
Abstract
The incidence of malignant melanoma in the developed world is continuously increasing. We conducted a case–control study in order to evaluate the association between each of the four estrogen receptor alpha polymorphisms (ESR1 single-nucleotide polymorphisms [SNPs] +2464C/T, –4576A/C, +1619A/G, and +6362C/T) and malignant melanoma susceptibility and disease course. The study population consisted of 205 Caucasian patients who were diagnosed as having malignant melanoma and 208 healthy Caucasian controls. Through DNA genotyping, we identified a SNP-dependent malignant melanoma susceptibility as well as a SNP-dependent effect on the course of disease and response to therapy.
Introduction
A positive correlation between the incidence of malignant melanoma and pregnancy has frequently been discussed. However, to date no such linkage has been demonstrated with regard to incidence, disease progression, or patient survival in association with melanoma. On the other hand, pregnant women show tumors of greater thickness and reveal a still unexplained shorter disease-free interval.1–3 Therefore, the question as to a potential association between hormonal status and melanoma remains still unanswered. The estrogen receptor (ER) may be found as a homodimer (ERα and ERβ). ERs are nuclear receptor proteins containing an estrogen-binding domain and a DNA-binding domain. 4 ERβ expression levels have been reported to correlate with the malignant tumor microenvironment of malignant melanoma and increasing Breslow depth. 5 ERα, on the other hand, seems to have no such linkage so far. 5
The aim of this study was to assess potential associations between ERα with malignant melanoma susceptibility and clinical parameters such as disease progression or response to treatment and others.
Materials and Methods
Study population
The study group comprised a total of 205 patients who were diagnosed as having malignant melanoma and registered at the interdisciplinary dermatology cancer center at the University of Regensburg between 1987 and 2008. The age distribution of the patients at initial diagnosis has an age peak in the group of 60- to 90-year-old patients (gender distribution: 100 females, 105 males) (Fig. 1). The control group consisted of 208 healthy young women and men as controls (gender distribution: 111 females, 97 males; about half female, half male to avoid gender differences), all younger than 30 years of age. Unfortunately polymerase chain reaction (PCR) was not feasible on all DNA samples, causing differences in the number of cases and controls. The study protocol was approved by the ethics committee of the ärztekammer des Saarlandes, Saarbrücken, and the study was conducted in accordance with the principles of the Declaration of Helsinki. Patients gave their written, informed consent to participate in the studies for which their blood samples were initially collected.
DNA extraction and genotyping
Blood samples were collected for DNA extraction and for subsequent genotyping from patients at first presentation to the clinic and from controls. DNA was extracted from peripheral blood mononuclear cells using the NucleoSpin-Blood-Kit (Macherey-Nagel) in accordance with the manufacturer's instructions. The observation period was from the time of initial diagnosis up to at least three years after diagnosis or death. Main attention was drawn to patient age at initial diagnosis and to disease progression and disease-free survival. They were split into two groups depending on the presence or absence of a disease relapse and were subgrouped depending on the temporal occurrence of the relapse. We checked their need for chemotherapy and the context (first diagnosis or relapse) in which chemotherapy was given. Patients were treated in accordance with the current melanoma treatment guidelines. Adjuvant chemotherapy was only used in the palliative setting (TNM stage IV). 6 In all patients, treatment regimens included dacarbazine as a chemotherapeutic agent. To focus on the duration of the disease, patients were split into four groups (less than one year, one to three years, and more than three years after first diagnosis and patient files lacking data as to duration).

Age distribution of the patients at initial diagnosis.
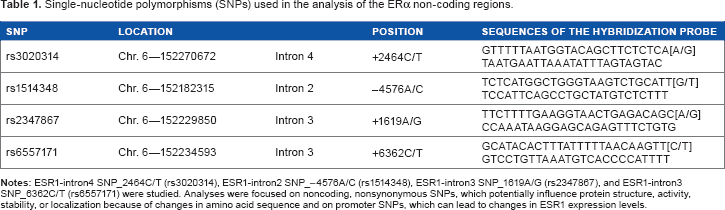
Four single-nucleotide polymorphisms (SNPs), which are located within ERα intronic regions, were assessed7–9 (Table 1), and PCR amplifications were carried out in accordance with the supplier's instructions: a single initial heating step at 95°C for 10 minutes preceded 45 cycles of denaturation at 92°C for 15 seconds, which were then followed by annealing and elongation at 60°C for one minute. For genotyping, the CFX 96™ real-time PCR Detection Systems (Bio-Rad) and/or StepOnePlus™ real-time PCR System (Applied Biosystems) with the related software were used. Allelic discrimination plots and the quantification analyses allowed to allocate SNPs to the wild-type allele or the variant allele.
Single-nucleotide polymorphisms (SNPs) used in the analysis of the ERα non-coding regions.
Statistical analysis
We analyzed the results for each SNP and checked the conformance with the Hardy–Weinberg equilibrium (HWE) using the χ 2 -test. Statistical analyses were performed with the SPSS software (IBM-SPSS-statistics 19). χ 2 -test was used for comparison of genotype frequencies for cases and controls, for comparison of the age by initial diagnosis, disease duration, and progression, and chemotherapy for the different genotype groups. In cases the χ 2 -test was invalid (expected values were <5), the Fisher's exact test for statistical significance was used.
Results
Disease progression of malignant melanoma in association with genetic frequencies is presented in Table 2, just as real-time PCR data, correlated with clinical parameters. There was no evidence of deviation of the genotype frequencies from HWE in patients and controls, with the exception of the control group for SNP–-2464C/T Therefore, this group was excluded from further analyses.
Disease progression in the context of ESR1 genetic polymorphisms.

