
Abstract
Background:
Palliative care, which aims to alleviate physical and emotional distress from cancer, is underutilized in many African healthcare systems. Therefore, there is a lack of data on the need and utilization of palliative care services among women with breast cancer in Ethiopia.
Objectives:
The goal of this study was to identify the level of need and utilization of palliative care services and identify associated factors among women in an oncology department of Hawassa comprehensive and specialized hospitals.
Design:
Hospital-based cross-sectional study.
Methods:
A total of 121 women age ⩾18 years old with breast cancer participated from 1 August to 30 October 2021. A hospital-based consecutive sampling technique was used. Data regarding the need and utilization of palliative care services were collected via questionnaire and interview, entered using EpiData 4.6.0.6, and analyzed by SPSS version 25. Variables with p < 0.25 were considered for multivariate analysis, and those with p < 0.05 indicate an association with palliative care utilization.
Result:
Seventy-two (59.5%) had worse utilization of palliative care services, with higher odds in rural areas (adjusted odds ratio = 11.82).
Conclusion:
The study findings indicated that more than half of the study participants had worse utilization of palliative care services, with rural living being a contributing factor.
Background
Based on the 2020 global cancer statistics, which analyzed data from 185 countries across 36 types of cancer, it was found that approximately one in eight cancer diagnoses is reported worldwide. Furthermore, the combined number of new cases in both genders was approximately 2.3 million. 1 About 685,000 women with breast cancer (BC) died in 2020, corresponding to one in every six cancer deaths in women. 2 The World Health Organization (WHO) supports collaborative teamwork to reduce mortality due to BC through early diagnosis and adequate treatment and management. 3
The incidence of BC in sub-Saharan Africa (SSA) is increasing, particularly in the prostate, breast, and cervix. The number of these cancers is estimated to double in the coming 20 years.4,5 In low- and middle-income countries (LMICs), the infrastructure and resources for routine screening mammography are often unavailable. In such low-resource settings, BCs are commonly diagnosed at late stages, and women may not receive adequate treatment, pain relief, or palliative care (PC) services. 6 In recent years, the rapid increase in BC in SSA has been attributed to changes in lifestyle, which include fewer children, reduced breastfeeding duration, changes in diet, increased alcohol intake, and obesity. 7
PC is a holistic approach that improves the quality of life of patients and families during life-threatening illnesses through the prevention and relief of suffering through the early identification and treatment of physical, psychological, and spiritual problems. 8 Globally, the need for PC is increasing due to the utilization of new technology to prolong the lives of patients with severe health conditions and unhealthy lifestyles, and the increased number of individuals with cancer and noncommunicable diseases.9,10
WHO 2020 reports that 40 million people worldwide are in need of PC, yet only 14% receive PC, implying that large numbers of people lack access to PC services. 9 In SSA, accessibility to PC services is limited, mainly due to a lack of workforce, a shortage of financial coverage for services, and a lack of understanding of the goals of PC delivery by clinicians, patients, and the public. 9 In 2019, over 55 million people died worldwide without access to basic PC. 11 The majority of these deaths occur in LMICs, where many people do not have access to basic PC. Without access to PC, many people in LMICs die in pain and with significant distress. 12
In one study, about 65% of cancer patients with advanced stages in Addis Ababa tertiary hospital did not receive adequate pain management. 13 Tikur Anbessa Specialized Hospital (TASH) is administered by Addis Ababa University and is located in Addis Ababa, the capital city of Ethiopia. It has five beds that are designated for PC services and cancer treatment. In Ethiopia, there is an extensive need for PC as the burden of noncommunicable diseases and cancer is increasing. Lack of PC services during the advanced stages of cancer creates significant symptom burden, psychosocial distress, and poor quality of life. 14 About 9 of 10 (89.8%) respondents to a survey reported problems with accessibility to PC services among adult cancer patients in Ethiopia at TASH. 15
To the best of our knowledge, there has been no study conducted regarding factors affecting the need and utilization of PC services among adult women with BC at Hawassa University Comprehensive and Specialized Hospital (HUCSH) oncology department, so this study was aimed at assessing the level of need and utilization of PC services and identifying factors affecting their utilization among Ethiopian women.
Methods
Study design
A cross-sectional study design was utilized in a hospital setting among women with BC.
