
Abstract
Nitric oxide (NO) is highly reactive, produced in endothelial cells by endothelial NO synthase (eNOS) and has been implicated in sickle cell pathophysiology. We evaluated the distribution of functionally significant eNOS variants (the T786C variant in the promoter region, the Glu298Asp variant in exon 7, and the variable number of tandem repeats (VNTR) in intron 4) in Africans, African Americans and Caucasians. The C-786 variant was more common in Caucasians than in Africans and African Americans. Consistent with other findings, the Asp-298 variant had the highest frequency in Caucasians followed by African Americans, but was completely absent in Africans. The very rare intron 4 allele, eNOS 4c, was found in some Africans and African Americans, but not in Caucasians. eNOS 4d allele was present in 2 Africans. These findings suggest a consistent and widespread genomic diversity in the distribution of eNOS variants in Africans, comparative to African Americans and Caucasians.
Introduction
Nitric oxide is a diffusible molecule synthesized by three isoforms of the nitric oxide synthase (NOS) eg, constitutive neuronal NOS, inducible NOS and endothelial NOS. Endothelial (e) NOS, derived from vascular endothelium, is the most dominant form of these isoforms, 1 and other sources such as cardiac myocytes, blood platelets and the brain 2 which are very crucial to maintaining nitric oxide production. 3 NO plays a pivotal role in the regulation of cardiovascular homeostasis. It is highly reactive, it facilitates maintenance of basal vasodilator tone, it inhibits platelet aggregation and it attenuates leukocyte adhesion to the endothelium. 4 Deficiency in NO production or activity directly affects cardiac dysfunction and is related to the pathogenesis of coronary spasms.5,6 In addition, several eNOS polymorphisms have been found. Three of these are shown to be associated with disease pathophysiology. These are located in the promoter region (T-786C), exon 7 (Glu298Asp), and a variable number of tandem repeats (VNTR) in intron 4. Published reports have suggested the involvement of eNOS polymorphisms in the pathogenesis of sickle cell complications such as acute chest syndrome (ACS) and painful vaso-occlusive crises.7–10 eNOS VNTR has been associated with mean plasma nitric oxide level, while the eNOS C-786 mutant reduces eNOS gene promoter activity and is a genetic risk factor for ACS in adult female sickle cell anemia patients.10,11
Considering the diversity of disease pathophysiology in sickle cell disease and the wide swath of differences in clinical presentation among African and African American patients, it might be necessary to determine whether interethnic diversity of eNOS polymorphisms plays any role in this diversity. Previous population studies have shown that there is marked interethnic difference in the distribution of eNOS polymorphisms between Caucasians and African-Americans 12 with a similar finding reported between black and white Brazilians 13 and white, black and mixed populations from Colombia. 14 Interestingly, an Italian group 15 reported a novel allele of the eNOS gene in an Italian population that had not been previously reported. These findings may explain the ethnic differences in cardiovascular outcome, response to and bioavailability of certain medications, as well as nitric oxide bioavailability. Additionally, polymorphisms that alter eNOS activity or its regulation are important for understanding how perturbations of red blood cell (RBC) membranes are likely to affect blood flow in the microcirculation and NO bioavailability, particularly in sickle cell disease, for which patients might need multiple transfusions. Investigating the role that interethnic variability of eNOS polymorphisms plays within and between groups is therefore highly imperative.
Since previous interethnic studies have been done with mixed populations, or those for which genomic purity is unknown, assaying a genetically pure and homogeneous population alongside others before reaching critical conclusions is imperative. In this study, we examined the distribution, haplotype and diplotype frequency of three endothelial nitric oxide synthase polymorphic forms, shown to have clinically relevant functions in well-defined population groups-Caucasians and African Americans recruited from the United States, and native Africans recruited from Mali. This is the first report examining eNOS polymorphic diversity in an African population and should be seen as a critical first step for examination of potential ethnic differences in clinical presentation. This study is highly imperative because of its capacity to decipher certain clinical differences observed among African Americans as compared to native Africans.
Methods
Subject characterization
Subjects recruited for this study gave informed consent and approval before participating. A total of 189 individuals from the Centre National de Transfusion Sanguine (CNTS) and Centre de Recherche et de Lutte contre la Drepanocytose (CRLD), Mali were recruited. Additionally, 499 de-identified and unlinked African American DNA samples from blood donors were obtained from LifeShare Blood Centers, Shreveport LA. This donor population is representative of the global blood donor population. 165 healthy Caucasians, recruited from the northeastern United States, were also included. This project was reviewed and approved by the Institutional Review Board of the Rochester Institute of Technology.
