. This study aims to investigate the efficacy of telemedicine consultation in outpatient palliative care settings.
Methods/Design:
During an 18-month recruitment period, participants recently diagnosed with advanced cancer who are not already receiving palliative care are invited to participate in a randomized controlled trial. Eligible participants are randomized to the intervention group (telemedicine) or the control group (face-to-face) consultations. Patients have monthly scheduled consultations (three such consultations), and unscheduled consultations as needed, provided through telemedicine or face-to-face visits. The primary outcomes are patients’ quality of life assessed monthly using the EORTC-QLQ-C30 Questionnaire, changes in self-reported symptom control measured at every visit through the mean changes in distress score on the IPOS Questionnaire, and patients’ satisfaction assessed monthly using the FAMCARE P16 Questionnaire. Secondary outcomes are eHealth Literacy, the domain of intervention, number of patients satisfied with physician communication, patients’ experiences with the care, number of emergency room visits, number of unscheduled visits, adherence to intervention, changes in medication adherence, number of completed telemedicine scheduled visits, and physician’s ability to evaluate a patient through telemedicine.
Discussion:
This is one of the first randomized controlled trials investigating virtual palliative care. Our data will determine whether telemedicine is appropriate for outpatient palliative care.
Trial registration:
ClinicalTrials.gov Identifier: NCT06538350.
Plain language summary
What is this about? In recent decades, more and more people have been diagnosed with advanced cancer, and this puts much pressure on the healthcare systems, especially in countries with fewer resources. One possible solution is using video calls for palliative care (care that focuses on improving the quality of life for patients with life-limiting illnesses). While this might save money and help more patients get care, we do not have enough solid research to know if it works well. What we are doing We are running a study to see if video calls are as good as in-person visits for palliative care. Here is how it works: We are looking for people who were recently diagnosed with advanced cancer and haven’t started palliative care yet. After randomly allocating these participants into two groups, one will have their appointments via video calls, and the other will have traditional face-to-face visits. Each participant will have three scheduled monthly check-ups and extra appointments as needed. What we are measuring We want to know: How the care affects patients’ quality of life (checked every visit) How well symptoms are managed (checked every visit) How satisfied patients are with their care (checked every visit) We’re also looking at other things, like: How comfortable patients are using technology How often do they need emergency care Whether they attend all their scheduled appointments How well they take their medications How well doctors can evaluate patients through video Why this matters? This study is one of the first to test whether video appointments work for palliative care. What we learn will determine whether this is a good way to help more patients get the care they need.
Introduction
In recent decades, cancer has become a significant public health concern and the second leading cause of death after cardiovascular diseases in the European region, particularly in lower-middle-income countries.1–3 In Europe, disparities in prevention programs, access to advanced diagnostics, treatments, and care across the cancer care continuum lead to significant differences in the timing of cancer diagnosis and survival rates.4,5
In addition to the Action Plan for the prevention and treatment of diseases, the European Commission is also working to improve access to and quality of care, 6 promoting the integration of palliative care into primary, secondary, and tertiary care, and disseminating best practices in innovative palliative care strategies. 7
The World Health Organization defines telemedicine as “the delivery of health care services, where distance is a critical factor, by all health care professionals using information and communications technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities” (WHO, 8 p. 10).
As demonstrated during the COVID-19 pandemic, implementing telemedicine options offers a new opportunity to address public health emergencies9–11 and combat disparities faced by cancer patients. 7
However, there is still significant potential to leverage telemedicine to improve access to healthcare and achieve better health outcomes for people with cancer.9,10,12
Telemedicine interventions include a variety of delivery methods: online, telephone, video, and interactive applications. They are not designed to replace face-to-face care completely but are intended to complement traditional care through a hybrid delivery model. 13
Telemedicine has demonstrated a substantial impact on improving access to palliative care for patients in rural and underserved areas with limited medical infrastructure, who face challenges such as a lack of healthcare providers and limited medical facilities, which bridge the gap between patients and specialized care providers.14,15 By enabling remote consultations and follow-ups, telemedicine alleviates geographical barriers and ensures that patients receive the palliative care they need, regardless of location.
