
Abstract
Introduction
Antibiotics are essential and abundantly prescribed in hospitals because of their effectiveness and lifesaving benefits. However, the unnecessary use of antibiotics has been observed in earlier studies, and it has persisted through recent years as a major issue since it is one of the leading causes of antibiotic resistance. The increase in antibiotic resistance nowadays is one of the most critical concerns in global public health around the world. The objective of this study was to evaluate the knowledge and perceptions related to antibiotic prescription among physicians at our medical centers.
Method
A cross-sectional survey of non-infectious diseases specialized physicians. The study was conducted during 2015 at two tertiary care centers in Riyadh, Saudi Arabia.
Result
Of the 107 returned questionnaires, 93 were complete and valuable. Most respondents (82%) perceived antibiotic resistance to be a critical problem globally, and 78% also think that it is a very important national problem. These attitudes did not differ across specialty or level of training. Widespread antibiotic use and inappropriate empirical choices were believed by 81% of the participants to be important general causes of resistance. Only half of respondents thought that antibiotic restriction is a useful intervention to decrease the antibiotic resistance. The physicians believed educational interventions are the most useful and effective way to improve prescription patterns and decrease antibiotic resistance. Complications due to infection with resistant organisms were acknowledged by almost all of the participants, with some differences in their estimations of how often it will occur.
Conclusion
Antimicrobial resistance, globally and nationally, is considered as a serious threat, and physicians in this survey acknowledged that. Among the most significant factors is antimicrobial misuse, either by overprescribing or providing inappropriate drugs with some ambivalence, as well as the importance of hand hygiene and antibiotic restrictions. By adhering to local guidelines, continuous education, and other practical interventions, the burden of resistance can be alleviated, as highlighted in this survey.
Introduction
Antibiotics are essential and abundantly prescribed in hospitals because of their effectiveness and lifesaving benefits. However, the unnecessary use of antibiotics has been observed in earlier studies, and it has persisted as a major issue. Antibiotic overuse, incorrect dosing, and extended duration are some of the leading causes of antibiotic resistance. 1 4 The increase in antibiotic resistance nowadays is one of the most critical concerns for public health around the world. On the national level, recent articles have demonstrated an increasing pattern of infections with multidrug-resistant organisms in Saudi Arabia, including both gram-positive and gram-negative bacteria. 5 7 The emerging bacterial resistance to antibiotics is increasing the challenges faced by physicians and institutions. 8 10 Data on the determinants of the prescription methods of individual physicians in different specialties are limited. Antibiotic prescription by general practitioners in the primary care setting was demonstrated as potentially inappropriate in several studies. 11 14 There are few studies focusing on inhospital physician behavior and attitudes toward antibiotic use. A recent local study mentioned that general physicians lack consistency in prescription aptitude and the use of practical educational resources; also, they do not strictly follow national and local guidelines. Although the respondents in that study have a clear theoretical knowledge of antimicrobial resistance and careful use of antibiotics, 15 antibiotic misuse was documented in several studies focusing on the prescription pattern in adult and pediatric patients. 16 19 In a recent survey in local tertiary care centers, participants were aware of the growing challenge of antimicrobial resistance, but were unaware of the specific antimicrobial resistance rates and patterns in their institutions. 20 The objective of this study was to further evaluate knowledge and perceptions about antibiotic prescriptions among physicians at our medical centers.
