
Abstract
Objective
This study sought to document Oklahomans knowledge, attitudes, and behaviors regarding palliative care; this paper focuses on subjects stated preferences for where they would choose to die.
Design
Quantitative study used a random state-wide telephone sample of Oklahoma residents.
Subjects
Data from 804 residents in the State of Oklahoma between November and December (2005).
Results
An overwhelming majority of the respondents (80%) reported preference to die at home in the event that they suffer a terminal illness. The proportion of respondents under the age of 65 who preferred to die at home (80.9%) was slightly higher than those aged 65 and over (74.8%). Also, while 81.4% of the female respondents reported preference for dying at home, 75.8% of the male respondents shared such preference (P < 0.05). More married respondents (82.7%) than non-married respondents (74.7%) reported preference for dying at home (P < 0.01). A significant association (P < 0.05) between income level and preference for dying at home was noted. While 84.3% of those with income level at $21,000 or more reported reference for dying at home, 76.4% of those with income below $21,000 reported the same preference.
Conclusions
This paper offers insight into factors that influence Oklahoman's stated preferences for site of death that can assist the statewide agenda in the planning and provision of palliative care. This information can be adapted in other states or countries to determine palliative care needs.
Introduction
According to the National Consensus Project for Palliative Care (2004), palliative care is integral to all health care delivery system settings and should ensure coordination, communication and continuity of palliative care across institutional and home care settings. The interdisciplinary care team works to prevent crises and unnecessary transfers for patients at the end of their lives (2004). This also includes helping patients to die in the setting of their choice and ensuring the health care system supports these choices. Unfortunately, there is little empirical evidence (Tang, 2003) to give insight into where people prefer to die and what factors influence that choice.
Mortality statistics from 2001 indicate that 49% of deaths occurred in hospitals, 23% in nursing homes, 23% in residences, and 5% elsewhere, including those declared dead on arrival at the hospital (Teno, 2007). About 55%–60% of persons older than age 65 die in the hospital. Findings from The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments (SUPPORT) Investigators (SUPPORT, 1995) sustain the national polls documenting that while most people prefer to die at home, the majority died in the hospital. The number of patients dying in the hospital varied between 29% and 66% in the five research sites across the U.S., with 23%–54% of these cases being Medicare beneficiaries (Teno, 2007).
Investigators found that measures of hospital availability and use were the most powerful predictors of the place of death. The chance of dying in a hospital was increased for residents of regions with a greater availability of hospital beds. The risk was decreased in regions that had greater nursing home and hospice availability and use. Variations within groups were not explained by socio-demographic, clinical, or patient preferences (Bookbinder, Kiss et al. 2006).
Berger (Berger, Pereira et al. 2002) and colleagues completed a literature review of social and cultural determinants as they relate to the settings where individuals in the United States die. Their paper outlines possible factors for choices of settings at the end of life: (1) sociodemographic characteristics of the patient, (2) characteristics of available support networks, (3) measures of functional characteristics and degree of dependence on support network, and (4) health system and institutional factors. (Berger, Pereira et al. 2002) With the exception of diagnosis (cancer) there is no other empirical data that agrees on the factors associated with site of death (Enguidanos, Yip et al. 2005). One study indicates that being older, white, married, and having a cancer diagnosis is associated with dying at home (Pritchard, Fisher et al. 1998). Another concludes that significant predictors of dying at home are having a high school degree, moderate physical decline in the five months before death, and being widowed or unmarried (Weitzen, Teno et al. 2003). Regarding race and ethnicity, one study documented that black and Latinos were more likely to die in the hospital and whites to die at home (Iwashyna and Chang, 2002).
Bruera (Bruera, Sweeney et al. 2003) studied place and predictors for site of death among Houston area residents with cancer. They documented that 52% of the patients died in the hospital, 35% died at home. The logistic regression model documented that patients were more likely to die in the hospital if they were black (OR 1.5), had a hematological cancer (OR 2.7), and county of residence (i.e. Harris County, OR 1.6) (Bruera, Sweeney et al. 2003). This study looked at actual cancer deaths in only one city and the authors concluded that more study is needed regarding understanding patient preferences regarding place of death.
A qualitative study from Scotland documents that the interviewed patients really had not considered where they wanted to be cared for at the end of their life, or did not think that they had a choice (McCall and Rice, 2005). The authors were also unable to determine why home was the preferred site of death, suggesting that it may be more of an aversion to the hospital than preferring to die at home. The authors concluded that the issue is more about initiation of the conversation regarding end of life options and a sensitive exploration of patients and their families’ choices (McCall and Rice, 2005).
