
Abstract
Objective
A growing body of literature seeks to understand how best to support students in their Professional Identity Formation (PIF) during medical school. Recent work has suggested the need for a longitudinal approach that supports development of and recognizes variation in professional identity (PI) reflecting individual differences in perspectives and goals. We sought to evaluate a longitudinal, formal PIF curriculum at our medical school through a qualitative analysis of learner perspectives.
Methods
We invited third- and fourth-year medical students likely to have strong opinions on the PIF curriculum to participate in semi-structured interviews, aiming to capture diverse opinions and outliers to better understand its impact. Twenty students were invited to participate, and 15 students consented to participate. We took an inductive thematic approach to data analysis. The first three transcripts were read by coders before the coding process began. Readers then reread the transcripts and independently generated initial codes and then met to develop a consensus on codes and coding framework. The agreed-upon framework was then used to code the subsequent transcripts.
Results
Our student interviews revealed a range of perspectives on the PIF curriculum as well as their PI. Five major themes within the data were identified, reflecting the developmental process of identity formation, the challenges and tensions that inform that development, and the impact of the curriculum on the learners’ identity development. These themes are 1) deciphering the curriculum and curricular concepts, 2) grappling with the concept of PIF, 3) actively crafting an identity, 4) challenges to engaging with PIF curriculum, and 5) strengthening the curriculum.
Conclusions and practice implications
The development of a PI in budding physicians is complex, and students appreciate the ability to explicitly reflect on and shape their identity, while receiving support and feedback about the process from educators. A formal PIF curriculum that supports students in actively creating their PI provides them with a better understanding of the challenges involved and the scaffolding needed to develop a mature PI that aligns with both professional and personal values.
Keywords
Highlights
Entering medical students have a vague sense of professional identity (PI).
Initial questions about joining the profession felt foreign but spurred reflection.
A formal longitudinal PIF curriculum provides a necessary framework for students to develop their PI.
Educators can support PIF by providing opportunities for reflection yet space for individualized pathways to unique PIs that fit with students’ personal identities.
Introduction
Medical educators are increasingly focused on supporting medical students’ (MS) professional identity formation (PIF). 1 A variety of approaches have been suggested, and several have been studied for their impact on PIF;2,3 however, there is a lack of studies that use qualitative methods to elicit a more in depth understanding of student perspectives on such strategies. A more recent reconceptualization of PIF that acknowledges the needs of a disparate range of learners in an everchanging world has highlighted the need for educators to consider PIF strategies that attend to the “diverse ways of being, becoming, and belonging within the profession.” 4 As such, the exploration of MS perspectives regarding their experience of curricula developed to support their PIF can further advance effective PIF strategies that will meet the needs of our evolving profession.
Our understanding of PIF and its theoretical underpinnings has evolved over the last decade, which has implications for the development of PIF-related curricula. Montrouxe and Rees categorized strategies to support PIF as falling into two broad theoretical domains: individualistic and social-contextual. 5 Individualistic identity development is dependent on one's internal, psychological processes of building identity, while social-contextual development accounts for how social interactions, group processes, and contextual factors help shape PIF. Two recent reviews5,6 found curricula predominately based their interventions on more individualistic approaches, such as written reflections. Additionally, many interventions used activities related to ethics, medical humanities, and doctor-patient communication skills training to promote professional development without an explicit focus on PIF. Yet both reviews highlight the need for more formal curricula that addresses both the individual and social context (including the hidden curriculum) contributing to PIF.
More recently, there has been recognition of the multiple pathways individuals may take as they seek to integrate their professional identity (PI) into their preexisting individual identity. There is no one “professional identity”; each person's lived experiences and values will uniquely shape how professional expectations, standards, and values are folded into a coherent identity.1,4 Sternszus et al 4 noted the importance of explicit discussions of how professional norms and values fit or conflict with both one's individual values as well as the demands of the social context. In order to do this, learners must reflect on their experiences and reactions, critically engage with professional context and norms, and recognize their own agency to actively and continuously build their PI.