Method
This study was conducted at two tertiary care centers in 2015 between August and October, consisting of a cross-sectional survey of noninfectious diseases specialized by physicians. The research was approved by the research committee of King Abdullah International Medical Research Center. Different levels of physicians from several departments, eg, anesthesia, intensive care, internal medicine, surgery, obstetrics/gynecology, emergency medicine, pediatrics, and family medicine, working at King Abdulaziz Medical City and King Saud Medical City in Riyad, Saudi Arabia, were invited to participate. The invitation was sent either by e-mail or SMS messages, targeting all physicians at these two institutions, and participation was voluntary. An online questionnaire, including 25 items, was created in an easy access, smartphone-friendly website. All participants read of the questionnaire type and agreed to the confidentiality conditions before beginning the questionnaire. No personal identifying information was required, and strict confidentiality was maintained. Demographic data including gender, specialty, duration of clinical practice, extra training for infectious diseases, and professional status (intern, resident, senior/chief resident, consultant) were all collated. Other items focused on the physicians' opinions of a problem's magnitude regarding antibiotic resistance were as follows: their knowledge of the local hospital type and the prevalence of antibiotic resistance, their beliefs about the contributors to the development of antibiotic resistance, and their attitudes on useful interventions designed to address the problem. Most questions about beliefs and attitudes used 3- to 6-point Likert-type response options from “useful” to “unuseful,” “extremely rare” to “often,” and “excellent” to “poor.” There were other graded response options such as a 6-point scale that included “not important” to “extremely important.” Some questions were also “yes/no” types. To assess the knowledge of antibiotic resistance, physicians were asked to choose the most common resistant organisms at their hospitals, restricted antibiotics at the hospitals that would require a specialist's countersignature, and avoided antibiotics that were more prone to induce antibiotic resistance. Basic knowledge about antibiotic choices in common infections and the best duration of therapy were inquired about along with the factors that would influence their antibiotic choices. The participants were then asked to grade their current knowledge about antibiotic resistance and state whether they needed to improve it or not. Using Microsoft Excel 2011, data were collected and analyzed; all data were collected using the Statistical Product and Service Solutions software, versions 8 and 9 (SPSS Inc.).
Result
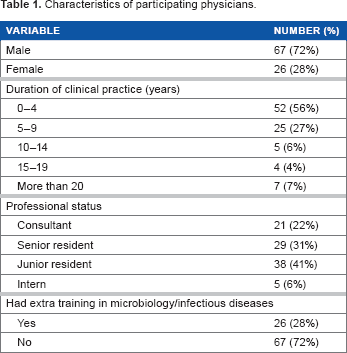
A total of 200 invitations were sent to the physicians at both institutions, with a response rate of 54%. Among 107 returned questionnaires, 93 were complete and valuable. The sample included 86 internal medicine physicians, who represented 93% of the responders; 21 (23%) consultants, 29 (31%) senior residents, 37 (40%) junior residents, and 6 (6%) interns were also included. Most (67) of the participants were male (72%), and more than half of them were relatively new to clinical practice (less than four years; Table 1).
Characteristics of participating physicians.
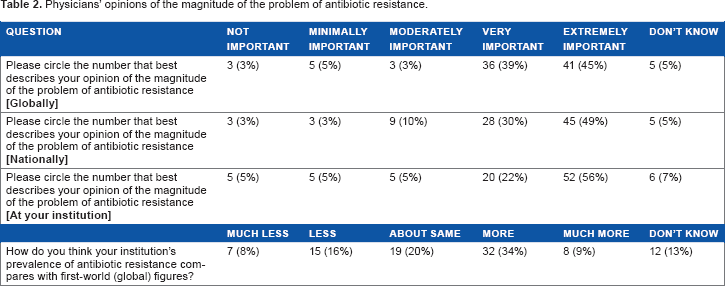
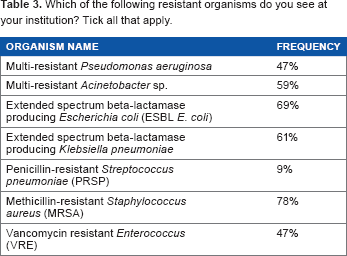
Most respondents (82%) perceived antibiotic resistance to be a critical problem globally, and 78% also thought that it is a very important national problem. These attitudes did not differ across specialties or levels of training. About 20% believed that the magnitude of this issue was similar in their institutions when compared to global reports. More than two-thirds of the participants were able to identify the most common resistant organisms in the institution correctly (ie, multidrug-resistant
Physicians' opinions of the magnitude of the problem of antibiotic resistance.
Which of the following resistant organisms do you see at your institution? Tick all that apply.
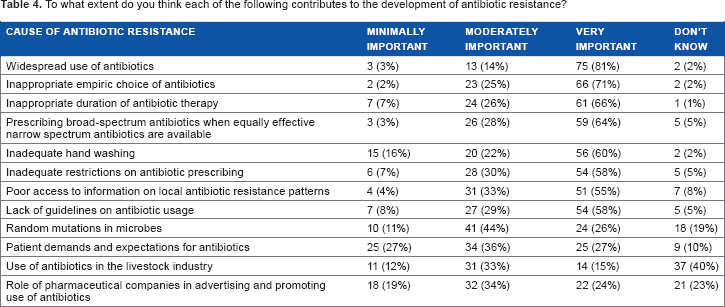
To what extent do you think each of the following contributes to the development of antibiotic resistance?