Genomic DNA samples
Following subject recruitment and informed consent, 5 mL of blood was drawn into EDTA tubes. Well-characterized genomic DNA samples were extracted with the Qiagen DNA Blood Mini kit (Qiagen, Carlsbad CA), according to manufacturer's instruction. DNA samples were stored at –20 °C until they were analyzed. All polymerase chain reaction (PCR) genotyping and restriction digestion were conducted anonymously, with 50% of samples subjected to repeat PCR and genotyping for quality control purposes.
eNOS genotyping
The variable number of tandem repeats (VNTR) polymorphism in intron 4
PCR amplifications of genomic DNA samples for polymorphic VNTR in intron 4 were performed with standard protocols 14 and previously published primers. 15 Primer sets: 5′-CTATGGTAGTGCCTTGGCTGGAGG-3′ (forward) and 5′-ACCGCCCAGGGAACTCCGCT-3′ (reverse) were used for PCR amplification, with conditions altered to 25 μL final volume and amplified using the Lucigen EconoTaq Plus Green 2X Master Mix PCR system (Lucigen Corporation, Middleton WI). Final reaction mixtures contained 0.1 units/μL of EconoTaq DNA Polymerase, reaction buffer (pH 9.0), 400 μM dATP, 400 μM dGTP, 400 μM dCTP, 400 μM dTTP, 3 mM MgCl2, 1 μM forward and reverse primers and a proprietary mix of PCR enhancer/stabilizer and blue and yellow tracking dyes (Lucigen Corporation, Middleton WI). We used 1 μL of genomic DNA template for primary PCR reactions. Post-amplification, 10 μL of the PCR product was evaluated on 2% ethidium bromide stained agarose gels, visualized and photographed. Product size was estimated with 5 μL TriDye 100 bp DNA ladder (New England Biolabs, Boston MA) and product size analysis was carried out with the Doc-It LS Image Analysis Software (UVP Life Sciences, Upland CA). We included negative controls, without DNA template, for confirmation purposes. The number of fragments of appropriate size obtained were compared for each sample, counted and combined across samples. PCR cycling parameters followed published protocol. 14 Fragments of 169, 196, 223 and 142 bp corresponding to eNOS alleles 4a, 4b, 4c and 4d, defined the presence of 4, 5, 6 and 327 bp repeats respectively.
The Glu298Asp polymorphism in exon 7
This polymorphism was genotyped by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP), with the primer pairs: 5′-AAG GCA GGA GAC AGT GGA TGG A-3′ and 5′-CCC AGT CAA TCC CTT TGG TGC TCA-3′. 13 PCR was performed for 35 cycles in a volume of 25 | L. The PCR mixtures were heated to 94 °C for 4 min for denaturation and underwent 35 cycles at 94 °C for 30 s for denaturation, 65 °C for 30 s for annealing, and 72 °C for 1 min for extension. Finally, extension was conducted at 72 °C for 5 min. Amplified PCR samples of 258 bp band size were subjected to restriction digestion with 2U BanII restriction enzyme for 6 hours at 37 °C. This enzyme cleaves the PCR product into fragments of 163 and 85 bp fragments (wild type) or no digestion (variant allele). Digested products were evaluated as described above, while size analysis was carried out with the Doc-It LS Image Analysis Software (UVP Life Sciences, Upland CA). Negative control reactions, without DNA template, were also included for confirmation.
The T7860 polymorphism in the 5′-flanking region
To genotype for the T786C (rs2070744) variant in the 5′-flanking region, we applied a similar PCR-RFLP procedure as described above, except for different primer pairs and different restriction enzymes. Primer pairs T786C-F (5′-TGGAGAGTGCTGGTGTACCCCA-3′λ) and T786C-R (5′-GCCTCCACCCCCACCCTGTC-3′) served for DNA amplification. 14 Final reaction mixtures contained 0.1 units/μL of EconoTaq DNA Polymerase, as described for intron 4 reaction above. 1 μL of genomic DNA template was used for amplification, while 10 μL of the PCR product was evaluated post-amplification. PCR products with the appropriate band size were digested for 1 hour on an Eppendorf gradient Mastercycler with 1 μL of Msp I restriction enzyme at 37 °C, producing fragments of 140 and 40 base pairs for the wild-type (TT) allele, or 90, 50, and 40 base pairs for polymorphic variants (CC). Sizes of PCR products and restriction products were estimated with a TriDye 100 bp DNA ladder (New England Biolabs, Boston MA) and size analysis carried out with the Doc-It LS Image Analysis Software (UVP Life Sciences, Upland CA).