We sought to contribute to the growing understanding of PIF and how best to support it by evaluating our longitudinal PI curriculum through the eyes of senior MSs who had completed the curriculum, using a qualitative approach. This longitudinal curriculum, starting from the beginning of medical school, is composed of educational activities and reflective practice designed to provide a language and scaffolding to help students make sense of their experiences and consider how they can make choices to actively shape their PIF. Our curriculum utilized a mixed model of PIF development (individual, social-contextual, including an awareness of professional and personal context) as described above.
Professional Identity Formation Curriculum
The longitudinal PIF curriculum, begun in 2007, has adapted over time as a more complex and multifaceted understanding of PIF became apparent. We sought to more broadly address the social context and the shifting societal, medical and educational landscapes, and consider how learners with different life experiences may choose to define their own PI as they integrate medicine's values into their own existing sense of self. The goals of the PIF Curriculum are to: (1) explicitly focus on the developmental nature of PIF, (2) explore challenges of integrating personal and professional identities and support students in assuming the responsibility to craft their own PI throughout their careers, and (3) provide a scaffolding and language, as well as the opportunity to discuss and understand professional values and behaviors.
The curriculum includes five workshops (90 min - 2 h) held over 4 years (Table 1), paired with writing Professional Identity Essays (PIEs) and reflecting on written developmental feedback about their writings (see Appendices A and B). Objectives include learning the language and framework of PIF, articulating the nature of medical professionalism, medicine's social contract, the values we hold as physicians, and describing the process of PIF and socialization. Students discuss barriers to professional behavior, including the “hidden curriculum,” ethical challenges they experience during their training, and reflect on their PI essay report with support from faculty. All workshops use active learning strategies paired with reflection and include facilitation by faculty and/or senior MSs. Recognizing that PIF is impacted by many other experiences beyond these formal sessions, most notably through clinical learning and role modeling that occur during clinical rotations, additional PIF support is thus integrated throughout the medical school curricula (Table 1). Students are encouraged to be active curators of their own PI, allowing for individualized pathways based on their own values and lived experiences, rather than a “one size fits all” prescriptive PIF.
Professional Identity Formation Curricular Activities.
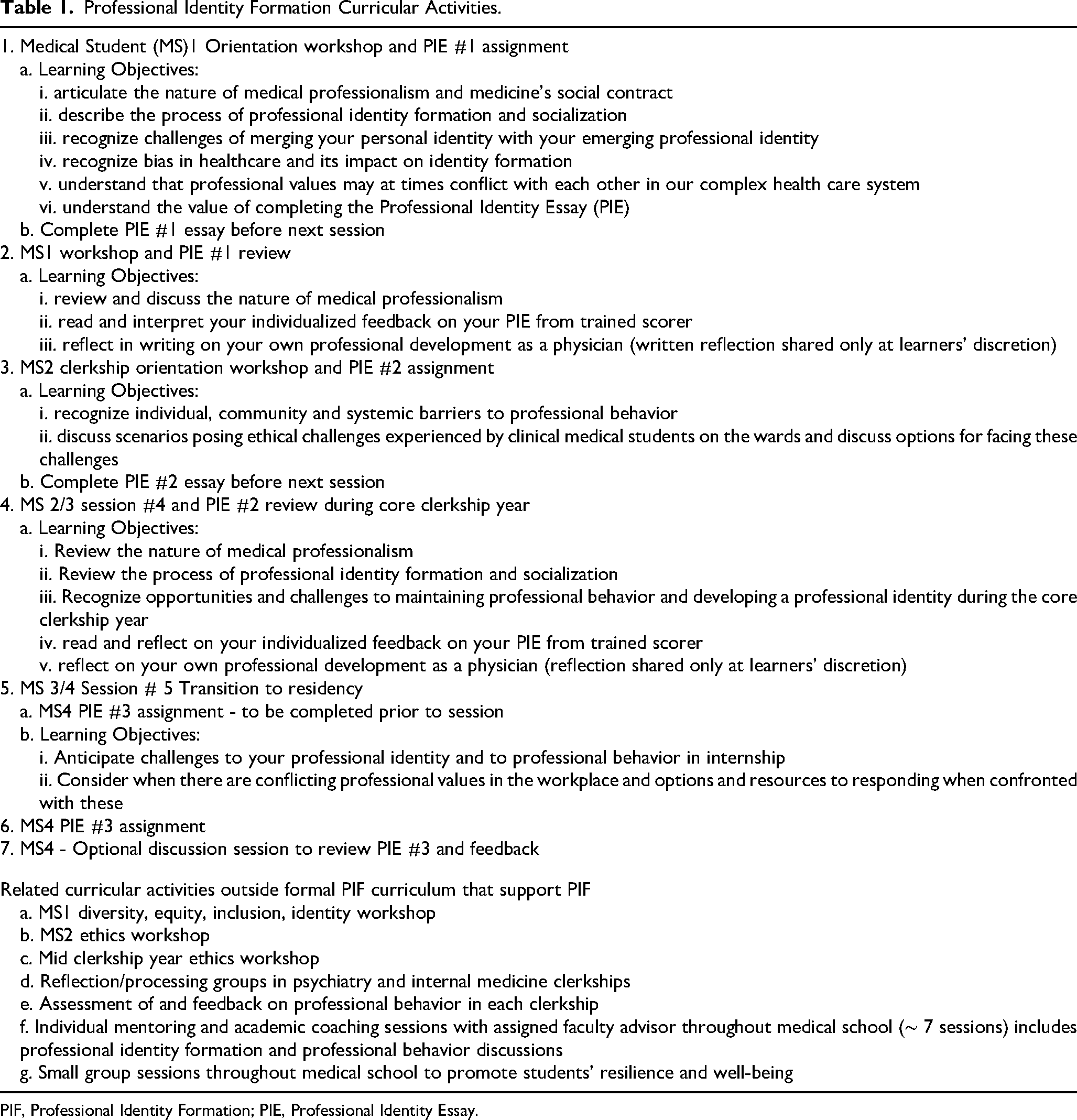
PIF, Professional Identity Formation; PIE, Professional Identity Essay.
Professional Identity Essays