Setting
The study was conducted at the oncology unit of HUCSH, the only primary cancer treatment center in the Sidama Region. According to registration records, approximately 484 women with BC visit the oncology unit annually. The PC services available in the oncology unit include face-to-face counseling, psychotherapy, a pain treatment center, and chemotherapy. These services are delivered primarily by physicians and nurses. Patients can access PC services in both inpatient units and the outpatient department, but a referral is required. Only women with health insurance can utilize PC services without payment. Data was collected at the time of the oncology unit visit between 1 August and 30 October 2021. The data collection tool was adapted from previous studies conducted outside the country and was pretested to ensure its suitability for the current study. 16 The tool was prepared in English and translated to an Amharic and Afaan Oromo version with the assistance of a language expert. The assessment tool contained four parts with closed-ended questions. Two data collectors and two supervisors facilitated the data collection process. Data collectors were selected based on their qualifications (BSc nurses) and experience, and study training was given for two consecutive days by the principal investigator. Based on the willingness of the study participants, data collectors reviewed the charts of the patients to determine who was included and excluded at the time of subject selection. Part one is related to sociodemographic factors with six items (age, place of residence, educational status, monthly income, marital status, and occupation). Part two is related to clinical factors with three items (stage of BC, physical wellbeing, and social wellbeing). The third part assessed the need for PC with 10 items (counseling service at the hospital, library of books and videos, relaxation classes, drop-in counseling and support service, 24-h telephone support and cancer advisory service, home nursing service, home cleaning service, home gardening service, respite care, and monetary allowance for travel and treatment), and the last part assessed utilization of 10 items of PC services.
Participants
All patients visiting the oncology unit were recruited during the data collection period. All women aged ⩾18 years old were included, while critically ill patients were excluded. The study participants were selected using a consecutive sampling technique. Every subject meeting the inclusion criteria was selected based on the hospital registration record until the targeted sample size was reached. The study participants were invited to participate when they visited the oncology unit. The researcher gained permission from the study setting with a cooperative letter and copies of an ethical approval letter. Respondents were informed about the objective and purpose of the study, and verbal and written consent was obtained from each respondent. Besides, all the study participants were informed that they have a full right to participate or decline to participate in the study, and the study participants were assured of the attainment of confidentiality for the information obtained from them.
Variables
In this study, age was classified according to the Ethiopian Ministry of Health adult age classification that was used in hospitals as 18–29, 30–39, 40–69, and ⩾70. The monthly income of the participants was categorized depending on their median income as <600 Ethiopian birr (ETB) and ⩾600 ETB. The need for PC services was categorized into four levels: no need, little need (low desire for better access to services), moderate need (moderate desire for better access), and high need (strong desire for better access). Utilization of PC services is defined as the access and subsequent implementation of PC services, either one-time only or ongoing care, by a PC provider. The minimum duration for ongoing care is 3 or 4 months. 17 Utilization of PC service was categorized as better and worse utilization. Participants who scored below the mean for utilization were considered to have worse utilization, while those who scored at or above the mean were considered to have better utilization. The utilization of PC services has been operationalized for participants who have utilized PC at any time in the past. Physical wellbeing was categorized as either yes or no, with ‘yes’ indicating good energy and/or no nausea and ‘no’ indicating a lack of energy and/or nausea. Social wellbeing was also categorized as either yes or no, with ‘yes’ indicating feeling close to partners and friends and receiving support from them and ‘no’ indicating a lack of at least one of these factors. The income of the study participants was classified according to the median.
Data sources/measurement
The data collectors completed the information related to sociodemographic, physical and social wellbeing, need for, and utilization of PC services through face-to-face interviews. Information related to the stage of BC was collected through a medical record review. The questionnaire was pretested on 5% of the sample size at another hospital, TASH in Addis Ababa, 2 weeks before actual data collection at the study site in Hawassa to check for acceptability and consistency. After reviewing the results of the pretest, modifications to the questionnaire were performed for clarity, sensitivity, and completeness. Continuous supervision and daily checking of the collected data were performed by the principal investigator. The reporting of this study conforms to the Equator Network guideline statement in reports of cross-sectional studies (Supplementary File). 18
Bias: Data were collected through face-to-face interviews to prevent measurement bias, and a pretest was done to improve the quality of the data. Participants were informed about the objectives and purpose of the study, and they voluntarily participated to avoid response bias.
