
Abstract
Gallstones are rarely seen in preterm neonates with most cases reported in term singletons without any identifiable risk factors. Although most cases are self-resolving, neonatal gallstones can be associated with significant complications. We report a case of 34-week gestation monochorionic diamniotic twins with twin anemia-polycythemia sequence (TAPS) where the recipient twin presented with gallstones on the first day of life. To the best of our knowledge, this is the first case of gallstones in preterm twins following TAPS.
Introduction
Cholelithiasis, or the presence of gallstones in the gallbladder, is rare in neonates and infants with a reported incidence of <1%. 1 Although several predisposing risk factors have been described in association with neonatal gall stones, most cases occur in singletons in the absence of any identifiable risk factor. On antenatal ultrasounds, gallstones are usually seen in the third trimester. 2 Due to its rarity, gallstones can cause significant anxiety and stress among parents, and many healthcare professionals may not be familiar with the condition. Most cases of neonatal gallstones are benign and self-resolving, 3 although significant complications have been described with them. Healthcare workers looking after neonates should be aware of possible risk factors, course, and outcomes of infants with gall stones so that proper counseling can be provided to parents.
Case report
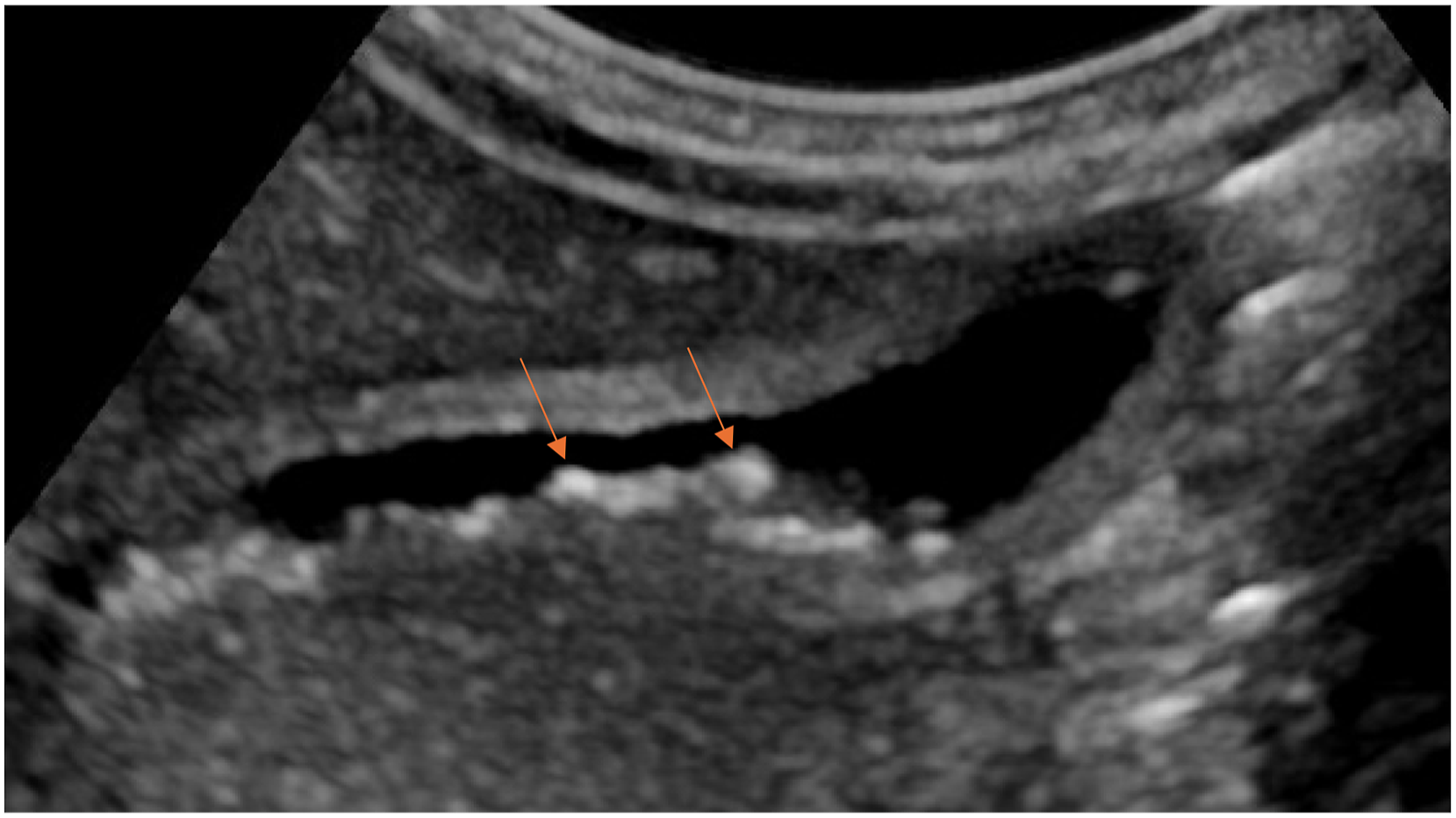
We report a unique case of monochorionic diamniotic (MCDA) twins with twin anemia-polycythemia sequence (TAPS) born at 34 weeks of gestation where the recipient twin was found to have gall stones on day 1 of life. We believe this to be the first reported case of gallstones in the recipient twin, the first of MCDA twins with TAPS. 34-week postmenstrual age (PMA) MCDA twins were delivered via planned cesarean section due to TAPS and cervical shortening on 3rd trimester antenatal ultrasounds. Twin 1’s birth weight was 2.085 kg, 46th percentile according to Canadian standards, and appropriate for gestational age. Baby was vigorous and cried at birth with APGAR scores of 8 at 1 minute and 9 at 5 minutes of life. Mother was a 35-year-old Gravida 2, Para 2 with blood group O positive and negative antibody screen, group B streptococcus status unknown, and protective serology (non-reactive syphilis, hepatitis B, hepatitis C, and HIV and immune to rubella and varicella). She had abnormal gestational diabetes mellitus screen and positive glucose tolerance test and met the criteria for gestational diabetes which was managed with metformin. She also had a past medical history of Graves’ disease and was on methimazole during pregnancy. Her TSH during pregnancy was 1.90 mIU/L and she remained euthyroid throughout pregnancy. Her last TSH receptor antibody was done in March 2023 which was normal with a level of 3.21IU/L. She was followed with serial antenatal ultrasounds for monochorionic and diamniotic gestation. Antenatal ultrasounds were reassuring with no fetal abnormalities or growth discordance between both