The PIE completed by our students, developed by Bebeau and Monson, is an adaptation of Kegan's Adult Developmental Model to focus on PI 7 and tailored to medical education. 8 This model describes development as a process of transforming to more complex ways of knowing and of making sense of the world. The essays, including nine prompts eliciting conceptions of the professional role (Appendix A), are evaluated by expert raters (who have no contact with students) who generate a stage score and an individualized report, highlighting the reasons for the assigned stage and ideas for reflection that are designed to broaden students’ reflections on ideas or situations. The stages, as set forth by Bebeau and Monson 7 based on Kegan's model, are described in Appendix B.
Explanations about the purpose of PIEs, and implementation processes (length and depth of responses expected, no “right answers”, what scoring means, feedback they will receive, privacy) are described at the first PIF workshop, and students are given 2-3 weeks to complete PIE assignments at a time convenient to them. They then receive written feedback including a description of their developmental stage, highlighting their strengths and including questions to consider that may prompt more complex consideration of PI issues. After a group debrief with trained faculty during a workshop, students write a confidential reflection on the report to cultivate insight on their PIF. In order to provide psychological safety in this reflection exercise, the essays, feedback, and their reflections are private, and only shared if, and when, the student chooses to do so. These essays are administered three times over the course of medical school: at the beginning, prior to beginning clinical rotations, and in the final year.
Statement of Purpose
We sought to evaluate the longitudinal PIF curriculum at our medical school. Using an inductive thematic qualitative method, we explored how MSs at an academic medical center experienced the PIF Curriculum.
Methods
The Institutional Review Board approved and deemed this work a quality improvement study (see attached documentation). In accordance with COPE guidelines, we are obtaining retrospective written informed consent for publication from all participants. Confirmatory documentation will be provided to the editors as required.
We invited third- and fourth-year students to participate in semi-structured interviews. These students had experienced the longitudinal curriculum and were well placed to reflect on its impact. Students were interviewed between 2022 and 2024. Initially, faculty mentors suggested students who had expressed positive or negative opinions about the curriculum and then snowball sampling was used by asking those students to suggest peers who may also have had strong opinions. We used this purposive sampling approach to gather a range of opinions, including outliers, to deepen our understanding. An effort was made to ensure the inclusion of a range of students representing diverse backgrounds and experiences. This included self-identified race, self-identified gender, and MS Year. Subjects were excluded if they did not meet inclusion criteria; otherwise, there were no exclusion criteria.