Tang (2003) conducted a qualitative study in Connecticut (n = 180) of people with a cancer diagnosis to elicit responses regarding preferences for place of death. 87% of the respondents preferred to die at home and they rated this as very important to them. It is of interest that subjects indicated that if dying at home placed a burden on their family that they would be willing to alter their preference for site of death (Tang, 2003). An association between site of death and physical decline was established by Weitzen (Weitzen, Teno et al. 2003), where a decline in the last 5 months of life was associated with dying at home or in a nursing home. Earlier functional loss was associated with dying in a nursing home (Weitzen, Teno et al. 2003).
Admission to hospice services does not guarantee that the patient will die in their home. Situations change that may necessitate transfer to the hospital or nursing home. Evens (Evans, Cutson et al. 2006) studied the reasons for transfer from home hospice to an inpatient facility and the preferences for site of care and death. Semi-structured interviews with 18 caregivers yielded 4 categories of reasons that patients were transferred. These included an acute medical event, symptoms that could not be controlled, imminent death, and safety issues. The transfer to the inpatient facility was seen by family members as necessary to maximize quality and quantity of life (Evans, Cutson et al. 2006).
A cross-sectional prevalence survey of older adults (n = 219) living in a continuing care retirement community (CCRC) in North Carolina was carried out to document death-related planning and preferences for site of death (Hays, Galanos et al. 2001). Forty percent of the respondents’ indicated that they had moved to the CCRC as part of their death-related planning. The majority had a clear preference for where they would prefer to die and most wanted to die on the CCRC campus. The authors suggest that a discussion regarding site of death be included in routine end of life planning (Hays, Galanos et al. 2001).
Ethnicity also plays a role in variations related to site of death. Enguidanos (Enguidanos, Yip et al. 2005) studied Medicaid and Medicare recipients in California. They documented that blacks and Latinos were significantly more likely than whites to die at home but were less likely to receive hospice care.
The discrepancy between where people say they want to die and where they actually die warrants further study; this disconnect between preference and reality may result in an unnecessary burden on the dying patient and their family. This study sought to quantitatively document Oklahomans knowledge, attitudes, and behaviors regarding palliative care. The aim of this paper is to build on previous studies and to go one step further to investigate Oklahoman's stated preferences for where they would choose to die and what factors influence their preference.
Methods
Data source
The purpose of this survey was to gauge levels of public awareness about end-of-life issues in general and to establish a baseline for subsequent monitoring of attitudes toward end of life care. Data were collected between November and December (2005) by trained researchers at the University of Oklahoma Public Opinion Learning Laboratory (POLL) and received IRB approval from the University of Oklahoma. This quantitative study used a random telephone sample of all Oklahoma residents with telephones and is the first survey to research one entire state on these issues. The sample was purchased from Survey Sampling, Inc. and was screened of many non-residential numbers (such as businesses and non-working telephone numbers) by Survey Sampling, Inc. in order to reduce the amount of time spent on this task by the interviewers. Eight hundred and four (804) people completed interviews were obtained among residents with a 58% response rate and a margin of error of +/– 3.5% at a 95% confidence level. Overall, 4,000 numbers were released (dialed) from the sampling pool, and 15,353 call attempts were made by POLL interviewers to complete interviews. These data were weighted by age group in order to represent the state as accurately as possible.(Matzo, Hijjazi et al. 2008)
The survey was adapted from a survey of public awareness completed in South Australia (Author, 2001), cognitive tested, and further revised. Specific wording of the questions to elicit preferences for site of death were: “If you were terminally ill, where would you prefer to die?” and “If you were dying, what concerns, if any, would you have about being cared for at home until you died?” Questions were open-ended and unprompted to elicit definitions in the respondents’ own words and sequenced so as to minimize bias from one question to another. Responses were reviewed by both researchers and consensus was reached regarding recoding categories. For purposes of this paper, responses have been grouped together by topic.