fetuses until 32 weeks PMA, when new evidence of TAPS with no twin-to-twin transfusion syndrome (TTTS) was noted. Follow up antenatal ultrasound showed mild stable TAPS with hypo-echogenicity in liver and placenta in Twin 1 as compared to Twin 2 with normal dopplers. Repeat ultrasound at 33 weeks and 6 days PMA again showed evidence of TAPS with hypo-echoic (starry sky) (Figure 1) liver and placenta which was more pronounced than on previous ultrasounds. Mother received a full course of antenatal steroids at 32 weeks to mitigate complications associated with prematurity. Following birth, the infant was admitted to the Neonatal Intensive Care Unit (NICU) due to prematurity with respiratory distress, necessitating Continuous Positive Airway Pressure (CPAP) and oxygen support initially, which was successfully weaned to room air by day 3 of life. Physical examination of baby was normal as per gestational age except for syndactyly of 2nd and 3rd toes on both feet. There was no hepato or splenomegaly. On postnatal day 1, an abdominal ultrasound was performed to follow on the antenatal finding of starry sky and echogenic appearance of the liver. The ultrasound showed calculi in gallbladder (Figure 2). Gallbladder was collapsed with no signs of acute inflammation. Bile duct measured 0.1 cm with no intrahepatic bile duct dilation. This baby was the recipient twin in TAPS. CBC done at birth showed a normal high hematocrit (0.64) compared to normal value (0.45) for Twin 2 (donor). Liver function test on day 2 of life were normal with ALT of 10 U/L and gamma glutamyl transferase of 132 U/L. Highest bilirubin was 149 micromol/L on day 5 and the baby never required phototherapy. Thyroid function test was done in context of maternal Graves’ disease which showed normal TSH and T4 with undetectable thyroid receptor antibodies. Follow up ultrasound was done at day 19 which showed completely collapsed gallbladder with wall apposition and no bile. Infant remained completely asymptomatic during the NICU stay and the plan was to follow the baby with abdominal ultrasound after discharge. Twin 2 course during NICU stay was uncomplicated. Abdominal ultrasound for this baby on the day 1 of life was unremarkable with no findings of gall stones or any other abnormalities. Trans abdominal view showing starry sky appearance on ultrasound done one day before birth. Abdominal ultrasound showing gallstones on the second day of life.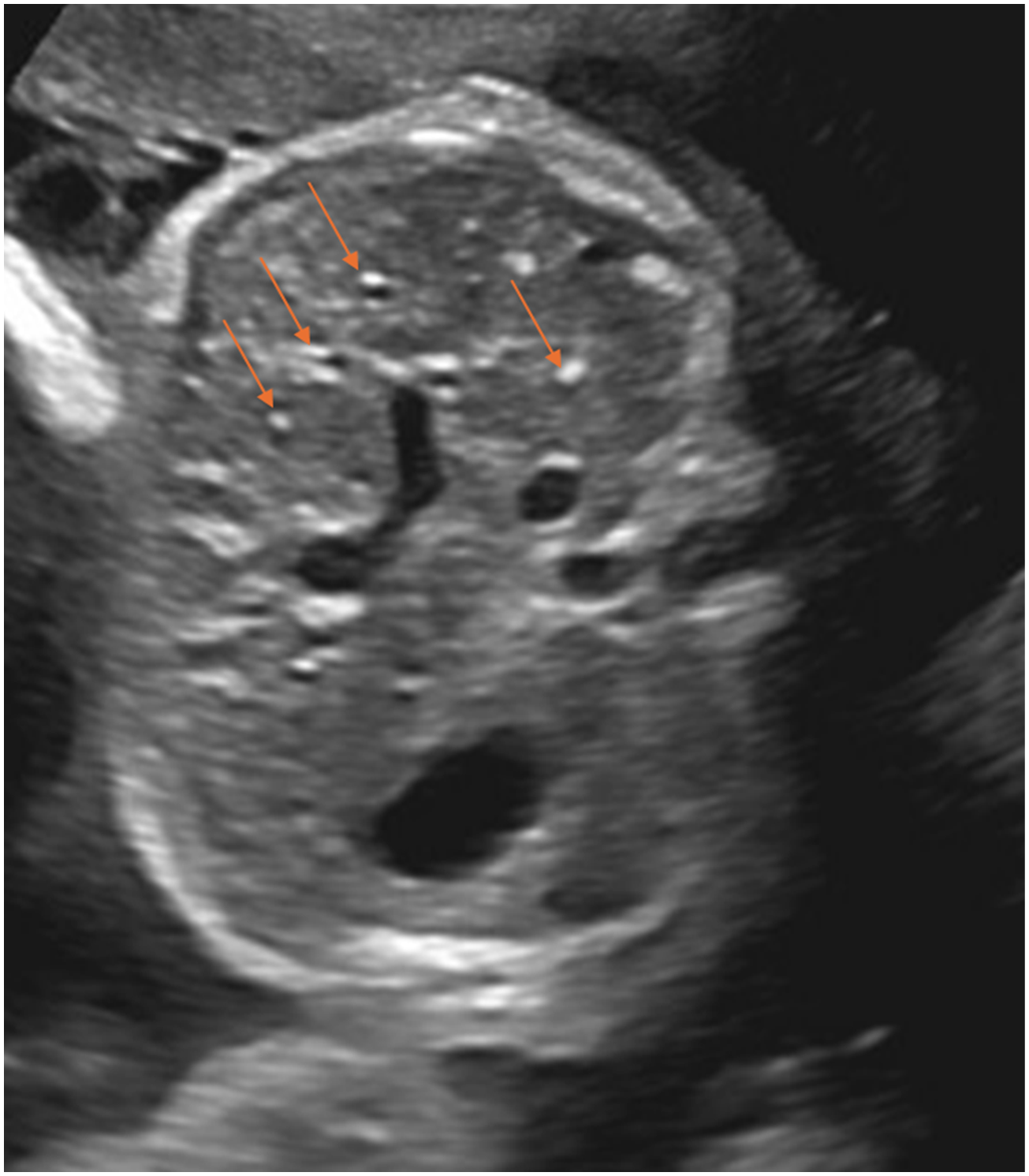
Discussion
In neonates, cholelithiasis is typically asymptomatic and usually resolves spontaneously without any medical intervention. 3 This condition is associated with several risk factors, including prematurity, hemolytic disorders, congenital heart disease, total parenteral nutrition (TPN), and disruptions in enterohepatic circulation. 4 The pathogenesis of cholelithiasis in preterm infants is poorly understood. Two divergent theories have been proposed to explain gallstones but have not been proven scientifically. One theory state that maternal and placental estrogens lead to increased cholesterol secretion and decreased bile acid production. Conditions associated with elevated maternal estrogen and progestin levels such as twin pregnancy may predispose patients to fetal cholelithiasis by increasing cholesterol secretion and reducing bile acid synthesis. 