Email invitations to participate in the study were sent to the identified students. Those who responded were asked for verbal consent at the beginning of the interviews. After consent was obtained, two researchers not involved in implementing the curriculum (LA & EW) conducted interviews via ZoomTM which, with permission, were recorded, stored on a secure server and professionally transcribed. Interviews ran approximately 30 min. Interviews were stopped after 15 interviews were completed as data saturation was reached.
The interview guide was developed by LA, who has expertise in program evaluation, survey design and qualitative methods, with input from the remaining authors. This guide was reviewed and edited by the remaining authors and by the PIF Curriculum Faculty. See Appendix C for Semi-Structured Interview Guide. All de-identified interview transcripts were uploaded into DedooseTM software. Analysis of the data utilized an inductive thematic analysis completed by three readers (L.A., L.T, and E.W.). 9
After familiarizing ourselves with the transcripts before the coding process began, readers independently generated initial codes for the first three transcripts. We then met to develop a consensus on codes and coding framework. The agreed-upon framework was then used to code subsequent transcripts. The group met regularly to review coding, make modifications, and add new codes as needed. After initial coding, L.B-K reviewed the codes and contributed to the discussion of themes. Once all transcripts were coded, emergent themes were discussed and adapted as appropriate by the team, including AK until consensual validation was reached. An audit trail and multiple coders helped ensure analytical rigor.
Reflective practice and discussions of issues of positionality occurred throughout these meetings, and we explored how each member's biases may influence interpretation of the data. LA and EW are medical education researchers with extensive training in PIE scoring. LA is a developmental psychologist, and EW is pursuing an advanced practice nursing degree. LT (pediatrician) and LBK (internist) have previously been Associate Dean of Student Affairs. LBK is Director of the Professional Identity Curriculum. AK (internist) is a medical educator with a strong research background and leadership experience at the UME and GME level. All authors are white cisgendered females.
The reporting of this study conforms to the Standards for Reporting Qualitative Research statement 10 (see Supplementary File 1).
Results
Twenty students were invited to participate, and 15 students consented to participate. Table 2 describes the student participants.
Student Participants.

MS, medical student.
We identified five major themes within the data, reflecting the developmental process of identity formation, the challenges and tensions that inform that development, and the impact of the curriculum on the learners’ identity development. These themes are 1) deciphering the curriculum and curricular concepts, 2) grappling with the concept of PIF, 3) actively crafting an identity, 4) challenges to engaging with PIF curriculum, and 5) strengthening the curriculum. See Table 3 for exemplary quotes.
Exemplary Quotes from Interviews.
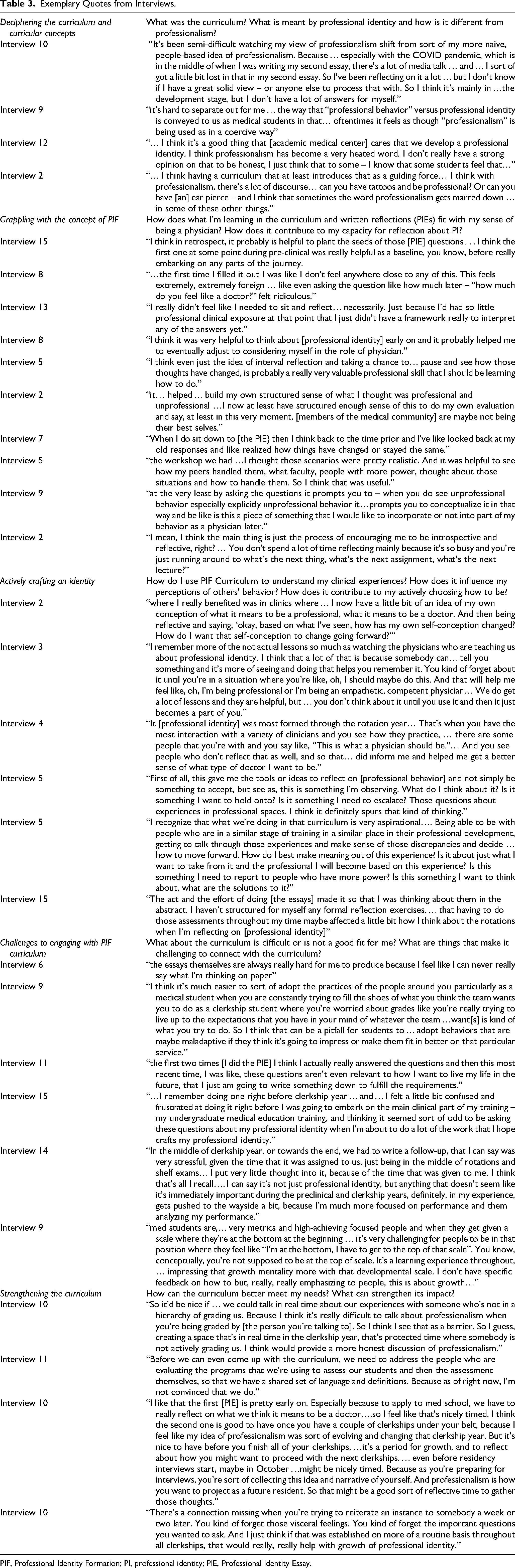
PIF, Professional Identity Formation; PI, professional identity; PIE, Professional Identity Essay.