Responses regarding preference for place of death were grouped into “preference to die at home” (80%) and “preference to die somewhere else” (20%). Some of the alternatives to dying at home that respondents answered were “somewhere bass fishing”, “on the beach”, or “a hospice program facility, but not at home”. Responses regarding the concerns about being cared at home were grouped into “availability, quality, and level of care” (38%), “burden on the family (physical and/or financial)” (30%), and “other concerns” (7%). Exemplars for ‘availability, quality, and level of care’ are “don't want to die at home and worry about a non-sterile environment”, “pain management, trying to be as comfortable as possible”. Burden on the family (physical and/or financial) were expressed in statements such as “don't want my family to see me suffer”, “financial, and time the family has to spend on me”, and “don't want anyone to give up their life for me”. Other concerns that were mentioned were, “want it to be sudden”, and “not to be cared for at home, since the family has to be there after I am gone”.
Data analysis was conducted using bivariate and multivariate techniques utilizing the SPSS software package. We assessed differences in reported preference to die at home versus preference to die elsewhere based on respondents’ demographics and experiences. Then a backward stepwise logistic regression was used to identify the key predictors of preference to die at home.
Findings
The weighted sample consisted of 792 respondents. The majority of the respondents were females (70%), white (81%), African American (6%), and Native American (7%). Twelve percent were age 18–24, 39% age 25–44, 30% 45–64, and 19% over age 65. Sixty-two percent were married, and 80% stated that their religion was Protestant. When asked about the preferred place of death, eighty-one percent (n = 630) stated that their preferred place of death was their home. Table 1 shows frequency distributions of sample characteristics.
Sample Characteristics (N = 792).
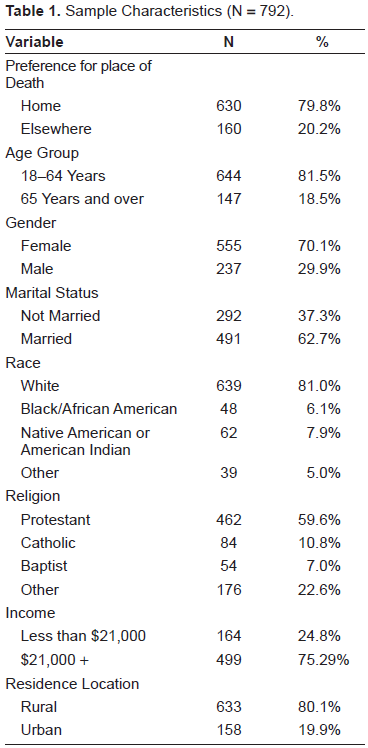
Table 1 and 2 include respondents’ characteristics and Table 3 includes comparison between those who preferred dying at home and those who preferred dying elsewhere other than home. The proportion of respondents under the age of 65 who preferred to die at home (80.9%) was slightly higher than those aged 65 and over (74.8%).
Sample findings (N = 792).

Preference for place of death (weighted N = 792).

Also, while 81.4% of the female respondents reported preference for dying at home, 75.8% of the male respondents shared such preference (P < 0.05). More married respondents (82.7%) than non-married respondents (74.7%) reported preference for dying at home (P < 0.01). A significant association (P < 0.05) between income level and preference for dying at home was noted. While 84.3% of those with income level at $21,000 or more reported reference for dying at home, 76.4% of those with income below $21,000 reported the same preference.
In terms of concerns about dying at home, we selected respondents who had any concerns and grouped them into three categories and compared the groups based on selected respondent characteristics (Table 4). Women were more likely than men to be concerned about the burden of care on the family. A similar finding was noted among respondents who had a family member die of a terminal illness. On the other hand, respondents who were hospitalized in the previous 12 months were more likely to be concerned about the availability, quality, and level of care at home.
Concerns about Dying at Home (Weighted N = 588).

Table 5 shows predictors of preference of dying at home. In the full model, gender and hospitalization within the past 12 months were the only significant predictors. In the reduced model, income and health status were significant as well. Male respondents were 40% less likely than female respondents to prefer dying at home. Respondents with income under $21,000 were also about 40% less likely to prefer dying at home compared to respondents with higher levels of income. Respondents in good to excellent health were more likely to prefer dying at home than those with poor to fair reported health. And finally, respondents who were hospitalized in the previous 12 months were twice likely to prefer dying at home compared with those who were not hospitalized during the same period.
Predictors of Preference for Dying at Home—Logistic Regression (Weighted N = 792).

Limitations
This study reflects the views of one state in the United State. The participants were randomly chosen and may or may not have a terminal illness at the time of the interview. Responses should be considered hypothetical rather than informed relative to an actual terminal diagnosis. Responses may have been different if the population of study had a terminal diagnosis at the time of interview.