Study size
The sample size for the study was calculated using a single population proportion formula, which is used to determine the minimum sample size required to estimate the true proportion of a population. The formula is as follows: n = Z(∂/2)2 × p(1 − p)/w2, where p is the proportion of accessibility and utilization of PC (which was assumed to be 50% since no previous local study had been conducted in Ethiopia), Z is the level of confidence [1.96 for a 95% confidence interval (CI)], w is the margin of error (5%), and n is the minimum sample size required. Using this formula, the minimum sample size was calculated to be 384. However, all women who were visiting the oncology unit and met inclusion criteria within 3 months (121) of the study period were included in the study.
Statistical methods
After the results of the pretest were reviewed, the questionnaire was modified to improve its clarity, sensitivity, and completeness. Data collectors and supervisors received 2 days of training on the objectives of the study. Continuous supervision and daily checks of the collected data were performed by the supervisor to ensure accuracy and consistency. Data for the study was coded, entered, and cleaned using EpiData version 4.6.0.6, and then exported to SPSS version 25 for analysis. Descriptive statistics, including frequencies and percentages, were used to summarize the characteristics of the study participants, and continuous variables were expressed as means and standard deviations. A logistic regression model was used to analyze the data, with bivariate logistic analysis performed to identify candidate variables for multivariate logistic regression at p values <0.25. The odds ratio and corresponding 95% CIs were used to indicate the presence and strength of any associations, with a p value of <0.05 in the multivariate analysis considered significant.
Results
A total of 121 women participated in the study, yielding a response rate of 100%.
Sociodemographic characteristic of participants
The mean ± standard deviation age of the participants was 50 (14.439). A total of 71 (58.7%) were living in rural areas and 61 (50.4%) were attending primary school (Table 1).
Sociodemographic characteristics of women with breast cancer visiting oncology unit at HUCSH, Hawassa, Sidama, Ethiopia, 2021 (n = 121).

ETB, Ethiopian birr; HUCSH, Hawassa University Comprehensive and Specialized Hospital.
Clinical characteristic of participants
Out of the 121 patients in the study, the majority were diagnosed with stage 3 disease. A total of 66 (54.5%) of the patients reported that they did not experience any physical wellbeing (Table 2).
Clinical characteristics of the study participants (n = 121).

Characteristics of need of PC service among participants
Among the study participants, 83 (68.6%) reported a moderate need for counseling services. A total of 69 (57.0%) reported a high need for home nursing services and 67 (55.4%) had a high need for a monetary allowance for travel and treatment (Table 3).
Need for to palliative care services (n = 121).

Characteristics of PC service utilization of participants
A total of 72 (59.5%) of the study participants had worse utilization of PC services (Figure 1). As much as 93 (76.9%) had not ever utilized community-based cancer support groups and ninety-nine (81.8%) had not utilized this service in the past 12 months. About 100 (82.6%) had not ever utilized internet-based cancer support groups and 99 (81.8%) had not utilized the service in the past 12 months. A total of 37 (30.6%) had ever utilized and 84 (69.4%) had not ever utilized community health nurses for cancer patients (Table 4).

Level of utilization palliative care services among the study participants visiting oncology unit at HUCSH, Hawassa, Sidama, Ethiopia, 2021 (n = 121).
Utilization of palliative care services (n = 121).