Deciphering the Curriculum and Curricular Concepts
When asked to describe what participants understood as the PIF curriculum, most expressed some degree of uncertainty. While many noted specific PIF workshops and PIE essays respondents also described structured and unstructured discussions, reflective exercises and experiential learning that, while contributing to PI, were formally part of other curricula (eg, ethics lectures, doctoring courses). One interviewee said “I’m not really sure… I’m sometimes unaware [of] which curriculum I’m currently sitting in or doing” (Interview 12). While this may indicate a lack of clarity in messaging about the PIF curriculum, it also reflects the reality that PIF is a complex phenomenon and is (and should be) developed and reinforced across all aspects of the medical school curriculum.
Faculty teaching within the PIF curriculum attempted to clarify the distinction between PI and professionalism; however, this distinction was not clear to some students. During PIF workshops, PIF was presented as an individual, active growth process of crafting “what kind of doctor you choose to become” while professionalism involved standards for professional behavior. However, when asked about PI, some students referenced lectures by other faculty that focused on standards for behavior. Respondents’ uncertainty about the terms “professionalism” and “professional identity” was apparent in the student comment: “it's hard to separate out for me I think the idea of or at least the way that ‘professional behavior’ versus ‘professional identity’ is conveyed to us as medical students in that… oftentimes it feels as though ‘professionalism’ is being used as in a coercive way” (Interview 9). Nonetheless, unearthing this perplexity helped prepare students for learning about and developing their PI.
Grappling with the Concept of PIF
Upon entering medical school, students had a vague sense of PI and found the topic confusing to consider. One student noted, “The first time I filled it out [the PIE] …this feels extremely, extremely foreign … like even asking the question …‘how much do you feel like a doctor’ felt ridiculous.” (Interview 8). Discussions during early PIF sessions and writing about what being a physician meant to them seemed to be purely theoretical and not grounded in experience, yet served as seeds that grew over time.
The value of planting seeds about PIF early on in medical school became apparent to students over time, and in fact, gave them a language to identify the process of PI development and empowered them to act. They recognized that the questions posed during the early sessions and in the PIE allowed them to deepen their understanding of what it means to be a part of the profession. “I think in retrospect, it probably is helpful to plant the seeds of those [PIE] questions . . . I think the first one at some point during pre-clinical was really helpful as a baseline, you know, before really embarking on any parts of the journey (Interview 15). And, “I don’t think I would have had the …conscious level… that I was like ‘oh I’m starting to think of myself more as a physician’ if I hadn’t been primed with the question. It was helpful to think about [professional identity] early on and helped me to adjust to considering myself in the role of physician” (Interview 8).
As they progressed through their training, the curriculum, and writing PIE essays, students came to more clearly appreciate their growth. Many respondents noted changes in their perspectives in their responses to the essays over time. “When I would write the next one, I would look back at what I’d said before, and I was surprised that things changed” (Interview 5).