Discussion
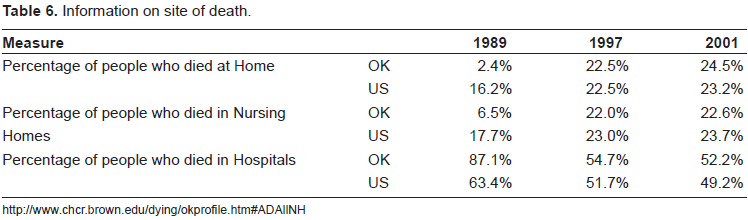
This article is the first that the authors are aware of to document preferences for site of death from the viewpoint of one entire state. The majority of Oklahomans in this study stated that their preferred site of death was home (80%), yet in 2001, only 24% of Oklahomans died at home (Table 6). In that same year, 52% of Oklahomans died in a hospital, higher than the national average for that year. A disconnect exists between Oklahoman's preferences and where they actually die. Oklahoman's preference to die at home is consistent with published studies that indicate that the preference to die at home is almost a universal desire (Putnam, McDonald et al. 1980; Zusman and Tschetter, 1984; Townsend, Frank et al. 1990; Weitzen, Teno et al. 2003; Grinyer and Thomas, 2004; Thomas, Morris et al. 2004; Brazil, Howell et al. 2005).
Information on site of death.
Yet, there are some subgroups of the population that prefer a hospitalized death. This study provides some insight into the factors that influence Oklahoman's preferences for site of death. These analyses indicate that younger age, gender (female), being married, and having income greater than $21,000 are the strongest predictors of preferring to die at home.
Of added interest are the reasons that respondents state that they had concerns about dying at home. Women and having had a family member die of a terminal disease were most likely to report concerns regarding being a burden at the end of life. It would appear that having had experience with end of life care raises concerns about being a burden if they were to die at home.
The second issue raised by respondents was the quality of care that they would receive if they were to die at home. The comments that respondents’ made regarding this concern indicate that they would receive better care in the hospital. This was a significant concern for those who had been in the hospital during the last twelve months. Despite this concern, in the regression analyses this group was still twice as likely to prefer to die at home as those who had not been hospitalized in this same period. This finding is like a double-edged sword. Having been hospitalized in the last year, this group has some experience with the amount and intensity of care that can be needed in the hospital, yet, having been in the hospital they know that they do not want to die there.
Conclusions
Where a person dies is influenced more by the characteristics of the health care system where they live and less by individual preferences and characteristics. (Pritchard, Fisher et al. 1998) The findings from this study not only document preferences for site of death, but also documents perceived barriers and issues to having a home death. For those families who are motivated to helping a loved one die at home, the issues and concerns that respondents raised can be used to develop programs and services to bridge the gap between where people want to die and where they actually do. Clearly family support and quality of care that can be delivered in the home to people at the end of their lives are two issues that need to be addressed. Understanding the wishes and needs of a community regarding preferences for site of death helps community planners modify provider practices and resource availability (Pritchard, Fisher et al. 1998).
One aspect of advance care planning is the discussion regarding advance directives and healthcare proxies. The findings from this study suggests that a discussion regarding preferences for site of death and perceived barriers to actualizing that wish also become a part of routine end of life planning. If health care practitioners facilitate a discussion regarding issues and concerns regarding dying at home as well as issues that family members themselves may have regarding caring for their family, then they can plan in advance what support and services are needed to overcome the barriers. Additionally, this discussion can allow the family to talk about the possibility that their loved one may become too sick to continue to be cared for at home; allowing them to know in advance that their terminally ill family member understands this and supports transfer to the hospital if it should be necessary.
Important findings from this study are the characteristics of Oklahomans who do not want to die at home. Health care practitioners should be aware of what subgroups of the population might be more prone to preferring to die in the hospital and discuss this possibility with them. These factors may influence the decisions that people will make at the end of life and these demographic and health status variables should prompt the practitioner to include this discussion in end of life planning.
In order to help patients have a good death, defined by the Institute of Medicine (1997) as “one that is in accord with the patients’ and families’ wishes,” health care practitioners need to address with dying patients and their families preferences for where they want to die and what barriers they perceive to this occurring. This professional guidance can help patients discuss their concerns and let family members know if and when they would find it acceptable to be transferred to the hospital if their condition warranted it. Having the discussion, helping patients make plans, and having the supportive services available when needed will help to bridge the gap between desire and reality when it comes to where people die.
Note
This study was funded by the Hospice Foundation of Oklahoma, Inc.
Disclosure
“No competing financial interests exist.”