
Abstract
Twin-twin transfusion syndrome (TTTS) is a severe complication of monochorionic twin pregnancies. A starry sky liver is characterized by sonography as liver parenchyma appearing hypoechoic due to swelling of liver cells, accentuating the periportal collagen. It has been associated with several pathological processes but has only recently been reported with TTTS. This case study is a report of a twin pregnancy that developed TTTS in which a starry sky liver was visualized in the recipient twin.
Twin-twin transfusion syndrome (TTTS) is a serious complication occurring in up to 15% of monochorionic twin pregnancies. 1 The etiology of TTTS is abnormal vascular connections within a shared placenta, which results in an unbalanced perfusion to the developing fetuses. 2 It is important to identify TTTS as soon as possible because of the high perinatal loss rate and increased risk of neurologic damage. 3 Although not all monochorionic twin pregnancies will develop TTTS, guidelines developed by the Society of Maternal Fetal Medicine recommend following twin pregnancies closely with sonography every 2 weeks from 16 weeks gestation until delivery to evaluate for TTTS. 2 Most cases of TTTS are identified in the second trimester when established sonographic markers indicative of TTTS are appreciated. 3 The case presented in this article was unique in that a starry sky liver in the recipient twin was also visualized.
Case Report
A 30-year-old gravida 1 para 0 woman was sent to our institution to assess chorionicity and amnionicity of a known twin pregnancy. A sonographic examination was done at 10 weeks 3 days, using a Philips iU-22 ultrasound system (Philips Medical, Bothell, WA) with a 5-1 MHz curvilinear transducer. Sonography confirmed a monochorionic diamniotic pregnancy that was consistent with dates by crown-rump lengths. A single posterior placenta was visualized. A sequential screen was performed at 11 weeks 4 days, which was reassuring except for an increased nuchal translucency on twin B. The sequential results gave the fetuses a 1:10 risk for Down syndrome; however, the patient was not interested in invasive testing. The patient returned for a subsequent sonogram at 16 weeks 0 days to assess anatomy and interval growth. Although several anatomic structures were not optimally visualized because of small fetal size, fetal growth was appropriate and no sonographic markers of trisomy 21 were seen. Additional sonograms were performed at 18, 20, 22, 24, 26, 28, and 30 weeks’ gestation, all of which were unremarkable.
Fetal echocardiography was also performed at 20 weeks, secondary to the increased nuchal translucency visualized on twin B in the first trimester. No overt cardiac abnormalities were appreciated in either fetus.
A follow-up sonogram performed at approximately 32 weeks gestation showed several findings consistent with TTTS. Oligohydramnios was seen in twin A’s sac, with a maximum vertical pocket (MVP) of 0 cm. The fetus’s stomach and bladder were visualized but small. Twin A’s abdominal circumference was lagging behind gestation age by more than four weeks, and its estimated fetal weight was in the 16th percentile at 1542 g. An umbilical Doppler was done, which showed an elevated systolic/diastolic ratio of 8.6 in one of the arteries. Twin B had an MVP of 10 cm. The bladder appeared mildly enlarged. Growth was adequate at 2020 g, which was consistent with the 57th percentile; twin growth was discordant at 24%. Of note, twin B’s liver was hypoechoic with increased periportal echogenicity, giving the liver a “starry sky” appearance (Figures 1 and 2).

Transverse image of the fetal liver in the recipient twin, exhibiting a hypoechoic, “starry sky” appearance.

Longitudinal image of the starry sky appearance of the liver in the recipient twin.
It was discussed with the patient that the findings for twin A of oligohydramnios (and polyhydramnios in twin B), discordant growth, the small bladder, intrauterine growth restriction (IUGR), and the abnormal umbilical artery Doppler were concerning for late onset of TTTS. The patient was admitted to the antepartum unit for administration of betamethasone, fetal monitoring, and a potential amnioreduction. Fetal heart monitoring was reassuring, and following the course of betamethasone, the twins were delivered successfully at 32 weeks 0 days by cesarean section.