Telemedicine interventions have been shown to improve patient comfort through improved symptom management significantly. By facilitating timely remote consultations and ongoing monitoring, telemedicine allows for frequent adjustments to care plans based on real-time data, leading to improved symptom management, overall patient comfort, and improved quality of life.16–20
By improving communication between patients and healthcare professionals, telemedicine has not only facilitated better access to care but also alleviated caregiver stress. This stress reduction has been associated with a more favorable experience and increased satisfaction among both patients and caregivers, leading to better adherence to treatment plans and improved overall outcomes.21–24
The cost-effectiveness of telemedicine in delivering palliative care, particularly in regions with financial and logistical constraints, is a significant advantage. Conventional models often involve substantial travel costs and are resource-intensive due to the need for regular in-person visits. Telemedicine alleviates this burden, allowing providers to manage a larger number of patients with increased efficiency. 25
Telemedicine, which incorporates modalities such as real-time video consultations and remote patient monitoring, is crucial for improving patient-centered care. However, widespread adoption of telemedicine is hampered by significant factors, including cultural differences, disparities in digital literacy, and language barriers.25–27 It is essential to recognize that “there is no one-size-fits-all.”28–30 Despite the recognition of the benefits of telemedicine by many patients, they consistently face challenges, particularly technical issues, that need to be addressed.17,22,31,32 The willingness of patients and caregivers to utilize telehealth services can have a significant impact on the efficacy of these programs. Hesitation to adopt telehealth, whether due to technological issues or a preference for face-to-face encounters, can hinder the success of telehealth.27,33,34
While telemedicine has shown promise in various areas of healthcare, providing state-of-the-art healthcare and treatments in remote, understaffed locations through contemporaneous communication and information technologies, 35 recent reviews have highlighted a significant gap in our understanding of its efficacy in palliative care.17,18,36
Challenges in measuring the clinical benefits of palliative care interventions delivered through digital technologies, such as patient and caregiver comfort, emotional and spiritual state, and quality of life, underscore the need for further research. There is also a need to explore how telemedicine initiatives in palliative care can be integrated into existing care systems.18,36
Aims
This study aims to estimate the effects of a palliative care consultation intervention among adults with advanced cancer delivered either as a remote (telemedicine) or face-to-face consultation.
The study will focus on the following areas:
Exploring patient views on quality of life, changes in symptom control, and patient satisfaction
Exploring patient experience on care received, adherence to interventions, communication with the physician, need for additional care, and changes in digital literacy
Subsequently, the proportion and reason for ineligibility, retention rate, and completion rate will be assessed.
Study hypothesis
Telemedicine consultations are non-inferior to face-to-face consultations for palliative care in outpatients diagnosed with cancer. Non-inferiority is evaluated using a 10-point non-inferiority margin on the EORTC-QLQ-C30 Global Health Status/Quality of Life (GHS/QoL) scale, consistent with published minimally important clinical difference estimates for this instrument.37–44 Non-inferiority will be concluded if the lower bound of the 95% confidence interval for the between-group difference exceeds the predefined – 10-point margin.
Methods/design
This is a prospective, single-center, randomized, parallel assignment, controlled study, with a 1:1 allocation across two treatment arms: telemedicine consultations versus face-to-face consultations.
The trial was registered on ClinicalTrials.gov (NCT06538350) before initiating study procedures. Registered on 6 August 2024.
Recommendations for interventional trials (SPIRIT) guidelines were followed when constructing the protocol for this study (Supplemental Material).45,46
An overview of this study is shown in Figure 1.

Trial schematic.
Study setting/location
All trial activities will be conducted through the Outpatient Clinic of OncoHelp Association located in Timişoara, Romania. The OncoHelp Oncology Center is a private university hospital that offers unlimited access and free oncology, hematology, radiotherapy, and palliative care services to patients diagnosed with cancer, malignant hemopathies, and other hematological diseases based on a contract with the National Health Insurance System.
This trial will take place over 18 months.
Study population
The participants will be recruited from patients newly diagnosed (in the last 3 months before enrollment) with advanced locoregional and metastatic cancer (solid tumors) who did not receive oncological treatment and palliative care interventions before enrollment in this study and are referred to the OncoHelp Association Outpatient Clinic for oncological and palliative care consultation and treatment.
Patients with advanced cancer may have difficulty using digital health solutions and may require, at least initially, the assistance of a relative to access telemedicine visits. 47
Caregivers may assist participants during visits if needed, but their presence is not mandatory. Relatives will not sign an informed consent form, and the study team will not collect any information from relatives.
Caregiver assistance will be limited to reading questions aloud or providing clarifications without influencing responses.
