
Abstract
Introduction
White coat ceremonies (WCCs) in medical school mark the transition of students to medicine, beginning their professional identity formation as a physician. However, a literature/web search revealed a paucity of residency-focused WCCs.
Methods
A 90-minute Family Medicine Residency (FM) WCC was designed to support residents’ professional identity formation as a specialty physician. Through faculty narratives and brief histories of the white coat and the specialty, the WCC concludes with new residents donning their specialty embroidered white coats. A brief e-survey was sent to attendees, and WCC leaders were debriefed to determine the value and key elements of WCC.
Results
Seventy-nine percent of survey respondents (34/43) agreed that the WCC is an important transition event for residents’ identity while reaffirming FM values for faculty/staff. WCC leaders identified critical steps for initiating a WCC.
Conclusion
A resident WCC formally marks the transition to specialty physician identity.
Lessons Learned
Ceremony structure will evolve over time.
Introduction
The bestowal of the white coat by a member of the medical profession marks a student's entrance into medicine and its associated roles, responsibilities, and values. 1 The white coat ceremony (WCC) or a similar rite of passage takes place at 97% of accredited allopathic medical schools and increasingly at osteopathic schools of medicine in the United States. 1
At the end of medical school, another rite of passage occurs as celebrated in the ritual of graduation when students are awarded the MD or DO degree. However, the one-day transformation from taking off the old white coat responsibilities of a medical student to wearing the new white coat responsibilities of a resident physician often gets lost, as residents travel to a new location and attend resident on-boarding sessions for the Graduate Medical Education (GME) Office, health-care system/hospital, and/or specialty-specific orientation programs. The resident is now someone's doctor whose obligations are “to place our patients’ welfare uppermost”, with “quality health care and patient safety” as primary objectives. 2 Yet, despite the fact that each resident often receives a white coat embroidered with his/her name/ specialty and is now addressed by patients and staff as “doctor,” we do little to mark this transition as these “new doctors” continue to develop their professional identity as a physician.
One hundred years after Funding Abraham Flexner's original report on medical education in the United States and Canada, the Carnegie Foundation again supported an extensive study of physician education entitled Educating Physicians. 3 This seminal work included residency education and highlighted the need for a focus on professional identity formation as a “necessary foundation for professionalism” among its four goals for medical education. 4 More recently, Cruess et al 5 have argued that professional identity will change as both society and health-care delivery systems evolve; therefore, the real objective of teaching professionalism is to support learners in developing their own physician identity, so that what they do as physicians emerges from “who they are.” The ACGME reemphasized the importance of professionalism as part of its Next Accreditation System in both the milestones 6 and the Clinical Learning Environment Review. 7
However, despite the power of the medical school WCC, a 2015 web search (keywords: resident, white coat ceremony, and transition to residency ceremony) revealed only 21 GME-focused WCCs. Six such ceremonies are at university-sponsored events (eg, George Washington University School of Medicine and Health Sciences, University of Texas Rio Grande Valley, and University of Buffalo) and 15 in community-based/health-care system-sponsored settings (eg, Ocala Regional Medical Center; Billings Clinic, Montana; and Texoma Medical Center). However, while these programs often presented the images of residents donning the white coat, they provided little to no description of the WCC's purpose or structure. A literature search revealed no explicit description of a WCC for residents, despite the long and evolving history of the WCC for medical students.
Recognizing this gap, in the United States, the Arnold P. Gold Foundation has begun piloting an oath creation and signing program as a formal residency event by having residents author an oath to strengthen their humanistic care of patients. 8 The oath signing is recommended to occur at a formal event in front of family and participating faculty with the oath then hung in a central hospital location and periodically revisited. While the Gold Foundation's work with residents is evolving with strategies for the resident writing groups, 9 a pilot phase for resident chapters, 10 and an expansion of the WCCs for nursing schools 11 and physician assistants, there is no mention of a WCC for residents within the Gold Foundation's materials.
To address this gap in the literature, this article describes a WCC for residents and provides resident/faculty perceptions regarding its value and critical elements to consider when implementing a WCC for a residency.
Methods
White coat ceremony
Aurora Health Care's Family Medicine Residency Program's annual WCC is designed to begin new residents’ acculturation to their entrusted roles as family physicians and professionals. Our objectives are to affirm for our new resident physicians and reaffirm for our current providers the privilege and joy associated with caring for our patients consistent with Family Medicine's core principles (eg, patient-centered continuity and coordination of care, teamwork, professionalism, quality, and safety). Held in late June, invitations are sent to current residents, faculty, staff, and hospital leaders in early spring along with a reminder to wear their white coats. All the residents and faculty are expected to attend.