Opportunities for reflection individually, with peers, and with faculty fertilized the seeds of PIF planted during early sessions, allowing them to flourish. “Having space for a discussion about professional identity has been really important … it's not something that I have necessarily actively thinking about on my own” (Interview 6). Sharing information and skills during workshops were also highlighted. For example, role-playing responses to unprofessional behaviors, 11 were noted to be “pretty realistic” and “helpful to see how my peers handled them, what faculty, people with more power, thought about those situations and how to handle them” (Interview 5). And, “[the school] doesn’t want this to happen yet it also recognizes that sometimes it does happen and that students need to recognize when it's happening and be able to discuss with someone that it's happening or their own reactions to it” (Interview 15).
Actively Crafting an Identity
As students progressed into their clinical years and took on the professional role, they experienced exceptional growth in their PI using earlier discussions and reflections about PIF to actively craft their PI in the clinical realm. Students observed a wide range of physician behaviors and skills and formed relationships with near-peers and attendings. Exposure to physicians in practice allowed them to reflect on values they would like to assume, and behaviors they would choose to emulate. Active discussion of values and expectations within the PIF curriculum before entering the clinical environment allowed learners to consider how professional and personal values and expectations fit (or not) together and to actively choose their values. This theme was highlighted in all of our interviews. Students actively craft their identities by observing others, practicing being in the role with all its attendant pressures and making choices about how to adopt, adapt or reject the behaviors they see in role models.
As one student noted, “where I really benefited was in clinics where … I now have …an idea of my own conception of what it means …to be a doctor. And then [reflecting on] ‘ based on what I’ve seen, how has my own self-conception changed? How do I want that self-conception to change going forward?’” (Interview 2).
The framing of PIF through the curriculum also provided a lens to negotiate responding to other professionals’ behaviors: “this gave me the tools … to reflect on …something I’m observing. What do I think about it? Is it something I want to hold onto? Is it something I need to escalate? Those questions about experiences in professional spaces, it definitely spurs that kind of thinking” (Interview 5).
Challenges to Engaging with PIF Curriculum
Students identified challenges as they tried to make sense of both the PIF curriculum and their own developmental journey and to integrate that development into the broader medical school experience. They noted time pressures that made attending to and completing the PIE reflective writing tasks difficult given the competing demands of higher stakes assignments. “It's not just professional identity, but anything … gets pushed to the wayside a bit, because I’m much more focused on performance and them [faculty] analyzing my performance” (Interview 14).
Students noted the tension inherent in needing to “perform” in different clinical settings and adopt behaviors that may conflict with their aspirations. “I think it's much easier to adopt the practices of the people around you particularly as a medical student when you are constantly trying to fill the shoes of what you think the team wants you to do as a clerkship student where you’re worried about grades … that can be a pitfall for students to adopt behaviors that are maybe maladaptive if they think it's going to impress or make them fit in better on that particular service” (Interview 9).
Additionally, awareness of being continually evaluated by others influenced students’ reactions to developmental feedback on PIE essays. Although students were regularly reassured that they were early in their lifelong PI journey, students experienced discomfort at not being at the top developmental level. Interestingly, few students described this as their own experience, but many presented this as the experience of their peers. For example, one student states that “it's challenging for people to be in that position where they feel like ‘oh no I’m at the bottom, I have to get to the top of that scale.’ … but really emphasizing to people this is about growth, you’re at the bottom and that is appropriate and–at medical school you’re not going to be at the top necessarily and that's appropriate as well” (Interview 9).
There was tension over how often to have structured reflection on PIF and who should lead these discussions, with psychological safety concerns. A few respondents felt that discussions about PIF were most relevant once they were in clinical settings, although most acknowledged that early discussions helped them consider their experiences in light of those earlier discussions. Regarding frequency, one student commented, “The first two times I actually really answered the questions and then this most recent time, I was like, these questions aren’t even relevant to how I want to live my life in the future, I just am going to write something down to fulfill the requirements” (Interview 11).
Finally, for a few learners, written reflections about PIF were not seen as helpful. One student commented, “the essays themselves are always really hard for me to produce because I feel like I can never really say what I’m thinking on paper” (Interview 6).
Strengthening the Curriculum
Students expressed the desire for more opportunities for reflection and more integration of such reflections into their ongoing learning and experiences.
