
Abstract
Objectives
Hematologic abnormalities, indicated by a deranged full blood count, are common manifestations and important prognostic tools for human immunodeficiency virus (HIV) infection and AIDS. This study aimed to determine the prevalence of cytopenia and its relationship to the degree of immunosupression in HIV treatment-naïve patients.
Methods
This was a cross-sectional study of treatment-naïve HIV-infected clients who enrolled at the HIV clinic of Lagos State University Teaching Hospital (LASUTH) between December 2009 and June 2010. Participants had samples taken for full blood count and CD4 counts, which are free routine pre-requisite and pre-treatment evaluations done for all registered HIV patients at LASUTH. They were asked to fill the structured questionnaires to obtain demographic data, with assistance if necessary.
Results
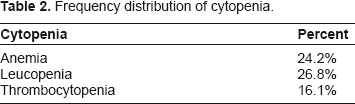
A total of 205 cases were reviewed: 24.2% had anemia (PCV < 30%), 26.8% had leucopenia (white blood cell <4,000/L) and 16.1% had thrombocytopenia (platelet count <150,000/L) at enrollment. The degree of cytopenia was directly related to the degree of immunosupression.
Conclusion
About one-fifth of HIV treatment-naïve patients were cytopenic at enrollment and the degree of cytopenia was directly related to the degree of immunosupression. It is necessary to investigate various causes of cytopenia in these patients so as to administer a specific intervention.
Introduction
Hematologic parameters (ie, packed cell volume (PCV), white blood cell count (WBC) and platelet counts, among others) are important monitoring tools for assessing treatment and prognosis in HIV/AIDS. Apart from the CD4 count, a full blood count is the commonest pre-treatment investigation done for people living with HIV. Although it is not part of the criteria for initiating therapy nor used by the World Health Organization (WHO) for staging HIV, hematologic abnormalities, indicated by a deranged full blood count, are common manifestations and important prognostic tools of human immunodeficiency virus (HIV) infection and AIDS. 1 In all cases, a specific diagnosis of the cause, severity and mechanism of cytopenia should be sought, because a specific intervention other than the use of antiretroviral drugs may be indicated for its correction. The use of antiretroviral drugs could positively or negatively affect these parameters, depending on the choice of combination used. Although many drugs used for the treatment of HIV-related disorders are myelosuppressive, severe cytopenia is most often related to the use of zidovudine. 2 Hence the need to review these parameters in a group of treatment-naïve HIV-infected patients only cannot be overemphasized.
Anemia in HIV
The diagnosis and treatment of anemia are essential in the medical care of the HIV-infected patient. Anemia affects quality of life by inducing symptoms such as weakness, dyspnoea and tachycardia. 3 Anemia has been shown to be a risk factor for early death in patients with AIDS. 2
The causes of HIV-related anemia are multi-factorial,4–6 anemia may result from the indirect effects of HIV infection, such as adverse reactions to medications, opportunistic infections or neoplasm; nutritional causes such as anorexia or malabsorption; or metabolic disorders associated with HIV. Renal production of erythropoietin is required to stimulate the erythroid bone marrow precursors to proliferate and increase red blood cell (RBC) production. Thus, severe renal insufficiency also contributes to anemia in HIV-infected patients.