Statistical analysis
Of the four alleles in intron 4, the 4c and 4d alleles are rare; for analysis purposes, they were pooled with the 4a variant as reported elsewhere. 13 Thus, each of the three variants had two alleles. Genotype and allele frequencies at each variant were determined with a PERL script (http://www.perl.org). Differences in genotype and allele frequencies between populations were assessed using chi-square tests. Haplotype frequencies were estimated and tested for interethnic differences with the EH program (http://linkage.rockefeller.edu/ott/eh.htm). 16,17 Individuals missing one or more genotypes were disregarded for analysis purposes (7 Africans, 2 African Americans, and 1 Caucasian). Linkage disequilibrium (LD) among variants in a given population was assessed in the EH program by likelihood ratio chi-square tests, and so were differences in haplotype frequencies among the three populations.
Diplotypes (genotype patterns) are analogous to haplotypes, except that instead of one allele per variant, they are sets of one genotype per variant. Diplotypes 18 have an advantage over haplotypes in that they can unequivocally be identified in each individual (barring missing genotypes). Also, no Hardy Weinberg Equilibrium (HWE) is assumed in the estimation of their frequencies, as is the case for some aspects of haplotype frequency estimation. Diplotype frequencies were estimated in a spreadsheet and their between-population differences were assessed using a chi-square test. For this test, rare diplotypes (less than one expected diplotype in at least one population) were combined with neighboring diplotypes.
Results
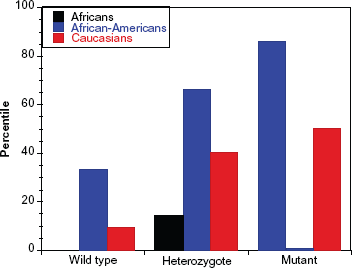
We have examined the ethnogenomic diversity of three endothelial nitric oxide synthase (eNOS) polymorphisms that have been reported to have significant clinical relevance in three well-defined and clearly distinct population groups (165 Caucasians from New Jersey, 499 African Americans from Louisiana and 189 Africans from Mali). For additional emphasis, we deciphered the significance of genomic homogeneity/heterogeneity on the interplay between African Americans versus native Africans or African Americans versus Caucasians. eNOS polymorphic groups analyzed include a T/C substitution in the 5′-flanking region near promoter at –786, a G/T substitution at position 894 in exon 7, and a 27-base pair variable number of tandem repeats (VNTR) in intron 4. We found significant interethnic disparity in the genomic distribution of these polymorphic types between the various population groups. Table 1 shows the genotypic frequency of these polymorphisms in the study populations. On the other hand, Table 2 depicts the allelic diversity of these polymorphic groups in the same study population. Figures 1–3 shows the percentile distribution of eNOS polymorphic forms, Glu298Asp, intron 4 and T786C genotypes in Africans, African Americans and Caucasians respectively (black bars-Africans; blue bars-African Americans; red bars-Caucasians).
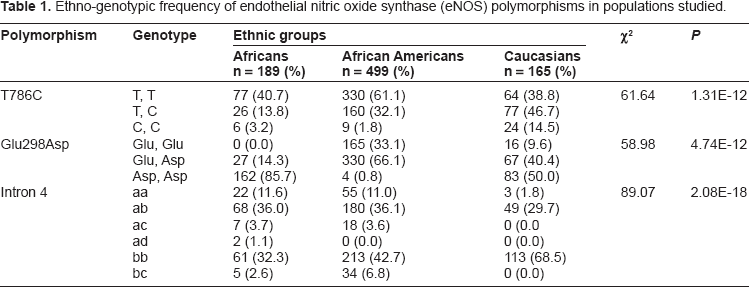
Ethno-genotypic frequency of endothelial nitric oxide synthase (eNOS) polymorphisms in populations studied.