There was a desire for a clearer understanding of PI as distinct from professionalism and a clarification of how both of those concepts are assessed. “Before we can come up with the curriculum, we need to address the people who are evaluating the programs that we’re using to assess our students and then the assessment themselves, so that we have a shared set of language and definitions”(Interview 11). Some students noted that at times there was a discrepancy between the values espoused in the curriculum and what they observed in practice. “There are plenty of behaviors that… don’t square particularly well with the professional identity curriculum… that we’re being given” (Interview 9). Finally, the uncertainty that students experienced as they tried to make sense of the complexity of PIF was reflected in their desire for clear “right answers” as they moved through their development. “Students are very used to… you answer a question then there is … if not a right answer, there's at least a way you should be thinking” (Interview 4).
Students’ views differed on the appropriate discussion guides based on their own sense of psychological safety. Some students were hesitant about engaging in open and honest discussions with faculty who were in positions to evaluate them. “It’d be nice if … we could talk … about our experiences with someone who's not in a hierarchy of grading us. Because it's really difficult to talk about professionalism when you’re being graded by an advisor, and the dean and all of your attendings” (Interview 10). Others felt that having PIF discussions integrated into their clinical rotations would allow them to process their thoughts and feelings about experiences in real time, and with faculty who were familiar with specific situations and with the learners’ strengths and challenges. “There's a connection missing when you’re trying to reiterate an instance to somebody a week or two later. You forget those visceral feelings. … And I think if that was established on a routine basis throughout all clerkships, that would really help with growth of professional identity.”
Finally, in spite of the challenges of making sense of this complex issue, students appreciated that the school highlighted the importance of PIF. As one student noted, “I think it's a good thing that [the school] cares that we develop a professional identity” (Interview 12). And they recognized that the uncertainty experienced during their journey may be part of the process. “I was kind of surprised in the whole process at how it naturally comes about, and I was very skeptical just getting the tools and skills pre-clinical. But it is helpful to be introduced to these things, forget about it, and then once you’re in a situation … it's helpful to have a toolkit so you can pull things out when you need and when you think it's appropriate. That was the major surprise to me in how successful that actually was, because I was very skeptical at first” (Interview 3).
Discussion and Conclusion
Discussion
Our evaluation of a longitudinal PIF curriculum revealed that students experienced identity formation as gradual, multifaceted, and shaped by structured opportunities for reflection. Participants described initial uncertainty about PI, followed by growing clarity as they engaged with workshops, PIEs, and dialogue. These activities “planted seeds” early in training that later grew into deliberate efforts to craft identity during clinical rotations. Students valued the curriculum for directly discussing these issues and for providing language and tools to interpret their experiences, though they also noted challenges such as competing demands, lack of clarity between professionalism and PI, and discomfort with reflective writing. Learners emphasized the need for more frequent, integrated reflection and the importance of psychological safety and non-evaluative faculty support.
By purposely seeking out students with strong reactions to our PIF curriculum, both positive and negative, we obtained a wide range of viewpoints. These findings highlight PIF as a dynamic developmental process in which learners integrate medicine's values into an authentic sense of self. Identity is not passively acquired but actively curated through reflection, critical evaluation, and selective integration of observed behaviors. By positioning students as agents in their own identity development, educators can foster deeper engagement and more adaptive trajectories.4,11
The curriculum's structured activities supported this process by scaffolding reflection across training. Developmental and transformative learning theories suggest that repeated cycles of reflection and application, supported by open discussion and guided questioning, promote more complex and integrated ways of making sense of the professional role.12,13 Participants particularly valued direct, honest conversations that helped them reconcile personal values with professional expectations and identify strategies to enact their role with integrity. Faculty-led dialogue and modeled reflective practice signaled that identity work is legitimate, further normalizing this as a central aspect of medical education. Further work is necessary to expand the capacity of more clinical faculty to directly support and model such practice during clinical rotations. One challenge to this is the dual role of clinical faculty in both evaluating students and supporting them by creating the psychological safety necessary for self-disclosure and reflection.
Unsurprisingly, the students’ PIF accelerated during their clinical rotations where patient care experiences and the opportunity to observe those further along in their medical training provided students the opportunity to visualize their future professional role. This is consistent with the literature 14 and points to the importance of embedding reflection within clinical contexts. Real-time reflection with trusted faculty makes identity work more relevant, bridging abstract discussion with patient care experiences and reinforcing the notion that PI is both contextually grounded and personally owned. Such integration may also reduce the sense that reflection is an added task competing with high-stakes evaluations.