HIV may directly affect bone marrow stromal cells, leading to decreased production of RBCs and other bone marrow elements. Although HIV-related anemia is often ultimately attributed to reduced RBC production, other conditions, such as hemolysis or gastrointestinal bleeding, may also occur in these patients. 1 For example, thrombotic thrombocytopenic purpura, an antibody-mediated microangiopathic hemolytic anemia, is seen with increased frequency in HIV-positive patients. 1
Leucopenia in HIV
Leucopenia is also encountered in patients with HIV. Although low leucocyte counts usually reflect the toxicity of therapies for HIV or associated conditions, studies of untreated patients have also shown a high incidence of leucopenia, particularly in patients with more profound immunodeficiency as a consequence of the virus. 7
Thrombocytopenia in HIV
Thrombocytopenia is a possible complication of HIV infection. Its pathogenesis has not yet been established. Possible mechanisms that have been reported are an increased platelet destruction either caused by the nonspecific deposition of circulating immune complexes on platelets or by the presence of specific antiplatelet antibodies, as well as direct infection of megakaryocytes by HIV with a resulting decrease in platelet production. 8
Materials and Methods
This was a cross-sectional study of treatment-naïve HIV-infected clients who enrolled at the HIV clinic of Lagos State University Teaching Hospital (LASUTH) between December 2009 and June 2010. Full blood count and CD4 counts, among others, are free routine pre-requisite and pre-treatment evaluations done for all registered HIV patients at LASUTH. All consenting participants were recruited consecutively into the study. Blood samples were taken after obtaining the institution's research and ethical committee's approval. Participants were asked to fill the structured questionnaires to obtain demographic data, with assistance given if necessary.
Data were analyzed using Statistical Package for Social Science (SPSS) version 16. Descriptive statistics (minimum, maximum, mean and standard deviation) were appropriately applied in the course of analysis. Proportions and percentages were calculated for categorical variables.
Results
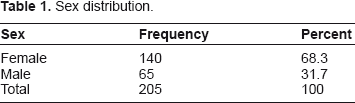
Sex distribution.
Frequency distribution of cytopenia.
Age and hematological parameter distribution.
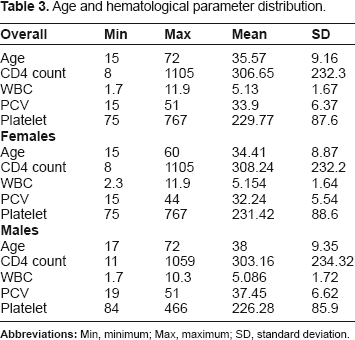
The overall minimum CD4 count was 8 cells/μL, the maximum was 1105 cells/μL and the mean CD4 count was 306.65 ± 232.24 cells/μL. Only 18.5% of the study population had a CD4 count of >500 cells/μL; the majority (27.8%) had a CD4 count of between 100 and 200 cells/μL, 15.1% had a CD4 count between 50 and 100 cells, while 11.7% had a CD4 count less than 50. Ten of sixty-five males (15.38%) and 24 of 140 (females 17.14%) had a CD4 count >500 at registration (Table 3).
The mean age of 34.41 ± 8.87 and 38 ± 9.35 years was obtained for females and males, respectively, with a minimum of 15 and 17, and a maximum of 60 and 72 years for females and males, respectively. The mean PCV was 32.45 ± 5.54% and 37.45 ± 6.62% for females and males, respectively. The minimum PCV recorded was 19% and 15% and the maximum was 51% and 44% for females and males, respectively (Table 3).
The mean WBC was 5.086 ± 1.72 and 5.15 ± 1.64, respectively, for males and females, while the mean platelet counts were 226.28 ± 85.95 and 231.42 ± 88.65 for males and females, respectively. The mean CD4 counts were 303.16 ± 234.32 and 308.24 ± 232.16 cells/μL for males and females, respectively (Table 3).
Only 7 of 65 males (15.38%) and 28 of 140 females (20%) were anemic (ie, PCV < 30%) at pre-treatment evaluation, while 10 of 65 males (15.38%) and 11 of 140 females (7.85%) were leucopenic (ie, total WBC < 4000), and 9 of 65 males (13.8%) and 12 of 140 females (8.57%) were thrombocytopenic (ie, platelet count <150,000) at registration.
Relationship between varying degrees of CD4 count and cytopenia.