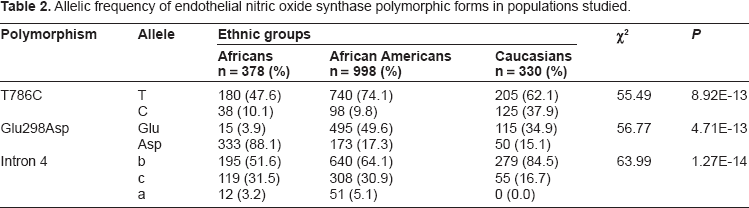
Allelic frequency of endothelial nitric oxide synthase polymorphic forms in populations studied.
Percentile distribution of endothelial nitric oxide synthase, Glu298Asp, polymorphisms in Caucasian, African American and native African populations.
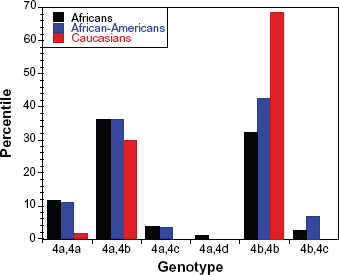
Percentile distribution of intron 4 polymorphisms in Caucasian, African American and native African populations.
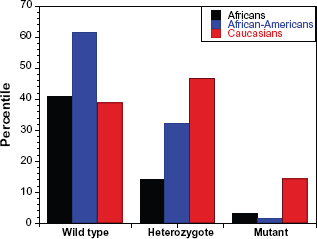
Percentile distribution of endothelial nitric oxide synthase, T786C polymorphisms in Caucasian, African American and native African populations.
Examining the genotypic diversity of T786C polymorphisms in the promoter region, the wild type group T-786 had the highest frequency in all populations studied (40.7%, 61.1% and 38.8% in Africans, African Americans and Caucasians respectively). The C-786 mutant group, however, was more common in Caucasians (14.5%) compared to Africans or African Americans (3.2% and 1.8% respectively) and this difference was highly significant (χ 2 = 61.64; P = 1.312 × 10–12). In addition, the Asp-298 variant in exon 7 had the highest frequency in Caucasians (9.6%) followed by African Americans (0.8%), whereas it was surprisingly absent among Africans (0.0%). This distribution also displayed a very high significance between the population groups (χ 2 = 58.98; P = 4.74 × 10–12). As for intron 4 polymorphism, we analyzed the distribution of wild-type alleles 4b and 4a, corresponding to five and four 27-base pair repeats, which are the most represented and well-detected, as well as the very rare variants 4c and 4d corresponding to six and three 27-base pair repeats respectively. We found eNOS 4c alleles in 12 (6.3%) Africans, and 52 (10.4%) African Americans, but found none in Caucasians. Additionally, we found eNOS 4d alleles in 2 (1.1%) Africans. Genotypic frequencies at each variant and within each population seem compatible with the Hardy-Weinberg equilibrium (HWE), except when analyzed for ethnic comparisons among African Americans (too many observed heterozygotes, too few of either of the homozygotes). These deviations from HWE presumably reflect effects of admixture.
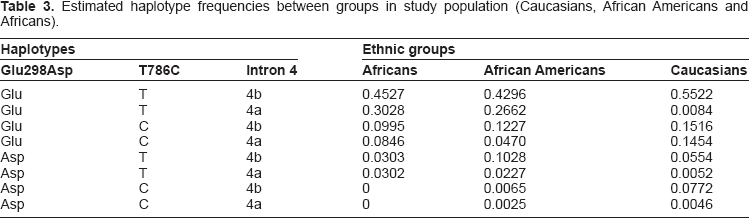
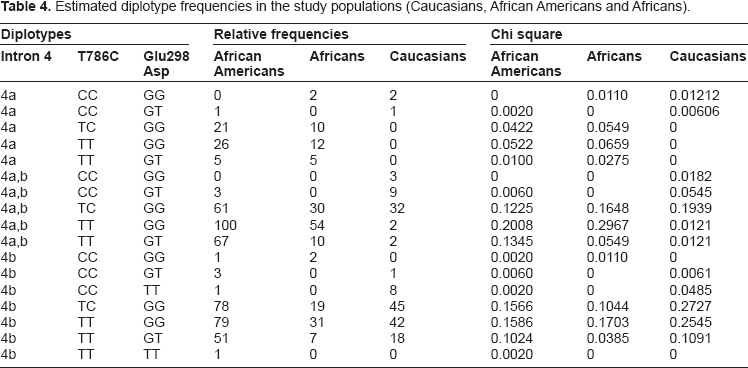
Relative frequencies for the haplotypes between groups is shown in Table 3. In addition to haplotype frequency, diplotype frequencies were estimated and their differences between populations were assessed (Table 4). The most commonly-encountered haplotype for all ethnicities combines the wild-type homozygotes for all three polymorphisms (45%, 43% and 55% respectively for Africans, African Americans and Caucasians). The second most common haplotype for Africans (30%) and African Americans (26%) includes the variant 4a in intron 4 and the wild-type polymorphic forms for T786C and Glu298Asp, which is almost absent in Caucasians (0.8%). In Caucasians, we found one haplotype to be significantly common-estimated haplotype frequency of ~15%. This is C-786 in the promoter region, and the wild-type homozygote forms for the other two polymorphisms (Glu298 and intron 4a, and 4b). In fact, analyzing the Caucasian group alone reveals that the C-786 haplotype is the most common in this group (estimated frequency of 27%) compared to ~10% for other ethnic groups.