Relatives or friends willing to participate in the study who the Participant has identified should live with the Participant or have contact with the Participant at least twice a week.
Caregivers should have a performance status that allows for the Participant’s care and assistance during visits (Eastern Cooperative Oncology Group (ECOG) ⩽2), and also not be themselves diagnosed with cancer or receiving cancer treatment during the study (to ensure that the Participant and caregiver focus their efforts on the Participant’s care).
The caregiver must have access to a computer/tablet/smartphone and an internet connection at home, and be willing to participate in a telemedicine study. It is necessary to have basic digital skills that allow them to navigate websites, communicate via email, and have regular access to the internet (assessed by Participant self-report), to be able to independently use an online platform for telemedicine medical consultations in a private setting (assessed by Participant self-report).
Recruitment, consent, and data collection
Naïve participants diagnosed with advanced locoregional and metastatic cancer who have not previously received oncological and palliative treatment will be enrolled.
Eligible patients newly diagnosed with advanced cancer in need of palliative care will be offered the opportunity to receive palliative care interventions in this clinical trial. Study procedures will be presented to potential participants and their caregivers. The voluntary nature of the research will be highlighted, as well as the right to withdraw at any time without providing a reason or affecting their subsequent medical care. The participants will be given an informed consent form to study and as much time as necessary to consider enrollment, and their questions will be answered.
Signed informed consent will be collected from participants on-site during the baseline visit before the initial assessment and any study procedure.
Data collected up to the withdrawal time will be used as appropriate, unless the participant specifically requests their data not to be used. This process is in place to respect the participant’s privacy and ensure their comfort with the study.
After gaining informed consent, a baseline assessment will be done, including screening feasibility for the telemedicine arm. During this preliminary stage, before randomization, the researcher will assess if patients have access to a smartphone, a personal computer with webcam or tablet, email, a full internet connection, need help from caregivers for video calls for those who might need assistance, and if they are willing to accept video consultations.
All participants will complete the eHealth Literacy Scale (eHEALS) 48 at the baseline visit.
All feasibility criteria for the telemedicine group must be met to continue the screening procedure. Otherwise, the participant is not eligible for this study.
The inclusion and exclusion criteria for participants and caregivers that will be used to determine enrollment eligibility for this study are shown in Table 1a to d.
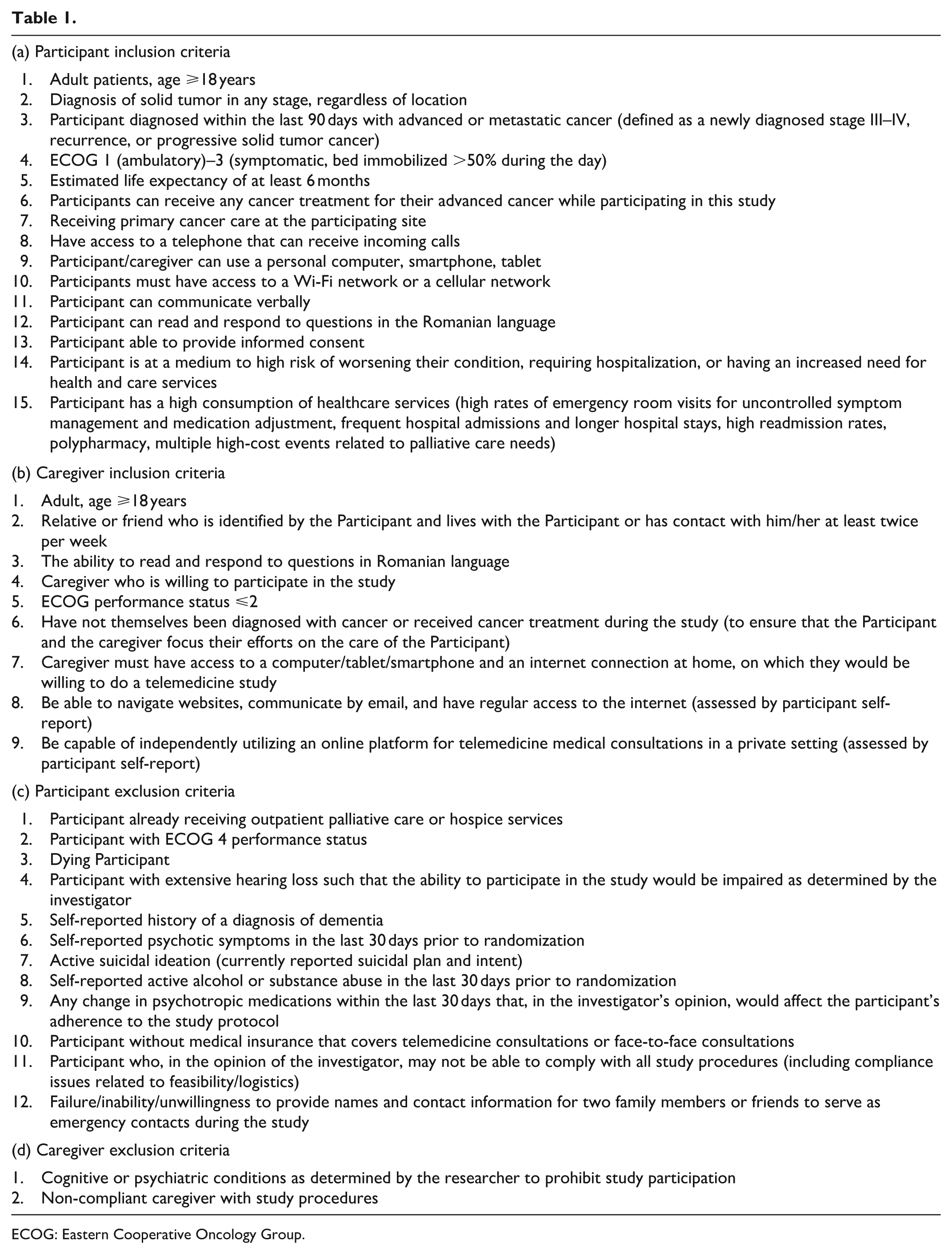
ECOG: Eastern Cooperative Oncology Group.
Randomization