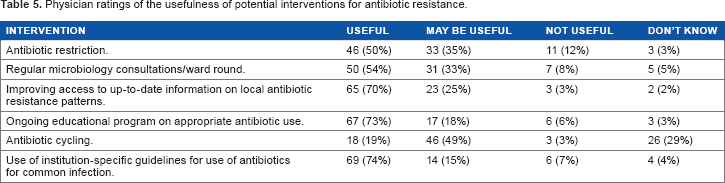
The beliefs of the screened physicians with regard to the effectiveness of informational interventions that they think are the most useful ways to improve the prescription pattern and decrease antibiotic resistance are local specific guidelines for use of antibiotics, ongoing educational programmes on appropriate antibiotic use, and improving access to updated local antibiotic resistance profiles. The responses of the physicians regarding the usefulness of other possible interventions differed (Table 5).
Physician ratings of the usefulness of potential interventions for antibiotic resistance.
With some variation in the indicated duration of therapy with bacterial infections, most of the participants choose to provide long treatment periods (14 days or more) to patients with bloodstream infections and hospital-acquired infections. Approximately 59% and 37% of the physicians think that 7 to 10 days are optimal for treating community-acquired pneumonia and urinary tract infections, respectively, while 23% and 25% think that five days are enough. Around half of the physicians believe that using particular antibiotics, such as ceftriaxone, ciprofloxacin, amoxicillin-clavulanate, and piperacillin-tazobactam, are more likely to induce the development of antibiotic resistance when compared to other classes of antibiotics.
Complications due to infection with resistant organisms were acknowledged by almost all of the participants, with some difference in their estimation of how often these would occur. The main complications recognized were prolonged hospital stays and increased costs of hospitalization, but a few mentioned organ failure and death (Table 6).
How often would you say that infections with resistant organisms contributed to the following outcomes?

Although most of the participants have a good awareness of their hospital antibiotic restriction policy and the need for infectious disease specialist approval, some of these physicians are clearly unfamiliar with this policy and the names of restricted antibiotics. Notably, 70% were aware that ceftriaxone is not restricted, while 81% were aware that meropenem is a restricted antibiotic that needs specialist approval. The responders believed that the current level of antimicrobial restriction should be maintained at 17% or further increased to 60%.
Approximately two-thirds of the participants assumed that their present knowledge of antibiotics and antibiotic resistance is between average and good, but almost all of them (92%) preferred having a refresher course on antibiotics and the recent guidelines. Upon asking the participants about their first-choice antibiotic for common bacterial infections, they choose amoxicillin–clavulanate (46%) or ceftriaxone (31%) for treating community-acquired pneumonia. In treating urinary tract infection, most physicians preferred using ciprofloxacin (36%), ceftriaxone (18%), or Bactrim (16%), while more than 57% chose piperacillin–tazobactam to treat ventilator-associated pneumonia. Variable results were noted in treating surgical wound infections, and the main choices were amoxicillin–clavulanate, piperacillin–tazobactam, or ceftriaxone. One-third preferred to use piperacillin–tazobactam for intra-abdominal sepsis, followed by meropenem and metronidazole.
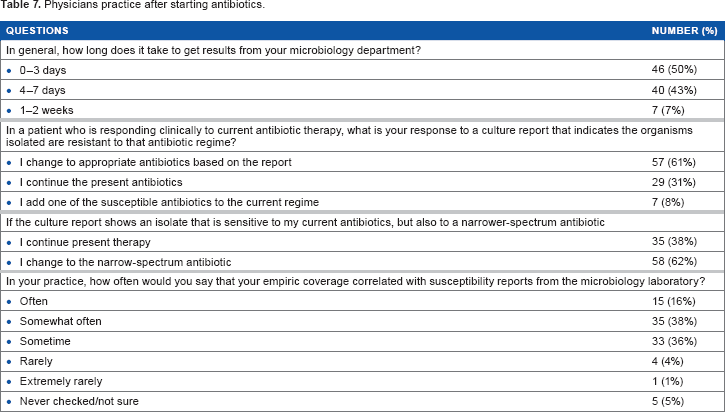
Half of the physicians in our survey expected a microbiological definition of the organism and its sensitivity in 3 days or less. They are most likely going to change the antibiotic according to the microbiology report even if the patient is clinically improving. As many as 60% of the physicians will de-escalate the antibiotic based on the sensitivity pattern to a narrower spectrum, if possible (Table 7).
