
Abstract
We examined the prevalence of specific perinatal complications of monochorionic-diamniotic twin pregnancies in cases without any abnormal findings until the second trimester of pregnancy. This was a retrospective cohort study performed at a tertiary perinatal center in Tokyo, Japan. There were 88 cases of uncomplicated monochorionic-diamniotic twin pregnancies at 28 weeks of gestation. In five of them (5.7%), there were serious complications associated with placental circulatory imbalance between the twins during the third trimester of pregnancy. Two cases were complicated by twin–twin transfusion syndrome, two cases were complicated by twin anemia–polycythemia sequence, and one case was complicated by acute twin–twin transfusion syndrome. In the five cases, no abnormal ultrasonographic findings or symptoms were recognized one or two weeks prior to the diagnosis. Fifty-eight cases (65.9%) were delivered at term uneventfully. Serious complications due to placental circulatory imbalance between twins occurred in about 6% of cases during the third trimester of pregnancy.
Keywords
Introduction
Some specific complications in monochorionic-diamniotic (MD) twin pregnancies such as twin–twin transfusion syndrome (TTTS) are the result of unbalanced blood flow through placental anastomoses between twins. TTTS occurs at a frequency of 8%–15% in monochorionic twin pregnancies, and the majority of these cases are diagnosed during the second trimester.1–7 However, twin anemia–polycythemia sequence (TAPS) is a rare form of TTTS, which is characterized by the presence of a large intertwin hemoglobin difference without signs of twin oligo-polyhydramnios sequence.8–10 Lewi et al 10 observed that TAPS was diagnosed in more than one-third of pregnancies with late-onset discordant fetal growth. In addition, acute TTTS, which is the shift of blood from one twin to the other, is thought to result from blood pressure differences due to uterine contractions or changes in fetal positions.10–12 Therefore, it is thought that various specific complications associated with unbalanced blood flow in the placenta are mixed during the third trimester of MD twin pregnancies.
In this study, we examined the prevalence of these specific perinatal complications of MD twin pregnancies in cases without any abnormal findings until the second trimester of pregnancy.
Methods
This is a retrospective study of the medical databases of our institute. The protocol for this analysis was approved by the Ethics Committee of the Japanese Red Cross Katsushika Maternity Hospital. In addition, informed consent for analysis from a retrospective database was obtained from each subject during their hospital visit.
In order to extract cases without any complications until the second trimester of pregnancy, we excluded the following cases: (1) those with single or double fetal demise before 28 weeks of gestation, (2) fetuses with major anomalies, (3) amniotic fluid (AF) discordance in one or both twins before 28 weeks of gestation, (4) fetal growth discordance ≥25%, or (5) fetal growth restriction in one or both twins before 28 weeks of gestation.
In our follow-up protocol for uncomplicated monochorionic twin pregnancies after 28 weeks of gestation, we measured the fetal weight, AF volume, and umbilical artery waveforms by ultrasonography every one or two weeks. During this period, we did not routinely perform the measurement of middle cerebral artery waveforms. During this period, we had a policy of elective delivery before 38 weeks of gestation for MD twins to prevent unexpected intrauterine fetal death in MD twins at term. 13 Even in uncomplicated MD twin pregnancies, elective cesarean section can be performed based on informed consent. 14
Between 2011 and 2014, there were 118 cases of MD twin pregnancies managed at our hospital beyond 28 weeks of gestation. Of these, 30 cases (25.4%) met these exclusion criteria. Thus, we examined the remaining 88 cases (74.6%) as uncomplicated MD twin pregnancies at 28 weeks of gestation.
In this study, the diagnosis of TTTS was based on the presence of polyhydramnios (vertical AF pocket greater than 8 cm) in one sac and oligohydramnios (vertical pocket less than 2 cm)/anhydramnios in the other sac.1–7 The diagnosis of TAPS was based on the presence of chronic anemia with reticulocytosis (as a sign of chronic anemia: reticulocyte count greater than 7%) in the donor twin and polycythemia in the recipient, while the diagnosis of acute TTTS was based on the presence of acute anemia without reticulocytosis in the donor twin and polycythemia in the recipient.8–10
At delivery, in addition, small for gestational age is defined as a weight below the 10th percentile for the gestational age in Japanese. 15
Results
There were 88 cases of uncomplicated MD twin pregnancies at 28 weeks of gestation.