Randomization will occur after informed consent is obtained at the baseline visit. It will be conducted using RANDOMIZER software for clinical trials (Institute for Medical Informatics, Statistics and Documentation, Medical University of Graz). Minimization as a randomization method will be used to give equal balance between groups. Weight loss, comorbidities, and cancer stage will be used as stratification variables.49–51 The outcome assessors (e.g., those scoring standardized measures and analyzing data) will be blinded to treatment allocation.
An independent researcher will generate and store the randomization code.
The participants will be randomized with a 1:1 ratio, without blinding, to one of the following arms:
Group A: Telemedicine consultations (intervention arm)
The experimental intervention will be delivered via Zoom and Video WhatsApp platforms via a secure internet connection.
The participants will choose what platform they would like to use based on their previous experiences with digital platforms.
Group B: Face-to-face consultation (control arm)
Patients randomized to this arm will continue with face-to-face consultations according to standard care.
Intervention and control
This study aims to estimate the effects of a palliative care consultation intervention among adults with advanced cancer delivered either as a remote (telemedicine) or face-to-face consultation, on changing symptom scores, quality of life, communication, participants’ experiences, e-Health literacy, emergency and unscheduled visits, adherence to treatment, retention rate, adherence rate, and the level of patient satisfaction.
Participants from both arms will receive three monthly scheduled palliative care interventions and also unscheduled visits whenever they need them, for a total duration of 3 months (12 weeks). The intervention will be administered by experienced palliative care physicians. To ensure intervention fidelity, interventionists will receive comprehensive training covering the study protocol and ethical conduct prior to the initiation of the study. This will include standardized operating procedures, confidentiality protocols, and telemedicine software usage. Throughout the study, periodic retraining sessions will be scheduled, regular communication with interventionists regarding the study protocol will be maintained, and a random sample of documentation will be reviewed to ensure adherence to palliative care content.
The baseline visit is face-to-face with all participants. Participants in the telemedicine group will be provided with a laptop or computer and a room (where they are alone) from where they can connect with the doctor who will administer the intervention. Participants from the telemedicine group will not meet the physician in person. In the control group, the visit is face-to-face.
Due to the moderate or severe intensity of symptoms that oncological patients frequently present within the outpatient clinic, visit one will occur on the same day as the baseline visit.
The first visit will take place according to the study arm to which the patient was assigned: face- to-face consultation for the control arm and using Zoom or WhatsApp platforms for the interventional arm. The content of the consultations will remain the same for both arms according to the national protocols. 52
Description of intervention
Demographic data, disease information, and social status will be obtained from the outpatient and electronic patient records.