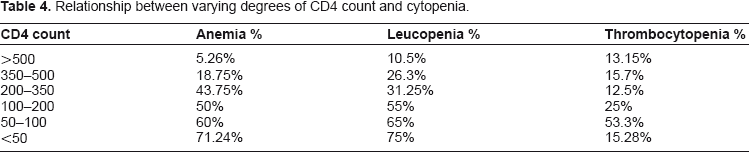
Only 4 of 38 subjects (10.5%) with a CD4 count of >500 cells/μL had leucopenia, 15 of 57 subjects (26.31%) with a CD4 count of 350–500 cells/μL were leucopenic, 10 of 32 (31.25%) subjects with a CD4 count of 200–350 cells/μL were leucopenic and 11 of 20 subjects (55%) with a CD4 of count 100–200 cells/μL were leucopenic.
The study showed that 5 of 38 subjects (13.15%) with a CD4 count of >500 cells/μL were thrombocytopenic, 9 of 57 subjects (15.7%) with a CD4 count of 350–500 cells/μL had thrombocytopenia, 4 of 32 subjects (12.5%) with a CD4 count of 200–350 cells/μL were thrombocytopenic, 5 of 20 (25%) of those with a CD4 count of 100–200 cells/μL were thrombocytopenic, while 8 of 24 subjects (53.3%) with a CD4 count of 50–100 cells/μL were thrombocytopenic and 9 of 57 subjects (15.28%) with a CD4 count of >50 cells/μL were thrombocytopenic (Table 4).
Discussion
This study revealed that 24.2% of the sample population was anemic at registration, which is in agreement with the 18.9% prevalence reported in Uganda 9 but in sharp contrast with the 80% obtained by Erhabor et al 10 in Port-Harcourt, Nigeria, amongst untreated HIV patients. This study confirms that anemia is directly related to the degree of immunosupression, as reported by Zon and Groopman, 7 Spivak et al 11 and a multicenter AIDS cohort study: 12 the lower the CD4 count, the lower the PCV.
A prevalence of 26.8% leucopenia was reported in this study compared to the 10% reported by Erhabor et al. 10 It is also confirmed in this study that a high prevalence of leucopenia is more associated with profound immunodeficiency, as was reported by Zon and Groopman, 7 Spivak et al 11 and the multicenter AIDS control cohort study. 12 A prevalence of 16.1% thrombocytopenia was obtained in this study, similar to the 10% reported by Erhabor et al. 10 The degree of thrombocytopenia is also directly related to the degree of immunosupression, as confirmed by Jost et al 8 and the multicenter AIDS control cohort study. 12
This study revealed that over half (54.6%) of newly registered HIV patients will require antiretroviral drugs almost immediately because their CD4 count of <200 cells/μL at enrollment will qualify them automatically for highly active antiretroviral drug, irrespective of symptoms, according to WHO criteria for initiating antiretroviral therapy.
This study reported a mean CD4 count of 308 cells/μL for females that was higher than the mean of 303 cells/μL for males, which is contrary to the study of Omoti et al 13 who reported a slightly higher CD4 count for males of 195 cells/μL versus 180 cells/μL for females. Oladepo et al 14 established a reference value for CD4 in healthy Nigerian adults of 365 to 1571 cells/μL, with a mean CD4 count of 847 cells/μL, similar to the mean value of 828 cells/μl reported by Aina et al 15 in an earlier study in Nigeria. Females were found to have significantly higher values of absolute CD4 counts in Oladepo et al's study, contrary to the earlier limited study by Aina et al. This observation of higher CD4 count in females has also been reported in several other countries among Nigerians 16 Ugandans 17 and Ethiopians. 18 A sex hormone effect is one possible explanation for the reported difference in CD4 counts between genders that has been suggested. 18
Conclusion
About one-fifth of HIV treatment-naïve patients were cytopenic at enrollment and the degree of cytopenia was directly related to the degree of immunosupression. Hence it is necessary to investigate the various causes of cytopenia in these patients, with a view towards administering specific interventions. Half of the HIV patients would require antiretroviral drugs almost immediately because of their low CD4 count. The study also found a slightly higher CD4 count in females compared to males.
Footnotes
Acknowledgement
The Institute of Human Virology, Nigeria, provided registration, laboratory investigations and treatment free of charge to all registered HIV patients participating in this study.
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.