While students learn the language and framework of PIF, clinical supervisors are not necessarily reinforcing the PIF curriculum. Faculty and housestaff development in this domain would likely enhance the clinical learning environment. 15 Although learners noted tensions such as the hidden curriculum, they described how the curriculum gave them tools to address these challenges constructively. They valued learning strategies to address professional challenges (eg, how to respond to unprofessional behavior of others, where/ how to seek support, how to report such behaviors). Brown et al note 16 the negative impact role modeling, stereotyping and organizational culture (ie, the “hidden curriculum”) can have on students’ PI and giving students tools to mitigate those impacts is essential to PIF. Explicit permission and support to question observed norms fostered professional agency and reframed PIF as not merely adapting to culture but shaping a better future for the profession. This shift from defensive resistance to generative contribution underscores the growth potential of well-designed PIF curricula.
Limitations
Despite a purposeful sampling strategy, input from students with minoritized identities was relatively limited. This includes individuals with prior personal and professional experiences that may challenge professional norms in unique ways. Faculty could also be viewed as gatekeepers of participants as they were asked to identify initial students for this study. Finally, our purposive sampling strategy, designed to obtain the full range of perceptions about the curriculum, may have excluded quieter students with other views. Future research is needed to further expand our understanding of the PIF process to support inclusion of the widest range of experience possible. Of course, the generalizability of our findings is limited because this study reflects the experience of students at one medical school with a curriculum that developed locally over a 16-year period.
Conclusions and Practice Implications
In sum, our results support moving beyond professionalism as a prescriptive list of behaviors to actively engage learners in the challenges of creating their own unique PI that can align with the aspirational goals of the profession. A formal PIF curriculum that creates intentional, psychologically safe spaces where learners can reflect, question, and integrate their personal values with those of the profession, provides the necessary scaffolding to develop a mature PI that we hope can serve them as they move through their career.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261427163 - Supplemental material for Growing Professionals: Exploring the Impact of a Professional Identity Formation Curriculum in Medical School
Supplemental material, sj-docx-1-mde-10.1177_23821205261427163 for Growing Professionals: Exploring the Impact of a Professional Identity Formation Curriculum in Medical School by Lisa Altshuler, Linda Tewksbury, Lynn Buckvar-Keltz, Elizabeth Wargo and Adina Kalet in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205261427163 - Supplemental material for Growing Professionals: Exploring the Impact of a Professional Identity Formation Curriculum in Medical School
Supplemental material, sj-docx-2-mde-10.1177_23821205261427163 for Growing Professionals: Exploring the Impact of a Professional Identity Formation Curriculum in Medical School by Lisa Altshuler, Linda Tewksbury, Lynn Buckvar-Keltz, Elizabeth Wargo and Adina Kalet in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
We would like to acknowledge Verna Monson for sharing her expertise on PIEs and the time spent dedicated to score the PIEs. Additionally, we want to acknowledge the PIF Curriculum Committee at NYU for supporting the curriculum work and the thoughts that led to the development of this paper. We thank the students that agreed to be interviewed and the insights shared. Lastly, we want to thank Sondra Zabar for her wisdom and just being Sandy.
Ethical Considerations
This study was deemed exempt by the NYU Langone Health Institutional Review Board (IRB) as a quality improvement initiative.
Consent to Participate
All participants provided consent prior to participating.
Consent for Publication
In accordance with COPE guidelines, we are obtaining retrospective written informed consent for publication from all participants. Confirmatory documentation will be provided to the editors as required.
CRediT Authorship Contribution Statement
Lisa Altshuler: Conceptualization, Methodology, Investigation, Formal analysis, Writing - Original Draft, Visualization. Linda Tewksbury: Formal analysis, Writing - Original Draft, Visualization. Lynn Buckvar-Keltz: Conceptualization, Methodology, Investigation, Formal analysis, Writing - Original Draft. Elizabeth Wargo: Project administration, Investigation, Formal analysis, Writing - Original Draft. Adina Kalet: Conceptualization, Writing - Review & Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by the Kern Family Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendices
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.