Discussion
TTTS is a serious complication seen in monochorionic twin pregnancies. 1 A monochorionic pregnancy is diagnosed when a single shared placenta is visualized. 4 TTTS is caused by abnormal vascular communications within a single placenta that result in an unbalanced blood supply to both fetuses. 5 In TTTS, one twin is considered the “recipient” while the other is commonly termed the “donor.” 1 A donor twin commonly develops anemia, IUGR, hypovolemia, and oligohydramnios because of a portion of their normal blood supply being shunted to their cofetus. 1 Inversely, the recipient or larger twin will experience hypervolemia, cardiac overload, and polyhydramnios due to the excess supply of blood they are receiving. 1 Several sonographic indicators are used to make the diagnosis of TTTS. These include oligohydramnios (MVP < 2 cm) in the donor twin with polyhydramnios (MVP > 8 cm) in the recipient and discordant growth >20% between the twins. 1 Nonvisualization of the bladder and stomach in the donor twin secondary to oligohydramnios is commonly found. 1 If oligohydramnios is severe enough, it will make the membrane difficult to visualize and look “stuck” to the donor twin. This in turn will cause the fetus to appear immobile and “stuck” to the uterus. 6
A staging system developed in 2003 by Quintero 5 is commonly used to characterize the severity of TTTS (Figure 3). In stage I, polyhydramnios and oligohydramnios are identified, but the bladder of the donor twin is still able to be identified. In stage II, the bladder of the donor twin is not seen throughout 60 minutes of scanning. In stage III, pulse Doppler evaluation will show absent or reversed end-diastolic flow in the umbilical arteries, reversal of flow in the ductus venosus, or a pulsatile umbilical vein. In stage IV, hydrops with be present in either twin. In stage V, the demise of either fetus will be visualized. 5 Fetuses with TTTS are at an increased risk of neurologic, cardiac, and developmental disorders, as well as in utero demise. 7 Because of the potential risk to the developing fetuses, several interventional options have been put into practice, which include serial amnioreduction, laser photocoagulation of placental anastomoses, intermembrane amnioseptostomy, and premature delievery. 3 Timing of delivery for TTTS pregnancies is contingent on several factors, including disease stage, progression, fetal growth, and response to previous treatment. 2 Because of the late onset of TTTS at 32 weeks in this case, early delivery of the fetuses was deemed prudent.
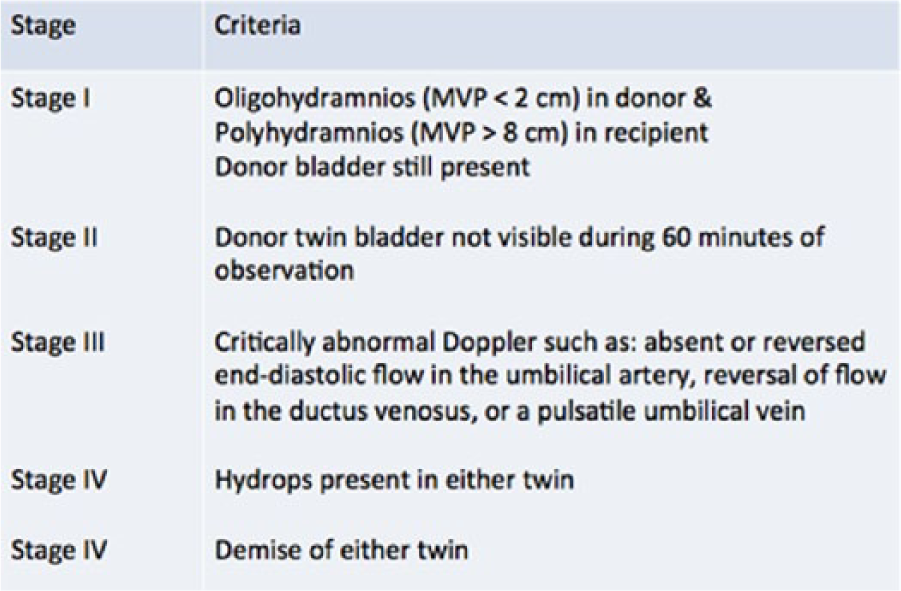
Quintero staging criteria for twin-twin transfusion syndrome. Modified from Quintero R: Twin-twin transfusion syndrome. Clin Perinatol 2003;30:591–600.
The term starry sky refers to the sonographic characteristics of a liver that has experienced diffuse swelling, which causes the parenchyma to appear hypoechoic, accentuating the naturally hyperechoic portal triad walls. 8 The appearance of a starry sky liver was originally synonymous with acute hepatitis but over the years has been identified in patients with leukemia, toxic shock syndrome, Burkett’s lymphoma, and right-sided heart failure. 9 It has recently been reported in a case of TTTS 10 and a less common variant of TTTS, anemia-polycythemia sequence. 11 The case reported by Segev et al 10 described a starry sky liver in conjunction with TTTS that closely resembled our case. However, in their case, the starry sky liver was first noted at a 20-week sonogram, prior to other sequelae of TTTS, which were present at 21 weeks. Tricuspid regurgitation and biphasic flow in the inferior vena cava were also visualized in their case, which the author suggested was caused by acute volume overload. The author hypothesized that right-sided heart failure eventually led to liver edema, which caused the starry sky appearance.
Conclusion
The appearance of a starry sky liver, although not common in the setting of TTTS, may be appreciated in certain cases. It is important to be aware that this may occur secondary to a volume overload and, if appreciated on sonography, may be an early sign of TTTS.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.