The format and structure for the 90-minute WCC event is determined by the residency program leadership (Table 1). A senior clinical faculty member serves as a WCC moderator providing opening remarks highlighting the reason for the ceremony through a personal story as a family physician. The Program Director then welcomes the new residents with comments emphasizing the values that drew him or her to the specialty and how those values are revealed in our work, our training program, and our families. The Associate Program Directors then provide two brief histories to situate the event within the larger profession.
Structure of 90-minute residency WCC.

The first history provides a synoptic time-lapse overview of the white coat,12,13 highlighting physician's attire in Europe and North America through art. It begins with the white toga worn by Hippocrates and many consider him to be the first physician who considered medicine to be a science. 13 In the 17th century, the physician's role had become more formalized, as depicted in Rembrandt's The Anatomy Lesson of Dr. Nicolaes Tulp in 1631. Yet when juxtaposed with the images of a barber surgeon's white apron, the black hooded cloak, and wooden beaked mask worn by the physicians to (unsuccessfully) protect themselves from the plagues, the role of evidence-based medicine and physician servant are highlighted. Nineteenth century contrasting images highlight the formal black dress wear (Thomas Eakins’ 1875 painting, The Gross Clinic) with white uniforms and white laboratory coats (Dr. Agnew's Clinic, circa 1889) associated with scientific advances (eg, antiseptic surgical techniques and pharmacology). In summary, the historical review of the white coat is emphasized to our new residents that medicine has and will continue to evolve as a science and an art.
Then, the evolution of Family Medicine into a specialty is described using the American Board of Family Medicine's emblem as the narrative thread. 14 For example, the emblem's palm tree is a symbolic ability of Family Medicine to continuously rejuvenate itself–-beginning with its general practitioner horse and buggy roots to the decline of general practitioners in the mid-late 1900s to the establishment of Family Medicine as the 20th primary medical specialty in 1969 with required residency training. By highlighting the forces and people who influenced the specialty, with its continued emphasis on the core training elements established in 1969 15 (eg, first-contact care; continuous, comprehensive, family care; and competency in scientific general medicine), the WCC's history section encapsulates how the physician's role is an evolving interplay between societal needs and medicine as science and art.
The WCC concludes with three recognitions. New residency faculty members receive a Society of Teachers of Family Medicine (STFM) teaching lapel pin for their white coats. An honorary white coat is presented to a nonphysician department member who has demonstrated a commitment to the education of Family Medicine residents. New residents are individually recognized with an STFM pin, and their faculty advisor or a senior resident coats them to highlight continuity and transitions. Each resident then takes 60–90 seconds to briefly introduce himself or herself before the ceremony is closed.
Evaluation
We used two data sources to ascertain the value of the resident WCC: attendance at the WCC and a survey of attendees. Attendance data were tracked through WCC signatures in sheets. A brief, anonymous survey was distributed electronically following the 2015 Resident WCC to all FM faculty, staff, and residents and signed-in guests with two follow-up e-mail reminders.
The six-item survey comprised three demographic items (confirm attendance at the session, role in program, and prior WCC attendance), one five-point Likert scale item asking the participants to judge the importance of the ceremony as a transition event for our residency program, and two open-ended items: (1) what they valued about the event and (2) suggestions for improvement. Analysis of responses to the open-ended questions was done through the text analysis software by the first and last authors with themes reviewed and confirmed by all the authors.
Program leadership recommendations for how to start a residency-focused WCC
The WCC leaders (eg, program director, associate directors, senior faculty, and WCC coordinator) were debriefed by an experienced educational consultant (DS) to ascertain key elements in starting and sustaining a WCC. The consultant used open-ended questions regarding WCC structure and lessons learned. Results from the debriefing were synthesized and recirculated to all the participants, and the final results were framed as short- and long-term action items.
Results
WCC attendance and evaluation
We have held the resident WCC annually since 2009 on the last working day before the new residents are expected to begin clinical care. Our attendance has gradually increased over the years from <30 to 79 in 2014 and 97 in 2015. The continued increase reflects attendance by training program and clinical staff and hospital and health system's leaders (eg, President and CEO, Chief Medical Officer, and Chief Academic Officer).