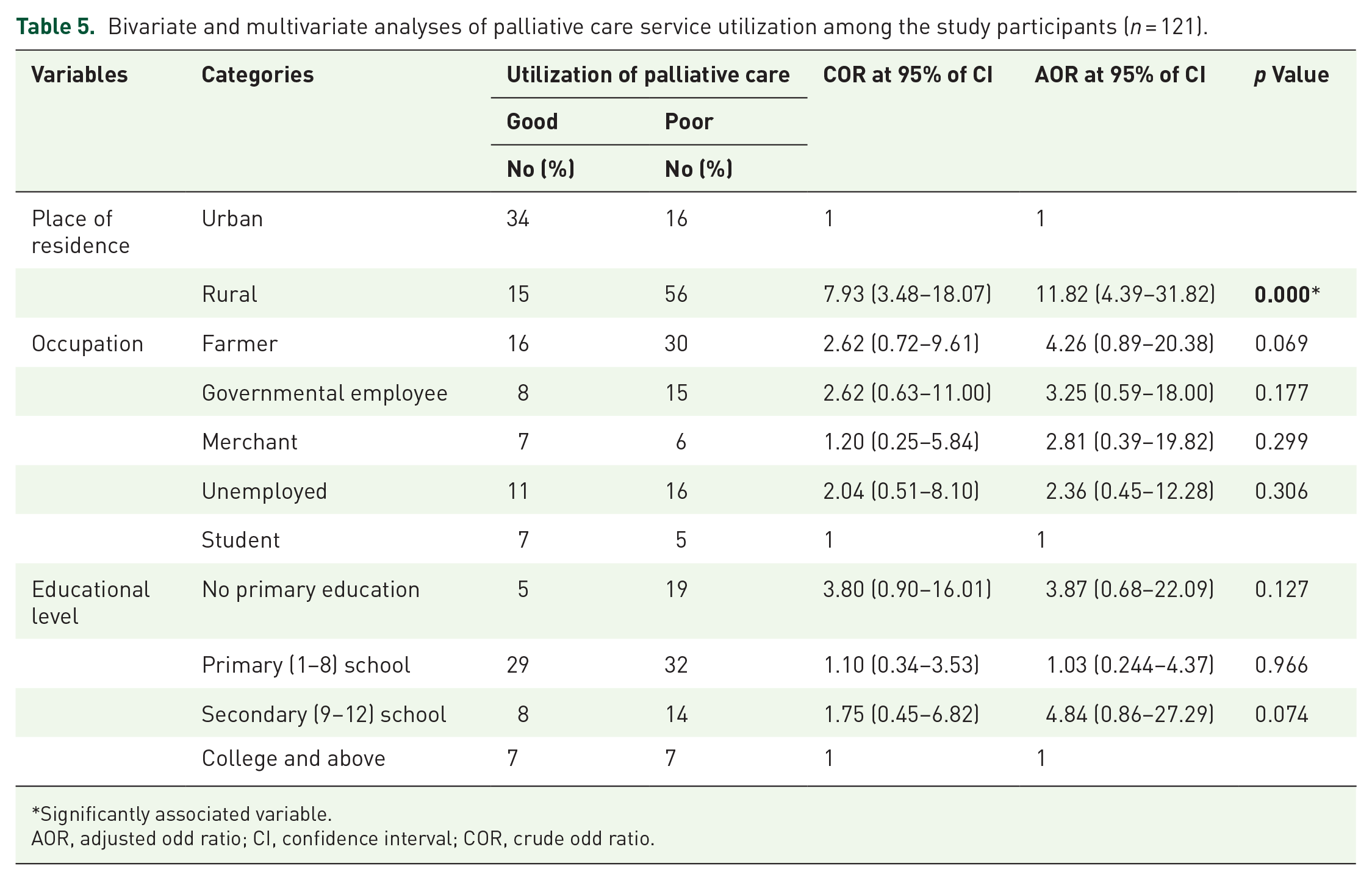
Bivariate and multivariate analyses of utilization of PC service among participants
In the bivariate analysis, factors that were considered for inclusion in the multivariate analysis at a p value of less than 0.25 included place of residence, occupation, and educational level. However, in the multivariate logistic analysis, the only independent predictor of worse utilization of PC services at a p value of <0.05 was a rural residence. Women with BC living in rural areas were 12 times [adjusted odds ratio (AOR) = 11.82, 95% CI = 4.39–31.82] more likely to have worse utilization of PC services compared to those living in urban areas (Table 5).
Bivariate and multivariate analyses of palliative care service utilization among the study participants (n = 121).
Significantly associated variable.
AOR, adjusted odd ratio; CI, confidence interval; COR, crude odd ratio.
Discussion
This study aimed to evaluate the need and utilization of PC services as well as the factors that affect women with BC at HUSCH in Sidama, Ethiopia. This study found that 72 (59.5%) of the study participants had worse utilization of PC services. This finding was lower than that of a study conducted among metastatic BC patients in United States hospitals, which found a rate of 78.1%. 19 This might be due to differences in study design and study population. However, the study finding was higher than the study conducted in three home-based PC programs in Addis Ababa and Yirgalem town, which revealed that 7 (20.6%) of participants claimed to have worse utilization of PC service. 13 This might be due to differences in the nature of the study, the study setting, and the study population. The study conducted in Addis Ababa and Yirgalem was a qualitative and home-based study.
