
Abstract
Patient navigation is an internationally utilized, culturally grounded, and multifaceted strategy to optimize patients' interface with the health-care team and system. The DuPage County Patient Navigation Collaborative (DPNC) is a campus-community partnership designed to improve access to care among uninsured breast and cervical cancer patients in DuPage County, IL. Importantly, the DPNC connects community-based social service delivery with the patient-centered medical home to achieve a
Introduction
The World Health Organization's Alta Alma Declaration of 1978 underscored the need for community health advisors to deliver primary health care to community members.1,2 This movement has historically been led by
Perhaps more so than patient navigation, the patient-centered medical home (PCMH) has been promoted as a central facet of health-care system redesign and a path toward health equity.5,6 Broadly, a medical home refers to accessible, continuous, and comprehensive clinician-directed care teams integrating all domains of the health-care system.5,7 However, compared with other developed countries, USA underperforms with respect to having accessible, efficient medical homes.
8
Despite its promise to transform care, the PCMH model is limited by its narrow focus on the course of disease in the clinical setting, with less emphasis on other factors that may exacerbate care fragmentation, such as social determinants.
6
An expanded PCMH model–-one that considers the social and environmental context in which patients seek care–-may be needed to achieve an effective, efficient, equitable, and patient-centered delivery model.
6
In this context, patient navigators have the potential to connect community-based social service delivery with the PCMH to achieve a
In this study, we discuss the DuPage County Patient Navigation Collaborative (DPNC), a campus-community partnership located in DuPage County, IL, through which lay health navigators helped patients to resolve multiple barriers to care and offered culturally competent support and guidance to women with an abnormal breast or cervical cancer screening test. This project was supported by a five-year National Institutes of Health community-based participatory research grant, with an emphasis on improving timeliness of care among the county's at-risk, uninsured, and immigrant population. A detailed overview of the DPNC collaboration, including the strategies that contributed to DPNC success, has been previously described within the literature.9,10
DuPage County, IL, which is adjacent to Chicago's Cook County, has rapidly become more diverse over the last two decades. Latinos, for example, account for 14% of the population, an increase of 253% over the last two decades, while the percentage of non-Hispanic Whites has declined by 9.6%. 11 DuPage has also experienced exponential increases in health and income disparities over the last decade. As a suburban area, DuPage lacks the well-established health-care safety nets commonly found within urban metropolises. Accordingly, DuPage has noted significant health disparities, particularly among racial and ethnic minorities. Between 2004 and 2007, 63% versus 71% of adult women in DuPage County and Cook County, respectively, reported receiving a Pap test within the past three years. 12 Furthermore, between 2000 and 2009, the percentage of DuPage County residents living below the federal poverty line rose by 182%. 13 To address these disparities, the DPNC campus-community partnership between Northwestern University and Access DuPage was forged. Access DuPage, which represents a collaboration of hospitals, physicians, local government, human service agencies, and community groups, is a not-for-profit organization that collaborates with more than 1000 health-care providers and organizations to create primary care homes for uninsured residents, with care provided by federally qualified health centers, volunteer private physicians, and a volunteer-staffed community clinic. 10
In this report from the field, we discuss emerging themes and navigation strategies offered through salient patient experiences told from the perspective of patient navigators. Through these personal accounts, we aim to offer a unique window into the barriers faced by the uninsured women enrolled in the DPNC and the strategies used by patient navigators to improve patients' timeliness of care and bring forth a community-nested PCMH for these women. It is our hope that this report offers insight to future programs that are similarly dedicated to improving the health of at-risk, low-income, uninsured women worldwide.
Methods
Conceptual Framework
Our model of patient navigation originated from the Chronic Care Management Model, which informs four components of the navigator's role: 1) identifying cases, 2) identifying individual barriers to care, 3) designing and implementing a care plan addressing those barriers, and 4) tracking through completion of all services.
14
This four-pronged model, which includes the patient, provider, and health-care system, is intended to address and alleviate barriers at each point of contact in the health-care system.