After the participant, the caregiver (if the patient needs assistance), and the interventionist are connected, the reason for consultation, previously prescribed medication, treatment efficacy, symptom control, mental health status, social situation, spiritual concerns, and goals will be assessed by the physician.
All the participants will benefit from the following categories of interventions, depending on their needs, regardless of the study arm to which they have been assigned:
Communication of diagnosis, prognosis, and treatment options
Mediation of patient-caregiver communication
Symptom control for pain, fatigue, nausea, depression, anxiety, drowsiness, comfort, dyspnea, sweating, cough, constipation, hemorrhage, itching, secretions, dysphagia, appetite
Advice regarding care of wounds, bedsores, stomas
Patient and caregiver education
Psychological support (provided by the physician in charge)
Reports for obtaining social rights (sickness pension, disability pension)
Reports for obtaining devices provided without personal contribution by the health insurance system
Referral for spiritual assistance
Management plan
Referral for specialized palliative care service level III (provided by healthcare professionals who work solely in palliative care, and who have extensive knowledge and skills in this specialty)
Referral for hospitalization
Unscheduled consultations
To minimize missing data, we have incorporated scheduled rest breaks during questionnaire completion, and research staff will be available to provide support without influencing responses.
After every consultation, the patients from the telemedicine arm will receive an email or text message with the management plan, recommendations, and prescriptions as needed until the next visit.
If the patient had mild/moderate symptoms at the previous visit, the physician in charge would contact the patient and do a reassessment after 48–72 h.
In case of moderate/severe symptoms at the previous visit, the patient will be contacted by their physician in charge and reassessed after 24 h.
Unscheduled visits will take place whenever the patient or the caregiver requests it.
Emergency visit means an urgent encounter requiring the immediate decision-making and medically necessary action to prevent death or any further disability for patients in health crises (including labor and delivery). Such medical conditions are manifested by acute symptoms of sufficient severity (including severe pain) such that the absence of immediate medical attention could reasonably be expected to result in placing the patient’s health in serious jeopardy, serious impairment to bodily functions, or serious dysfunction of any bodily organ or part. To be considered urgent, the encounter must occur within 72 h from the onset of the presenting medical condition. 53
Unscheduled care encompasses healthcare services that arise unexpectedly, often due to accidents, sudden illnesses, or exacerbation of chronic conditions. This type of care is crucial for addressing immediate health concerns that cannot wait for a scheduled appointment. It is designed to provide timely medical attention to patients who may not have a life-threatening condition but require prompt treatment to prevent deterioration. 54
The method of conducting unscheduled visits will be the same as for scheduled visits. These visits will be conducted face-to-face for participants in the control group and via telemedicine for the intervention group. The attending physician will quantify the number of these visits for both groups.
The telemedicine application will not be used in emergencies due to safety restrictions.
According to standard care, all participants will be notified verbally and via email/text message of their next appointment.
Outcome measures
The following outcomes will be monitored during the study:
Primary outcomes
Patients’ Quality of Life will be assessed using the European Organization for the Research and Treatment of Cancer Quality of Life (EORTC-QLQ-C30) Questionnaire.
Changes in symptom control will be measured through the mean changes in distress score on the IPOS Questionnaire.
Patients’ satisfaction will be measured using the FAMCARE P 16 Questionnaire.
Secondary outcomes
eHealth Literacy.
Domain of intervention.
Number of patients satisfied with physician communication using Communication Assessment Tool (CAT).
Patients’ experiences with the care will be measured using the Patient Reported Experience Measures (PREMs) Questionnaire.
Number of emergency room visits.
Number of unscheduled visits.
Adherence to intervention will be estimated as the mean proportion of the scheduled consultations each participant completes.
Changes in medication adherence will be measured using the Morisky Medication – Taking Adherence Scale (MMAS-4).
Number of completed telemedicine scheduled visits.
Other study outcomes
Proportion of participants enrolled.
Number of participants ineligible or refusing to participate.
Frequency of participant ineligibility reason.
Frequency of participant refusal reason.
Retention rate.
Completion rate.
Measurement instruments
The patients’ vulnerable condition was an essential point to consider when selecting the questionnaires. The questionnaire length, difficulty, and measurement time points were carefully considered. When the patient cannot complete the questionnaires independently, the informal caregiver can assist. Table 2 provides an overview of the questionnaires used in the study.
Outcome measures.

Outcome measures
During the study, the following outcome measures will be used, as shown in Table 2.