Our research is different from previous studies, as we specifically concentrate on women with BC and their utilization of PC. This focus is crucial for patients, as it focuses on the actual use of PC services. This study lacks cultural and social factors that have significantly impacted individuals’ attitudes toward illness, treatment-seeking behavior, and acceptance of PC. A cross-sectional study only provides a snapshot of the findings and fails to capture change over time. So future researchers are advised to do longitudinal studies and include cultural factors for better findings.
In a multivariate analysis, it was found that rural residency was significantly associated with worse utilization of PC. Women living in rural areas were 12 times more likely to experience worse utilization of PC than urban residents, with an AOR of 11.82 and a 95% CI of 4.39–31.82. This result is in line with a study conducted in Ontario, Canada, 20 Australia, and 21 Ethiopia. 22 One possible explanation for this association between rural residences and worse utilization of PC services could be that living in rural areas is often associated with a lack of awareness causes misunderstandings and prevents timely intervention and symptom management. Distance from healthcare facilities and the difficulty of transportation services, beliefs, and attitudes are also reasons why people living in rural areas worse utilize PC services. Rural residents might have a fear of facing the reality of a serious illness, which can prevent patients from seeking PC early. Some patients may decline PC due to cultural norms or religious issues. Fundamental strategies include educating patients, involving community and religious leaders, and collaborating with health extension workers to raise awareness.
Strength and limitation
This study had some limitations, including a lack of existing literature on the utilization of PC services in the area and the factors affecting their use, which limited the ability to design the study and compare outcomes. Additionally, the number of patients included in the study through consecutive sampling may have been affected by seasonal variations.
Conclusion
This study found that 72 (59.5%) of women had worse utilization of PC services. Living in a rural area was identified as a factor contributing to worse utilization of PC services. These findings suggest that HUCSH should develop strategies to improve utilization, such as increasing awareness among patients and the community about the importance of PC and identifying the reasons for worse accessibility to these services. Hospital boards also have a responsibility to work with health professionals, families, and patients to increase accessibility to PC, which directly affects their utilization. Collaboration between home care nursing services and community-based services can have a direct impact on the utilization of PC.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241253625 – Supplemental material for Factors affecting need and utilization of palliative care services among Ethiopian women in an oncology department: A hospital-based cross-sectional study
Supplemental material, sj-docx-1-pcr-10.1177_26323524241253625 for Factors affecting need and utilization of palliative care services among Ethiopian women in an oncology department: A hospital-based cross-sectional study by Deriba Fetene, Lesley Taylor, Betty Ferrell, Bedilu Deribe, Jabir Abdella and Amdehiwot Aynalem in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524241253625 – Supplemental material for Factors affecting need and utilization of palliative care services among Ethiopian women in an oncology department: A hospital-based cross-sectional study
Supplemental material, sj-docx-2-pcr-10.1177_26323524241253625 for Factors affecting need and utilization of palliative care services among Ethiopian women in an oncology department: A hospital-based cross-sectional study by Deriba Fetene, Lesley Taylor, Betty Ferrell, Bedilu Deribe, Jabir Abdella and Amdehiwot Aynalem in Palliative Care and Social Practice
Supplemental Material
sj-sav-3-pcr-10.1177_26323524241253625 – Supplemental material for Factors affecting need and utilization of palliative care services among Ethiopian women in an oncology department: A hospital-based cross-sectional study
Supplemental material, sj-sav-3-pcr-10.1177_26323524241253625 for Factors affecting need and utilization of palliative care services among Ethiopian women in an oncology department: A hospital-based cross-sectional study by Deriba Fetene, Lesley Taylor, Betty Ferrell, Bedilu Deribe, Jabir Abdella and Amdehiwot Aynalem in Palliative Care and Social Practice
Footnotes
Appendix
Acknowledgements
Special appreciation goes to Hawassa University, School of Nursing, for their support in the accomplishment of this study. We are grateful to the healthcare workers and the women with breast cancer who participated in our study.
Declaration
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.