15
In addition, we further considered the challenging environmental and social realities in which patients seek care, such as low financial resources, limited English proficiency, home insecurity, lack of transportation, and immigration legalities. Toward that end, we conscientiously designed a navigation program that connected health-care and wraparound services to achieve a more
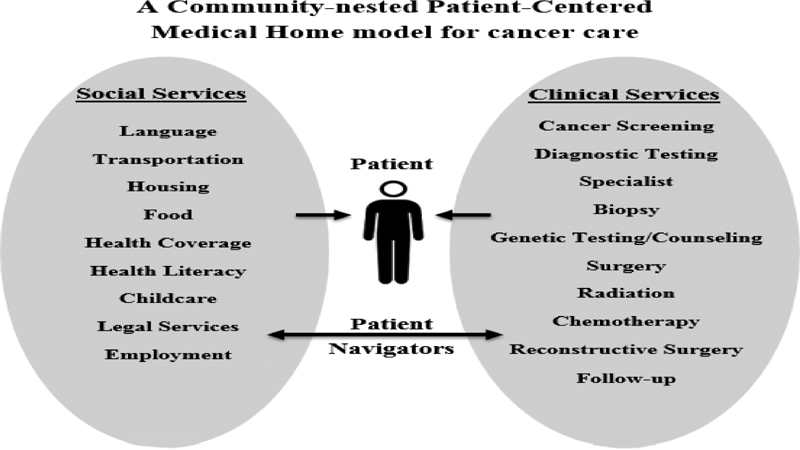
The DPNC connects community-based social service delivery with the PCMH to achieve a
Design and Setting
As a part of their professional role, patient navigators composed personal accounts of their experiences working with study participants in DuPage County, with particular emphasis on the barriers faced by DPNC patients and the navigational strategies implemented to address these barriers. Case studies were composed from data on patient-identified barriers, encounter information, and navigator care coordination activities collected via patient navigator tracking logs. The Northwestern University Institutional Review Board (IRB), the IRB of record for Access DuPage, approved all study procedures.
Project Participants and Patient Navigators
Patients were eligible to enroll in Access DuPage for health-care services if they were uninsured, resided within DuPage County, and had a household income below 200% of the Federal Poverty Level. 16 Access DuPage enrollees with an abnormal breast or cervical cancer screening test result or new cancer diagnosis were referred to DPNC patient navigators through the county health department's Illinois Breast and Cervical Screening Program (IBCCP) and local community health-care providers. Study enrollment occurred from March 2009 to September 2012.
The project's six patient navigators were linguistically matched to DuPage's patient population and, collectively, were proficient in Spanish and/or English. Aligned with the targeted gender-specific cancers of interest, all patient navigators were female. Navigators' primary roles were to guide women who received an abnormal cancer screening test through diagnostic resolution for those with a negative cancer diagnosis or through treatment completion for those with a positive cancer diagnosis. Patient navigators moved freely among multiple clinics and hospitals and navigated patients regardless of patients' clinical or hospital affiliation. Navigators made appointment reminder calls; provided informational, logistical, and emotional support; provided interpreter services; referred patients to community health and human resource wraparound services; and connected patients to health insurance and primary care homes as needed. Throughout the study period, navigators sought to expand ties with local health and social service organizations able to assist patients. Navigators embedded in clinical teams formed strong working relationships with physicians, clinic staff, and support staff. More detailed descriptions of navigators' interactions with medical teams are published elsewhere. 17
Data Collection and Analysis
We obtained written informed consent prior to delivery of navigation services and data collection on barriers to care using patient navigation tracking logs. Case studies were composed exclusively by three of the study's patient navigators (authored herein: N.H., C.F., and C.B) and were formatted and supplemented with additional information obtained through unstructured interviews with patient navigators conducted by ATS and NJN. A case study is “an in-depth exploration from multiple perspectives of the complexity and uniqueness of a particular project, policy, institution, program or system in a ‘real-life’ context.”