1. ECOG Questionnaire (monthly visits and unscheduled visits)
ECOG is a tool for assessing the progress of a patient’s disease, how the disease affects the patient’s daily living abilities, and how to determine appropriate treatment and prognosis. 55
2. IPOS Questionnaire (monthly visits and unscheduled visits)
IPOS measures symptoms and concerns that matter to a patient and helps to provide the best care. It consists of 10 questions scored on a scale of 1–4 that assess a patient’s physical, social, psychological, and spiritual symptoms and needs. 56
3. EORTC-QLQ-C30 Questionnaire (monthly visits)
EORTC-QLQ-C30, a 30-item instrument developed by the EORTC, assesses various aspects of cancer patients’ quality of life, such as physical functioning, emotional well-being, and symptoms. 57
4. PREMs Questionnaire (monthly visits)
PREMs collect information on patients’ views of their experience while receiving care. This is an indicator of the quality of patient care, looking at the impact of the care process on the patient’s experience, for example, communication and timeliness of assistance. PREMS differ from satisfaction surveys in that they report objective patient experiences, removing the ability to report subjective views. 58
5. FAMCARE P 16 Questionnaire (monthly visits)
FAMCARE P16 is the only satisfaction assessment tool for outpatients with advanced cancers. It is structurally composed of 16 items, cohered into a single patient satisfaction factor. Each item is evaluated using a 5-point Likert scale (1–5; 1, very dissatisfied; 5, very satisfied), with a total score ranging from 16 to 80. 59
6. CAT (monthly visits)
CAT addresses patient satisfaction with key aspects of communication and interpersonal skills. Items are scored on a 1–5 scale, where 1 = poor and 5 = excellent, and a higher score indicates better communication skills. 60
7. eHEALS (baseline and visit three)
eHEALS is an eight-item measure of eHealth literacy developed to measure patients’ knowledge, comfort, and perceived skills at finding, evaluating, and applying electronic health information to health problems. 48
8. MMAS (first visit and visit three)
The MMAS consists of four items, with a scoring scheme of “Yes” = 0 and “No” = 1. The items are summed to give a range of scores from 0 to 4. 61
The study team will collect the measurements during scheduled and unscheduled visits. The Participant or caregiver will complete the outcome measures if the Participant needs help for completion, and will be sent to the study team by email or WhatsApp.
In case the patient requires hospitalization in a specialized level III unit, no subsequent assessments will take place during the study.
Regarding secondary outcomes, the attending physician will assess the number of visits to the emergency department reported by the Participant or caregiver, the number of unscheduled visits, the adherence to the intervention, and the number of completed telemedicine sessions.
Retention strategies
Participants will receive detailed information about the purpose, procedures, and benefits of the study from the first visit.
To facilitate adaptation to telemedicine consultations, we have opted for easy-to-use technology through intuitive platforms, easy to navigate, and accessible on various devices (smartphones, tablets, computers). Participants will be able to choose the platform they want to use in the study (Zoom or WhatsApp) based on their previous experience with these platforms. If necessary, participants will benefit from technical assistance to quickly resolve problems.
Participants will be provided with a smartphone or tablet during the study if they do not have the necessary technology to carry out telemedicine visits.
Participants will be able to choose appointment times that suit their schedule and their relatives’ and will have the opportunity to add appointments directly to their calendars.
Participants will not benefit from financial compensation for participating in the study.
Sample size calculation
The null hypothesis is that telemedicine consultations are inferior to face-to-face consultations for palliative care in outpatients diagnosed with cancer, with inferiority defined as a difference exceeding the non-inferiority margin of 5% in any of the following outcome measures: interventions efficacy, changing symptom scores, quality of life, communication quality, frequency of emergency and unscheduled visits, adherence to interventions and treatment, retention rate, adherence rate, and patient satisfaction with palliative care given.
A total of 128 participants (64 per arm) are required to prove that 95% lower limit of one-sided CI will be above the non-inferiority limit of 5%, with 80% power.
To account for an anticipated 33% missing data proportion at week 12 due to loss to follow-up, withdrawal, or death, the enrollment of 86 participants per group (172 total) is planned.
Briefly, a sample size of 172 patients (α = 0.05, power = 80%) is required to detect differences between the intervention and control groups.
Statistical analysis
Analysis of populations
Intention-to-treat
The intention-to-treat (ITT) population will include all randomized participants, analyzed according to their assigned study group, regardless of adherence or protocol deviations. This is the primary analysis set for the non-inferiority hypothesis.