A 60% (58/97) response rate was obtained with four of the respondents indicating that they had not attended the 2015 ceremony and were omitted from further analysis. In total, 41% of the respondents were residents, 24% Family Medicine faculty, 27% Family Medicine clinic staff, and 8% others (GME staff and academic/hospital leaders). For 14% of respondents, including the first-year residents, this was their first WCC, with 53% reporting attendance at two to three prior WCCs and 33% at more than three past WCCs. Seventy-nine percent of respondents (34/43) agreed that the WCC “is an important transition ceremony for our residency program”: 100% of clinic/academic staff, 73% of residents, and 67% of faculty.
Responses to the open-ended items focused on the WCC's value, highlighting the ceremony's role in marking the transition of new residents to the specialty. Figure 1 provides a graphic depiction of the 35 most commonly used terms in respondents’ answers, with word size increasing as word frequency increases.
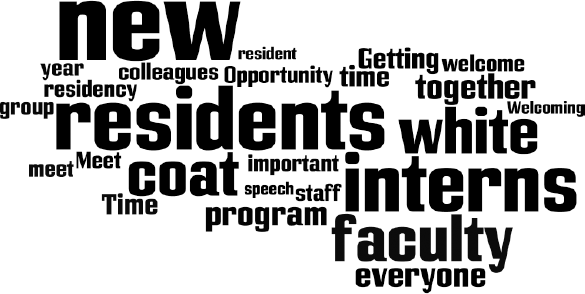
Value of resident WCC–-text analysis frequency up to 35 words for all respondents. Word size increases as word frequency increases (eg, the more frequently the word is mentioned, the larger the word text).
Residents valued the WCC as an “opportunity to recognize the incoming residents’ passage into doctor hood,” “welcoming the new residents into their chosen profession,” and “opportunity to welcome new physicians into our family”; a “reminder of our collective history as family physicians”; and the symbolic nature of the ceremony through the “Presentation of the STFM Pin.” Residents also emphasized the importance of “show(ing) the new residents they are important and we are excited to have them,” “making new colleagues feel valued,” and the opportunity to “emphasize that we all have worked hard … (to be) proud to get to where we are and honor that.”
Faculty responses affirmed the value as a transition event but had an expanded view of the WCC's value to the training program. Typical responses included “enhancing sense of purpose and community,” “ability to drive culture,” and “building an esprit de corps.” Faculty responses highlight an added WCC value as a time for renewal/reaffirmation on their physician role. Example responses included “reaffirming my career choice,” “a sense of community and time for reflection on the careers we lead,” and the “… privilege to wear the white coat as an MD.”
Respondents recommended that the WCCs continue to evolve given the number of repeat attendees. Suggestions included providing an opportunity for discussion (eg, white coat as symbol or barrier for Family Medicine) and logistics (timing and invitation to friends/family).
Recommendations to programs considering a WCC
The WCC leaders, the residency program director, and two associate program directors have identified key short-term and long-term action steps associated with starting a residency-focused WCC (see Table 2). The action steps needed are common to any residency education initiative in that it takes leaders and champions, advance planning (eg, resident/ faculty/clinic schedules, facilities, and budget for white coats), and ongoing internal and external communication regarding the importance of marking transition events for current and new residents/faculty/staff. Similarly, the inability to galvanize support/resources may indicate the need to reframe the proposed plan.
Recommendations for how to start a residency-focused WCC.

Conclusions
The residency WCC formally marks the transition from medical student to that of the physician, who assumes ever-increasing responsibility for the unsupervised care of patients. Initially designed to support new residents’ professional identity development by highlighting the history, ideals, and values of their chosen specialty, the WCC also served to reaffirm our faculty physicians’ specialty choice, which was consistent with Cruess et al's observation that professional identities evolve with changes in societal expectations, health care, and delivery systems. 5
The WCC elements change to reflect the evolving role of family physicians and the residency program. Future study is needed to determine the effects of the WCC, as part of a longitudinal residency curriculum, on residents’ and faculty physicians’ professional identity development.
Author Contributions
Conceived and designed the experiments: JLB, MWR, CG, and ES. Analyzed the data: DS and JLB. Wrote the first draft of the manuscript: JLB and DS. Contributed to the writing of the manuscript: JLB, MWR, CG, ES, and DS. Agreed with the manuscript results and conclusions: JLB, MWR, CG, ES, and DS. Jointly developed the structure and arguments for the paper: JLB, MWR, CG, ES, and DS. Made critical revisions and approved the final version: JLB, MWR, CG, ES, and DS. Reviewed and approved the final manuscript. JLB, MWR, CG, ES, and DS.