
Abstract
Background
Brucellosis is a common zoonotic infection throughout the world, and is endemic in Saudi Arabia. Neurobrucellosis is a rare, severe form of systemic brucella infection. Treatment of neurobrucellosis continues to be variable, depending on the location of diagnosis.
Methods
A retrospective patient chart review was undertaken from 1995 to 2010 at King Abdulaziz Medical City, Riyadh, to identify cases of neurobrucellosis following a proposed case definition. Follow-up visits were evaluated to determine response to treatment.
Results
A total of 22 cases of neurobrucellosis were identified from a total of 517 cases of brucellosis. The mean patient age was 42.5 years with a male to female ratio of 1:1. Most antibiotic combinations included doxycycline, rifampin, and cotrimoxazole (36%). Three patients received ciprofloxacin in combination with other antibiotics and showed a satisfactory response.
Conclusion
Combination of antibrucella antibiotics is recommended, but there are no clear guidelines regarding antibiotic selection and duration of therapy. The use of ciprofloxacin in cases of neurobrucellosis should be evaluated.
Introduction
Brucellosis is a common zoonotic infection throughout the world. Brucella species remain important human pathogens in endemic regions, most notably the Mediterranean basin, Arabian peninsula and Indian subcontinent.1,2 More than 500,000 new cases occur annually, but with an uneven global distribution.2,3 Brucellosis is endemic in Saudi Arabia, with an incidence rate of 40 cases per 100,000 population per year. 4 Neurobrucellosis is a rare and severe form of systemic brucella infection, with only 4%–13% of patients with brucellosis having an element of central nervous system involvement.1,2,5,6 Treatment of neurobrucellosis continues to be variable depending on where the case is diagnosed. The objective of our study was to evaluate and discuss newer regimens used to treat neurobrucellosis.
Methods
A retrospective patient chart review from early 1995 to mid 2010 was conducted at King Abdulaziz Medical City, Riyadh. Patient charts were screened for any case of brucellosis. Neurobrucellosis case definition were: clinical manifestations consistent with neurobrucellosis features; including headache, meningitis, encephalitis, myelitis, cerebellar dysfunction, backache, areflexia, paraparesis, proximal nerve radiculopathy, and systemic manifestations; cerebrospinal fluid (CSF) changes consistent with neurobrucellosis, such as pleocytosis, elevated CSF protein level, and low CSF glucose; and either microbiologic evidence of brucellosis (positive blood or CSF culture) or serologic evidence of brucellosis (serum agglutination titer ≥1:160 and CSF serology ≥1:80). Data were collected on the treatment regimen used, the duration of therapy and the final outcome at last follow-up. Patient recovery was classified as complete clinical recovery, partial recovery with some residual neurologic deficit, or death attributable to neurobrucellosis.
Results
We identified 517 cases diagnosed with brucellosis during the 15-year study period. Of these cases, only 20 (4%) patients fulfilled our neurobrucellosis case definition criteria. Another two cases of presumptive neurobrucellosis with clinical manifestations of neurobrucellosis who had refused lumbar puncture but responded to empiric antibrucella therapy were also included.
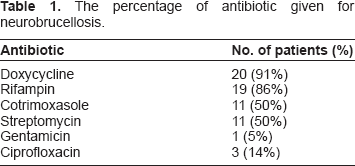
The percentage of antibiotic given for neurobrucellosis.
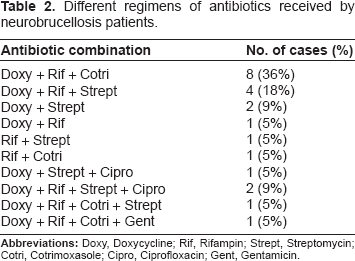
Different regimens of antibiotics received by neurobrucellosis patients.
Discussion
Neurobrucellosis is an uncommon complication of brucellosis. It is reported that about 4%–13% of patients with brucellosis develop neurologic complications.1,5–8 In our retrospective review of neurobrucellosis patients it was shown that most patients had responded favorably to antibiotic treatment, with 96% of the patients recovering completely (73%) or partially (23%). This outcome is consistent with the findings of other investigators. 1 Our patients received different antibiotic combinations with different durations of therapy (5–44 weeks). The combination of antibiotic treatment commonly included doxycycline (91%) and rifampin (86%). The commonest combination of triple antibiotic therapy was doxycycline, rifampin, and cotrimoxazole (36%).
However, three patients (13.6%) received ciprofloxacin intravenously and were then switched to an oral formulation. These patients recovered completely after finishing treatment. Fluoroquinolone therapy for brucellosis was suggested by several investigators as an alternative therapy.4,9–14 Ciprofloxacin is an agent that would have a better concentration in CSF because it crosses the blood-brain barrier more than doxycycline, rifampin, cotrimoxazole, and aminoglycosides. The parameter that could preclude use of quinolone for treating brucellosis may be the risk of development of resistance. However, similar worries concerning emergence of resistance to rifampin have not impeded its extended use for treatment of brucellosis. 15 The other concern is to reserve rifampin for tuberculous infection.
We realize that the small sample size of our study was too small for subgroup analysis based on regimens and/or duration of therapy applied. This makes it difficult to draw strong conclusions; however, a large randomized clinical trial comparing a ciprofloxacin-based regimen of multiple (triple) antibiotic therapy for neurobrucellosis treatment is needed to evaluate this important question. We also recommend using combination antibiotic therapy for at least 12 weeks in all cases of neurobrucellosis.
Footnotes
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.