Per-protocol
The per-protocol (PP) population includes participants who complete ⩾80% of scheduled intervention sessions and have no major protocol deviations affecting the primary outcome.
The PP analysis will be supportive, allowing assessment of the robustness of the ITT findings. Any deviations affecting adherence or outcome measurement will be documented and reported.
Primary outcome
The primary endpoint is the EORTC-QLQ-C30 GHS/QoL score at the primary follow-up point.
Non-inferiority will be concluded if the lower bound of the 95% confidence interval for the mean difference (intervention minus control) is greater than the prespecified – 10-point non-inferiority margin, consistent with published minimally important differences in advanced cancer populations for this scale.37–44
The primary outcome, EORTC-QLQ-C30 GHS/QoL, will be analyzed using linear mixed-effects models for repeated measures. The ITT population will serve as the primary analysis set. Models will include the baseline GHS/QoL score as a covariate to adjust for individual differences at study entry. Random intercepts will be included for each participant to account for intra-participant correlation across repeated visits. The PP population will be analyzed similarly as a supportive analysis to assess the robustness of the primary findings.
Secondary outcomes
Secondary outcomes include symptom burden (IPOS), participant satisfaction (FAMCARE-P16), communication assessment (CAT), PREMs, medication adherence (MMAS), and eHealth literacy (eHEALS).
Continuous outcomes will be analyzed using linear mixed-effects models, adjusting for baseline scores and key covariates (age, cancer stage, treatment).
Categorical outcomes will be analyzed using generalized mixed models (logistic or ordinal) for repeated measures.
Secondary outcomes are exploratory; results will be interpreted descriptively.
Handling of missing data and deaths
Given the high-risk nature of the palliative care population, missing data and deaths are anticipated.
Primary approach – Multiple imputation
Missing primary outcome data will be addressed using multiple imputation by chained equations under a missing-at-random assumption. Imputation models will include baseline scores, demographic and clinical covariates, and treatment assignment. Twenty imputed datasets will be generated, and results will be pooled using Rubin’s rules.
Deaths will be considered as terminal events. Longitudinal outcomes will be analyzed using joint models of repeated measures and time-to-death, allowing for informative censoring.
Sensitivity analyses will include: complete-case (available-case) analysis, worst-case/best-case scenarios, comparison with the PP population analysis, pattern-mixture models if data appear not missing at random. These approaches will evaluate the robustness of the non-inferiority conclusion.
Subgroup and exploratory analyses
The following predefined subgroups will be analyzed to evaluate the consistency of treatment effects across clinically relevant populations: cancer type, age group, and baseline performance status.
Exploratory analyses may examine associations between patient digital literacy (eHEALS) and adherence or symptom reporting.
Protocol deviations
Deviations will be prospectively documented and classified as major or minor.
Major deviations will exclude participants from the PP analysis but not from ITT analyses.
A summary of deviations and reasons will be included in the final report.
Interim analyses and monitoring
No formal interim efficacy analyses are planned.
Data completeness, retention, and safety will be monitored regularly by the study team, in accordance with institutional ethics requirements.
Statistical software
Analyses will be performed using SPSS (IBM Corp., version 28.0.1, Armonk, NY, USA), with additional procedures for multiple imputation conducted in R when required.
Reporting
Primary outcome results will include mean difference, 95% confidence interval, and p-value for non-inferiority. Both ITT and PP results will be reported.
Secondary outcomes will be presented descriptively with appropriate measures of central tendency and variability.
All analyses will adhere to Consolidated Standards of Reporting Trials (CONSORT) non-inferiority guidelines.
Ethical considerations
It can be challenging for vulnerable patients to participate in telemedicine visits and complete questionnaires actively as their condition worsens toward the end of the study period. Therefore, the researcher and the palliative consultation team will always consider the patient’s condition before conducting research. The informed consent form clearly outlines the advantages and disadvantages of participating for the patient and the informal caregiver. Ethical approval from the OncoHelp Association Ethics Committee will be obtained before any study procedures begin.
The Institutional Ethics Committee and Data and Safety Monitoring Board will review periodically data regarding timelines, enrollment rates, safety concerns, data availability, data quality, and protocol compliance.