Estimated haplotype frequencies between groups in study population (Caucasians, African Americans and Africans).
Estimated diplotype frequencies in the study populations (Caucasians, African Americans and Africans).
Genotype frequencies at each variant and in each population were compatible with Hardy-Weinberg equilibrium (HWE) except for the T786C (P = 0.0456) and Glu298Asp polymorphisms (P = 2.13 × 10–8) in African Americans (due to too many observed heterozygotes, and too few of either of the homozygotes). These deviations from HWE presumably reflect effects of admixture.
Within each population, the three variants exhibited significant linkage disequilibrium (LD): P = 0.0432 for Africans, P = 0.0003 for African Americans, and P = 1.74 × 10–13 for Caucasians. This cline of relatively low LD in Africa and high LD in Westerners nicely demonstrates the out-of-Africa hypothesis. Due to these differences in LD and to differences in allele frequencies among populations, haplotype frequencies turned out to be significantly different in the three populations (χ 2 = 221.08, 12 df, P = 1.42 × 10–40).
Discussion
We present results from our study examining the ethnogenomic diversity of endothelial nitric oxide synthase (eNOS) polymorphic forms that have been reported to have significant clinical relevance. We analyzed DNA samples from three clearly distinct and well-defined ethnic groups. These included Africans from Mali, African Americans and Caucasians from United States. To our understanding, this is the first report ever to examine a purely homogeneous African population for comparative purposes. Previous studies have examined Caucasians versus African Americans in the United States, 12 black and white Brazilians 13 and white, black and mixed populations from Colombia. 14 This present report, however, is a first step toward deciphering the role of a homogeneous African population sans admixture in data analysis and eNOS polymorphism conclusions.
Ethnogenotypic diversity studies of endothelial nitric oxide synthase (eNOS) polymorphisms has become imperative because of the possible clinical and pathophysiological implications of certain diseases, as well as potential deconvolution of ethnic-based responses and/or observations to certain chemotherapeutic agents. Tanus-Santos et al 12 have reported on the potential possibility that these polymorphisms may predispose African Americans in the United States to coronary artery disease and hypertension.12,19,20 In addition, the ethnic distribution of these polymorphisms and pathophysiological implications might carry a geographical import, considering results from a Japanese cohort. 21 In our report, we found very extensive and clearly marked differences in the interethnic distribution and haplotype frequency of these eNOS variants, within and between the populations analyzed. This information adds to the growing consensus that eNOS variants play more significant roles than previously thought in disease pathophysiology.22–28
A closer examination of the T786C polymorphism (located in the promoter region) revealed that the homozygote CC variant was commonly encountered in the Caucasian population (14.5%), compared to its frequency among “blacks” (3.2% and 1.8% in Africans and African Americans respectively), and further confirms observations made elsewhere.12,14 However, this observation clearly contrasts the report in a Brazilian “white” cohort. 13 We can thereby postulate that the differing frequency of this variant is, either individually or in combination, population and geography-dependent.12–14,35 Particularly in Brazil, individual contributions to biogeographical ancestry varies widely. However, most individuals, irrespective of demographic classification, phenotypic coloration or generation, possess significant degrees of genetic admixture of European and African ancestry. A few others display Amerindian heritage, which may explain the difference in genotypic frequency. This variant is clearly represented in the Caucasian gene pool but not others, and deciphering its role in disease predisposition or pharmacokinetic potential require further studies.