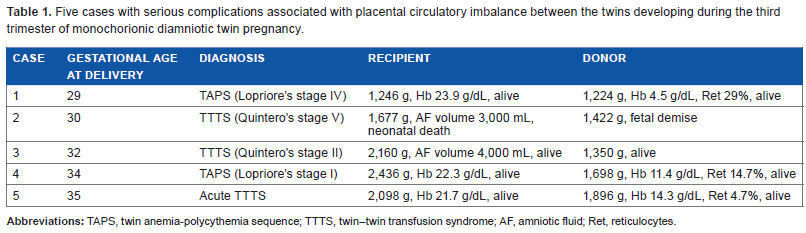
In five of them (5.7%), however, there were serious complications associated with placental circulatory imbalance between the twins during the third trimester of pregnancy, as shown in Table 1. In these five cases, no abnormalities were recognized one or two weeks prior to the diagnosis. The two women complicated by TTTS (Cases 2 and 3) exhibited increased abdominal distension during the week prior to the diagnosis. The living fetus in Case 2 showed early neonatal death due to heart failure. In Case 5 (acute TTTS), the patient was admitted to the emergency department because of the feeling of decreased fetal movements from a few hours before the diagnosis. An emergency cesarean delivery was performed due to a nonreassuring fetal status of both the twins using a cardiotocogram. In Cases 1 and 4, the cardiotocogram showed a reassuring fetal status in both twins. However, immediate cesarean deliveries were performed due to abnormal ultrasonographic findings: fetal growth arrest in the donor twin in Case 1 and the accumulation of pericardial fluid in the recipient twin in Case 4. Unfortunately, in these cases, we missed the observation of blood flow in the fetal middle cerebral arteries.
Five cases with serious complications associated with placental circulatory imbalance between the twins developing during the third trimester of monochorionic diamniotic twin pregnancy.
Twenty-five cases of the MD twin pregnancies were delivered preterm (28.4%, 6 vaginal and 19 cesarean deliveries). The remaining 58 cases were delivered at term (65.9%, 12 vaginal and 46 cesarean deliveries) uneventfully. In addition, 66 neonates in the MD twin pregnancies without serious complications (39.8%) were small for gestational age.
Discussion
In cases of MD twin pregnancies without any abnormal findings until the second trimester of pregnancy, 65.9% could be delivered uneventfully at term; however, 5.7% had serious complications associated with placental circulatory imbalance during the third trimester of pregnancy. The rate of complications was lower than that in one previous Japanese study by Murata et al, 16 who reported that the prevalence of TTTS onset after 28 weeks of gestation was 4%, because their study included cases of AF discordance, AF abnormality in one or both twins, and fetal growth abnormalities at ≤28 weeks of gestation. Therefore, the current study extracted only cases of placental circulatory complications that solely developed during the third trimester of pregnancy.
In all five cases with serious complications associated with placental circulatory imbalance in this study, no abnormal ultrasonographic findings or symptoms were recognized one or two weeks prior to the diagnosis. In an earlier study by Thorson et al, 3 it was found that a maximum surveillance interval of 14 days for MD twins may lead to diagnosis at an earlier stage, earlier intervention, and better outcomes of TTTS, because an interval of greater than 14 days from the previous ultrasonogram was closely associated with the detection of higher stage TTTS. In this study, higher stage TTTS complicated by perinatal death in both twins was observed in only one case (1.1%) of all MD twin pregnancies; however, our data may indicate that the development of placental circulatory imbalance between the twins during the third trimester is rapid, and an ultrasound examination interval of 14 days or shorter is required. Otherwise, women with MD twin pregnancies should be recommended to visit an emergency department immediately when they have feelings of discomfort.
In addition, unfortunately in this study, we did not routinely perform the measurement of middle cerebral artery waveforms. Based on the current cases, we now routinely measure middle cerebral artery waveforms, especially during the third trimester. Lewi et al 10 observed that TAPS was diagnosed in more than one-third of pregnancies with late-onset discordant growth, in contrast to no pregnancies with early-onset discordant growth and only 3% of pregnancies with concordant growth.
Conclusion
About 66% of uncomplicated MD twin pregnancies at 28 weeks of gestation could be delivered uneventfully at term. However, serious complications due to placental circulatory imbalance between the twins occurred in about 6% during the third trimester of pregnancy.
Author Contributions
Performed all the work: SS. Author reviewed and approved of the final manuscript.