18
Using a case study approach,
19
patient navigators purposively selected
Results
A total of 697 of 1018 potentially eligible patients (68.5%) were referred by IBCCP program coordinators of the DPNC, of which 477 patients participated in the research study. Ethnicities represented among DPNC participants included Hispanic White (62%), non-Hispanic White (29%), non-Hispanic Black (6%), and Asian (3%). The most common primary languages spoken included Spanish (57%) and English (39%). Additional demographic information about study participants is provided elsewhere. 10 The case studies presented below are the stories of four of those participants, as told by patient navigators. The interdisciplinary team of patient navigators possessed varied educational backgrounds: two navigators were trained social workers (one Master's level and one Bachelor's level); two navigators had Master of Public Health degrees; two navigators had Bachelor of Arts degrees; and one navigator had a high school diploma.
The following DPNC patient navigators' personal accounts qualitatively depict the true voices of navigators, who have helped to resolve extensive barriers to care, and offer insight into effective navigation strategies.
Stories from the Field: Voices of DPNC Patient Navigators
Mary
Mary openly shared her personal hardships with me during her first session at a breast health center. Mary was a recent immigrant from Eastern Europe with a limited support system. She diligently balanced two jobs as a medical assistant and as a caregiver to her disabled child. Due to her husband's abusive nature and disinterest in raising their children, she planned to file for divorce after establishing US citizenship.
As we waited to meet with her surgeon regarding her breast biopsy, Mary became tearful, stating that she was
Following her positive breast cancer diagnosis, I strongly encouraged Mary to disclose her HIV status to her surgeon, who explained that her HIV status would not affect her surgical plan. After contacting local AIDS legal services, I was also able to reassure Mary that her HIV status would have no bearing on her citizenship status. Due to her current citizenship status, however, she was ineligible for Medicaid. By coordinating with her surgeon's office, immigration specialists, the county's health department, and with my colleagues, we formulated a plan for Mary to have her surgery just after her citizenship ceremony scheduled for the following month.
Importantly, the necessary health education I provided Mary allowed her to make an informed decision to seek both HIV care services and breast cancer treatment. Moreover, through widespread coordination among medical and community resources, I was able to aid Mary in obtaining the cancer care and financial assistance she needed.
Carmen
Carmen immigrated to USA a year prior to beginning patient navigation services. She spoke only Spanish and, beyond language barriers, faced significant obstacles such as long overnight shifts as a factory worker and caretaking for her mother who had recently suffered from a stroke. Following a Pap test, Carmen was informed that she had a low-grade lesion and would need a colposcopy to remove the precancerous cells. Carmen enrolled in the health department's IBCCP program and was referred to the DPNC.
Though Carmen's evening hour work schedule made it difficult for me to reach her, I aided her in scheduling follow-up appointments for exams and her colposcopy procedure, emphasized the importance of attending her appointments, and provided health education. I additionally helped Carmen to apply for health insurance, ensuring her that proof of citizenship was not required. Carmen successfully completed the colposcopy, which resulted normal, and she subsequently assured me that she would attend recommended follow-up visits in the future.
Sally
As patient navigators, ideally we would like to see every patient reach diagnostic resolution, and if necessary, treatment completion. While I addressed several barriers to care for Sally, who faced a pending home eviction and various medical conditions, she was ultimately lost to follow-up. Sally was referred to our program after receiving an abnormal breast cancer screening test. She lived alone, lacked a source of income, and walked five miles round trip to her doctor's visits. I connected Sally with a program that provides low-cost transportation to medical visits for qualifying county residents.
Though Sally was then able to attend her medical visits, she lacked financial resources to pay for her prescriptions. After extensive research online and through local contacts, I found an antibiotics distribution program through a local pharmacy that would provide her prescription antibiotic–-free of cost. Due to Sally's limited access to transportation, I delivered her medication to her home.