Physicians practice after starting antibiotics.
Discussion
Our survey confirms that physicians are conscious and aware of the issue of antibiotic resistance in the inpatient setting, locally and around the world. They were also mostly aware of the specific resistant organisms and their institutions but not cognizant of their rates and revisions, despite the availability of antibiograms of both. This may indicate that personal experience with antibiotic resistance was the most likely reason for perceptions about importance.
Widespread antibiotic use and inappropriate empirical choices were believed to be important general causes of resistance to 81% of the participants, and on the other side, only half of them thought that antibiotic restriction is a useful intervention to decrease antibiotic resistance. Interestingly, it showed an apparent discrepancy in their estimation. The moderate approval of poor hand hygiene as a critical cause of antibiotic resistance may reflect a need for the awareness of the usefulness of this simple practice. It was noted that physicians are not exposed to nonclinical causes of antibiotic resistance like the basic bacterial mechanism of resistance and the use of antibiotics in the livestock industry. All of these risk factors of developing antimicrobial resistance that are mentioned in Table 4 were identified as carrying the risk of the emergence and spread of resistant bacteria, including those capable of causing infections in both animals and people.4,21
According to IDSA guidelines, patients with uncomplicated urinary tract infections or community-acquired pneumonia should be treated for a minimum of 5 days22,23 and those with bacteremia should be treated for a minimum of 7–10 days, 24 which showed that the physician tends to use antimicrobials for a longer duration than recommended. According to multiple reports, the extensive use of third-generation cephalosporin antibiotics is developing more resistant bacteria (mainly ESBLs). Also, some interventions showed that discouraging the use of ceftriaxone and ceftazidime will reduce the rate of ESBL bacteria. 25 27 About half of the participants seem to have an idea about this concept, which is acceptable for the nonspecialized physician. The response of the physicians after the microbiological identification and the susceptibility pattern showed that we have great room for improvement, as one-third of them would not replace the empirical antibiotic for a narrower spectrum.
Although an earlier article stated that physician education has a weak effect in changing physician practice and behavior, 28 others proved that a multifaceted approach could be successful. 29 32 Our participants addressed this point, as well as the need for further training and a regular educational program, to improve their antibiotic prescription practice. It is necessary that the informational intervention is accompanied by practical implementations such as computerized physician order entry; this will help increase acceptance by clinicians and will sustain the effectiveness of positive changes. A few studies showed that consulting infectious diseases specialty is important to reduce inappropriate antimicrobial therapy; it improves outcomes and reduces the risk of resistance. 33 35 This consultation service is usually available and active in the reference hospitals, and it should be utilized.
Our study focused on physicians' attitudes on antibiotic resistance in the inpatient setting and provided additional information to the previous work. To minimize potential bias, we opened our survey in a neutral manner and ensured complete respondent confidentiality. Infectious diseases specialists were excluded from the study, as we were targeting physicians who face common infections. The study limitations included surveying mainly internal medicine physicians, which may make the general data differ from a scenario where surgeons, intensivists, and hematologists, for example, are included as well. The number of the respondents is relatively small compared to the size and capacity of the institutions.
In summary, antimicrobial resistance, globally and nationally, is considered a serious threat, as acknowledged by physicians in this survey. Among the most significant factors is antimicrobial misuse, by either overprescribing or providing inappropriate drugs with some ambivalence, as well as the importance of hand hygiene and antibiotic restrictions. By adhering to local guidelines, continuous education, and other practical interventions, the burden of resistance can be alleviated, as highlighted in this survey.
Author Contributions
Conceived and designed the experiments: Binsalih, Alalwan, Alothman. Analyzed the data: Algwizani, Alsulaiman. Wrote the first draft of the manuscript: Bosaeed, Alothman. Contributed to the writing of the manuscript: Alsulaiman, Binsalih. Agree with manuscript results and conclusions: Algwizani, Alalwan, Alothman, Alsulaiman, Binsalih, Bosaeed. Jointly developed the structure and arguments for the paper: Bosaeed, Alothman. Made critical revisions and approved final version: Algwizani, Alalwan, Alothman, Alsulaiman, Binsalih, Bosaeed. All authors reviewed and approved of the final manuscript.