2 The other states that gallstones are related to increased hemolysis due to Rhesus or ABO blood alloimmunization, spherocytosis, sickle cell anemia, and other causes of hemolysis may contribute to the formation of gallstones. In our case, there was no apparent hemolysis in the recipient twin and the baby did not show any evidence of hemolysis after birth. There was no set up for ABO or Rhesus incompatibility. The baby also did not have any reported risk factors associated with gallstones in neonates. There was no family history of gallstones, and no maternal history of liver disease or use of third generation cephalosporins. The mother had normal body mass index and the baby was not small for gestational age. Gestational diabetes has been reported as an inconsistent risk factor for gall stones in newborns. Multiple studies have demonstrated that infants born to diabetic mothers often exhibit increased erythropoiesis. This phenomenon may be linked to intrauterine hypoxia, which arises from the combined effects of hyperinsulinism and hyperglycaemia. 5 Newborns generate bilirubin at a rate of approximately 6–8 mg per kg per day which is over twice that of adults. Also, newborns reabsorb much larger quantities of unconjugated bilirubin by enterohepatic circulation, than does the adult. This production of unconjugated bilirubin is even more increased due to neonatal polycythemia due to faster turnover of red blood cells. 6 We speculate that the higher hematocrit in the recipient twin in our case led to increased formation of indirect bilirubin which contributed to the formation of gallstones. The presence of diabetes in the mother could have also contributed. 5 Syndactyly has previously not been reported with neonatal gallstones, and it is difficult to say if this is an actual association or an incidental finding. This baby was born to Gravida 2 Para 2, 35-year-old mother. As reported in case series by Schwab et al, 7 most common maternal age associated with fetal cholelithiasis is 17–42 years with median gravidity and parity of 2. Most cases of fetal cholelithiasis are diagnosed in 3rd trimester of pregnancy with median gestational age to diagnose antenatal fetal gallstones as 34.7 weeks. 2 No sex predilection is described with gallstones. The repeat abdominal ultrasound on day 19 showed a contracted gall bladder where the gallstones could not be visualized. However, it is a common belief that neonatal cholelithiasis resolves spontaneously with hydration and adequate feeding, Stringer et al. have proposed that characteristic conditions of the postnatal period, such as increased bile flow and changes in its composition, may allow for the dissolution of gallstones and their subsequent passage through the bile ducts. 