Real-time PCR data from patient samples were correlated with clinical parameters as shown in Table 2. Association of malignant melanoma with the genotype of two of four intronic polymorphisms was evaluated. Figure 2A-D shows differences between the frequencies depending on their locations within the ERα gene in cases and controls.
Figure 2 shows that the ERα location on the infrequent allele seems to have a protective role as to malignant melanoma susceptibility. An association between patients and a heterozygote location of ERα is evident. For the comparison of cases and controls with the heterozygote location on SNP–-2464C/T, a tendency of more diseased people was seen. Since this was not in accordance with the HWE, this observation was not examined any further. This tendency increases further for associations with the heterozygote location of SNP–-–4576A/C with significantly more heterozygotic patients. By contrast, the prevalence of SNP_–4576A/C on the wild-type allele appears to have a protective effect as to the acquisition of malignant melanoma. The frequency of SNP_–4576A/C lying on the variant allele seems to have no influence of the incidence of melanoma. Cases carried significantly more often the +1619A/G wild-type allele than controls and, vice versa, controls carried significantly more often the +1619A/G and +6362C/T variant alleles.

SNP frequencies in patients and controls.
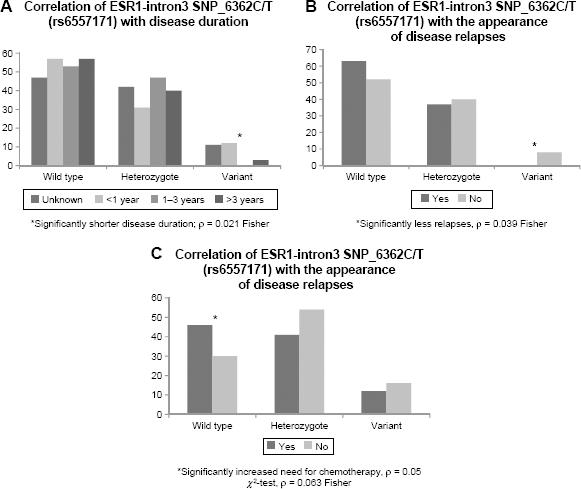
We failed to identify a correlation for any of the SNPs and patient age at the time of diagnosis or the appearance of a disease relapse within one year after first diagnosis. However, the correlation of the SNPs and the relapse rate, the duration of the disease, and the need of chemotherapy are shown in Figure 3. Significantly more patients had a disease course that was shorter than one year when the SNP_6362C/T was located on the variant allele, while if SNP_6362C/T was located on the wild-type allele or heterozygote, disease duration was almost the same and no differences were found. Patients with SNP_6362C/T lying on the rare allele had significantly less relapses. In fact, not one patient in our study with SNP_6362C/T on the variant allele (12 cases) had a disease relapse. Patients with SNP_–4576A/C on the wild-type allele needed significantly more chemotherapy in total when compared to patients with SNP_–4576A/C on the variant allele, even though the risk of acquiring the disease decreases with this SNP lying on the wild-type allele (Fig. 2B).
SNP frequencies in correlation with malignant melanoma.
Discussion
Malignant melanoma is the type of cancer with the most rapidly increasing incidence rates worldwide. A connection between steroid hormones and melanoma has frequently been discussed. Numerous studies investigating the role of estrogen in association with malignant melanoma have been performed earlier. 5 ,10–14 Pregnancy and oral contraception and hormonal replacement therapy were suspected to increase melanoma risk and poor disease prognosis, but none of them appear to affect five-year survival rates. 14 However, a meta-analysis from Gandini et al 10 found a statistically increased risk by about 10% to acquire the disease through a 10-year increase in age at first pregnancy and lower risk for women with more than one child. Furthermore, population studies have detected a survival advantage for women when compared to male survivors. 15 Therefore, the assumption of estrogen promoting malignant melanoma still persists. Also, ERβ expression levels have been reported to correlate with the malignant tumor microenvironment of melanocytes and increasing Breslow depth. 5 ERα, on the other hand, did not show an obvious role for estrogen influencing the appearance or progression of malignant melanocytic lesions in the same study. 5 But how malignant melanoma is affected by estrogen still remains unclear. In our study, we investigated the probability of inherited susceptibility to melanoma arising from different genomic ERα SNPs (Table 2). Therefore, this study gives us the opportunity to test for genetic risk constellations as to malignant melanoma disease susceptibility and potential disease course already at the time of initial diagnosis. Since this information, which is certainly interesting from an academic point of view, helps us to further understand the pathogenesis of malignant melanoma, it does not affect disease outcome for the patient and it is certainly an ethical issue whether patients with a dismal prognosis once they have acquired malignant melanoma should be tested and potentially be identified to belong to a risk group that is being associated with an even worse prognosis predicting an average survival of only few weeks or months.
Author Contributions
Conceived and designed the experiments: JK. Analyzed the data: TV, JK, HG. Wrote the first draft of the manuscript: HG. Contributed to the writing of the manuscript: HG, UM. Agree with manuscript results and conclusions: UM. Jointly developed the structure and arguments for the paper: UM, HG. Made critical revisions and approved final version: UM. All authors reviewed and approved of the final manuscript.