Safety considerations/patient safety
Data forms, storage, management
All patient information and study source documents, including signed informed consent forms, completed eligibility checklists, and participant questionnaires, will remain confidential and will be retained at OncoHelp Association Ambulatory, in a locked cabinet complying with the current Good Clinical Practice (GCP) recommendations, and will be scanned and stored on a cloud-based system.
Since these records necessarily contain patient identifiers, only study staff will have access to them. Location, time, and date of the scanning of the document will be recorded.
No data will be stored on the researcher’s computer.
Data will be downloaded for analysis after removing all identifiers before downloading.
General Data Protection Regulation compliance
Data stored in the trial database will include participants’ initials, date of birth, and identification numbers. Only the minimum identifiable information will be collected to allow the management of the study.
Participants will provide a signed informed consent prior to participation in the study. This will include a patient information form and a notice explaining what data will be collected and where it will be stored. Also, they will give contact information to the study team.
Monitoring
Non-serious adverse events, serious adverse events, severe deteriorations, and withdrawals will be monitored.
Risks
The use of telemedicine is not the same as face-to-face consultation. There may be disruptions or distortions due to technical failures and/or interruptions during transmissions. Video and audio risks related to third parties could occur during the use of telemedicine, without the knowledge of the investigator.
Data collection
Baseline data collection will be conducted before the first telemedicine or face-to-face visit.
During subsequent visits, data collection will be conducted through electronic care records, and questionnaires will be completed at every contact. In case of missing data, a telephone interview will be conducted.
These data will be collected from all participants, including those who discontinue the study as long as they do not withdraw their consent to participate in the study.
Trial results will be reported in the ClinicalTrials.gov trial registry (Identifier: NCT06538350).
Discussion
This study protocol seeks to investigate the efficacy of outpatient palliative care interventions provided through telemedicine for patients with advanced cancer. It compares clinical outcomes in the intervention group with the control group. According to the study arm allocated to the participants, the intervention consists of three monthly and unscheduled palliative care consultations as needed, provided through telemedicine or face-to-face visits. Offering virtual specialist expertise via technology is an innovative way of improving complex care for patients with palliative care needs. A strength of our study is the robust design. We plan to conduct a randomized controlled trial, one of the first in palliative care in Romania, at least in telemedicine.
Furthermore, our primary outcome measures are quality of life, symptom burden, and participant satisfaction. Studies addressing ambulatory patients with advanced cancer and palliative care needs that have evaluated the applicability and efficacy of telemedicine are limited.
However, there are also several challenges in this study. The first challenge will be to enroll a sufficiently large sample to make sure that differences between the intervention group and the control group can be detected. If recruitment problems occur, the oncology consultation teams from other centers will also be involved.
Finally, this research project stimulates the collaboration between different levels of palliative care provided in hospitals and communities, strengthening the collaboration between oncology and palliative care settings to optimize the continuity of care.
In addition to the innovation of our daily practice, we also focus on technological innovation. Conducting innovative research is a big challenge in a rapidly changing world of technology.
Conclusion
The use of telemedicine interventions for patients with chronic diseases has increased considerably in recent years. However, we face insufficient information globally regarding the acceptance and efficacy of such treatment programs for patients with advanced cancer. This highlights the need for further research and exploration. It is essential to elucidate the extent to which our study participants accept these forms of medical intervention, the type of patient for whom they are appropriate, and how these interventions can be incorporated into standard care, as this will provide information on the transferability of these treatment options into routine clinical practice.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251408888 – Supplemental material for Efficacy of telemedicine for cancer patients in outpatient palliative care setting: Protocol of a randomized, open-label, non-inferiority study
Supplemental material, sj-docx-1-pcr-10.1177_26323524251408888 for Efficacy of telemedicine for cancer patients in outpatient palliative care setting: Protocol of a randomized, open-label, non-inferiority study by Alexandra Kovacs, Sheila Payne and Daniela Moşoiu in Palliative Care and Social Practice
Footnotes
Ethical considerations
This trial will be conducted in accordance with the protocol and consensus ethical principles derived from international guidelines, including the Declaration of Helsinki and Council for International Organizations of Medical Sciences international ethical guidelines, applicable ICH GCP guidelines, applicable laws and regulations, including regulation (EU) 536/2014. Ethical approval from the OncoHelp Association Ethics Committee will be obtained before any study procedures begin.
Consent to participate
Freely given written informed consent will be collected from participants on-site during the baseline visit before the initial assessment and any study procedure.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research receives support from the OncoHelp Association.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.