8 This infant will have a repeat ultrasound at 3 months of life and earlier if there are any clinical indications. The “starry sky” sonographic pattern is a distinctive finding observed in diffuse liver pathology, 9 which was originally synonymous with acute hepatitis but over the years has been identified in patients with leukemia, toxic shock syndrome, Burkett’s lymphoma, and right-sided heart failure. 10 Recently, the starry sky pattern has been reported in association with TTTS and in TAPS, a less common variant of TTTS. 11 TTTS is a condition that occurs in pregnancies with monochronic twin gestation, where there is an imbalance in blood flow between the fetuses via shared placental vessels. TAPS occurs in 5% of MCDA twins due to slow transfer of blood from the donor to the recipient through small anastomosis in the placenta. 12 Diagnosis of TAPS relies on abnormal doppler ultrasound findings, notably an increased peak systolic velocity in the middle cerebral artery (MCA-PSV) in the donor twin, indicative of anemia, and a decreased MCA-PSV in the recipient twin, suggestive of polycythemia. 9 This diagnostic approach enables early identification and management of TAPS, facilitating appropriate interventions to optimize outcomes for both twins. The echogenic liver with the starry sky appearance may have resulted in failure to identify the gall stones antenatally. This baby was a recipient twin in TAPS and had high hematocrit of 0.64. These findings highlight the importance of vigilant antenatal monitoring and postnatal assessment in neonates, particularly in cases of monochorionic twins where shared placental circulation can predispose to various complications. The increased utilization of abdominal ultrasonography in clinical practice has led to the incidental discovery of cholelithiasis in infants. Once gallstones are reported in a neonate, the baby should have a detailed history and thorough physical examination and any risk factors identified to prevent not only potential complications such as biliary obstruction, cholecystitis, or pancreatitis but also to avoid unnecessary investigations.
Conclusion
We report an unusual association of TAPS with neonatal cholelithiasis. Although several authors have reported fetal cholelithiasis in previous studies, this is the first report where neonatal cholelithiasis was seen in a monochorionic diamniotic twin who was the recipient after TAPS complicated the pregnancy. This case was without symptoms or complications with normal physical examination except for the presence of syndactyly. Although not reported previously with neonatal gallstones. We believe syndactyly to be an incidental finding. Healthcare workers need to be aware of the natural course of neonatal cholelithiasis to provide proper counseling to parents and avoid unnecessary investigations.
Footnotes
Consent to publish
Written and informed consent was obtained from mother of the case.
Author contributions
SK collected the clinical information and wrote the first draft of the manuscript. PS: Reviewed and revise manuscript. KY: Helped with collection of clinical information and revised and finalized manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.