The intron 4 results in our study are very significant; this is the first report, to our knowledge, that has examined intron 4 in an African population. This polymorphism has been found to be positively associated with varying nitrate levels in plasma, with potential implications for various cardiovascular and pharmacologic outcomes. Reports abound on the distribution of the common intron 4 alleles; eNOS4a and eNOS4b, commonly encountered with diverse distribution, while the rarer eNOS4c and eNOS4d has been defined in very few instances. These alleles have been studied in different populations and under different conditions to ascertain their possible physiologic or disease implication. Populations studied include healthy controls, as well as patients with acute coronary syndromes, venous thromboembolisms, myocardial infarction, preeclampsia, and Alzheimer's disease.10,36–42 Our results for the eNOS4d allele in the African population reveal the need for an extensive genetic association study to ascertain a potential role for this allele in that population. In a recent report, it has been shown that red cell eNOS expression and activity are both lower in patients with coronary artery disease than age-matched healthy individuals, and this activity is correlated with the degree of endothelial dysfunction. 43 The authors concluded that human RBCs constitutively produce nitric oxide under normoxic conditions via an active eNOS isoform, and this activity is compromised in patients with coronary artery disease. How this observation plays in ethnic-based disease pathophysiology or sickle cell crisis will be a necessary next step.
The Glu298Asp polymorphism was also analyzed in all population groups, with its distribution following a Hardy Weinberg Equilibrium (HWE). Consistent with other studies, we found the 298 Asp variant to occur at ~1% in African Americans and to be completely absent in Africans. We do not contend that this would be the outcome had African Americans from a different region or Africans from a different part of the continent had been studied. This is due to the admixture among African Americans34,44,45 and geography 46 in the African population. African Americans in this study were recruited from the state of Louisiana based on knowledge of an ancestry that can be traced to the slave trade era,47–50 which might potentially contribute to this observation. Published reports 51 have shown that African American ancestry is closely traceable to the Afroasiatic and Nilo-Saharan speaking populations of coastal West Africa, but not the Niger-Kordofanian (Dogon from Mali). Further studies examining this polymorphism in representative population of African Americans (recruited from the Northeast or Mid-Atlantic United States) and Africans (recruited from coastal West Africa) vis-à-vis region- or disease-specific selection pressures is highly imperative and urgently advocated.
In conclusion, we found that the three variants under study exhibited significant linkage disequilibrium (LD) in the various population groups, with the highest values in Caucasians and the lowest values among Africans. This cline of relatively low LD in Africa and high LD in Westerners nicely demonstrates the out-of-Africa hypothesis. As has been reported previously, 52 increasing linkage disequilibrium is observed with increasing geographical distance from Africa. 53 This hypothesis states that all modern humans stem from a single group of Homo sapiens who left Africa 2,000 generations ago, spreading all over Eurasia, and that they replaced other early humans rather than interbreeding with them. The cline of relatively low LD in Africa and high LD in Westerners observed in our data nicely demonstrates this fact. In addition, compared to other reports, we present an analysis of a much bigger sample size that is statistically justifiable. 54 Due to these differences in LD and to differences in allele frequencies among populations, haplotype frequencies were significantly different in the three populations, confirming our hypothesis. Our report is a foundational study to elucidate the role of these polymorphisms in sickle cell disease, applicable to the study of diversity in clinical presentation and disease outcome in Africans versus African-Americans. This is particularly imperative considering the significant admixture and richness of the African American gene pool.29–34 The next step is to extrapolate how each of these polymorphisms regulate clinical (patho)physiology in a strict African and African American sickle cell population.
Funding Sources
Funding for this project was provided by an Accelerated Research Funding Award, Sponsored Research Services, Rochester Institute of Technology (BNT).
Author Contributions
Conceived and designed the experiments: BNT, AG, DAD. Analyzed the data: BNT, TJT, LY, JO. Wrote the first draft of the manuscript: BNT, TJT. Contributed to the writing of the manuscript: JO. Agree with manuscript results and conclusions: BNT, TJT, LY, AG, DAD, JO. Jointly developed the structure and arguments for the paper: BNT, JO. Made critical revisions and approved final version: BNT, TJT, AG, DAD, JO. All authors reviewed and approved of the final manuscript.
Competing Interests
The authors declare that they have no competing interests.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgements
We are grateful to Joann Moulds of LifeShare Blood Center, who provided the de-identified DNA samples, Mounirou Baby and Londyn Cullifer for technical assistance.