To address Sally's pending home eviction, I contacted every agency in DuPage County that provided shelter or subsidized housing. Unfortunately, due to a number of factors, none of these agencies was a viable option for Sally. I knew that I had made significant strides in addressing several of Sally's barriers but realized that, despite my best efforts, I would not be able to resolve her housing issue. Ultimately, Sally moved out of the country, at which point I was unable to continue navigation services.
Jamila
Jamila, a recent immigrant from South Asia, was referred to the DPNC following a breast abnormality. Jamila needed magnetic resonance imaging (MRI), a test not covered by IBCCP, and as a permanent US resident for less than five years, Jamila did not qualify for Medicaid. I helped Jamila enroll in Access DuPage, and within a few weeks, she was able to schedule her MRI appointment.
Beyond her positive screen, Jamila faced a number of significant challenges to her personal life. Jamila, her husband, and their young children lived off of Jamila's husband's modest monthly wage of $350, keeping them 200% below the federal poverty level. Jamila's sister initially allowed Jamila and her family to live rent free in an apartment that she owned, but due to personal financial reasons, soon asked them to find housing elsewhere. I fastidiously researched subsidized housing options within DuPage County but unfortunately discovered that Jamila and her family did not qualify. I eventually found housing for Jamila within a neighboring county that had a relatively short wait time of less than 18 months; however, continuation of Access DuPage enrollment required residency in DuPage County, and for that reason, her sister ultimately allowed Jamilia's family to remain in her apartment.
Following inconclusive MRI results, Jamila was referred for a needle biopsy and subsequently diagnosed with breast cancer. Jamila's husband was able to find a higher paying job in another state, leaving behind Jamila to receive treatment and care for their children. Because she continued to reside in DuPage County, Jamila received a full round of chemotherapy followed by over a month of radiation therapy. During that time, she had access to genetic counseling through a safety net hospital, received a wig through a cancer advocacy organization, and was provided free transportation to and from treatment. As Jamila's navigator, I collaborated with a team of physicians, social service agencies, and community partners, working to make her cancer care as seamless as possible during this challenging life phase.
Recurring Patient Themes and Navigational Strategies
These navigator stories revealed common recurring themes of barriers to follow-up care including: limited financial resources, co-morbid disease, fear of deportation, home insecurity, feeling overwhelmed by the healthcare system challenges, lack of health insurance, reluctance to seek care due to language barriers or fear of repercussions, lack of occupational opportunities, and lack of transportation.
The DPNC patient navigators developed a wealth of navigational tools, with navigation strategies that encompass addressing patient concerns regarding treatment hesitation; researching affordable housing, transportation, and prescription options; emphasizing health education; coordinating interagency communication; ensuring patient care logistics; offering translation services during clinic visits and scheduling; and developing critical bonds with local health clinics and community organizations to improve patients' access to financial, social, and educational resources. The navigators additionally made every effort to avoid having a patient lost to follow-up by obtaining all available means of communication at the initial encounter; arranging for transportation to appointments; and being as flexible as possible. Additionally, while each navigator had their own patient caseload, they acted in a team fashion for consultation and support. The navigators' various educational backgrounds in social work and public health allowed for a greater shared knowledge among the group, including community linkages, mental health resources, and governmental assistance programs, as well as greater awareness of the health-care system at large.
Discussion
DPNC patient navigators are aware of the crucial nature of their role within the patient care team and are dedicated to helping their fellow community members to achieve and maintain health and wellness. Moreover, as described through their stories, the DPNC patient navigators have instilled both confidence and hope in DPNC patients, many of who otherwise lack social support. These stories from the front line begin to capture both the practical and compassionate support that navigators provide to patients, critical elements in the interface between patients and the health-care system. Considering the significant complexities of the US healthcare system, the rapidly shifting national demographic trends, and existing health disparities, patient navigation serves a critical function throughout care and, importantly, connects patients to a medical home.
As illustrated in these stories, despite the availability of a PCMH, women still encountered multiple barriers to care that stemmed from the environmental, economic, and social context in which they lived. Within the patients' microsystems, DPNC patient navigators were able to make headway toward a
As health-care reform implementation continues within USA, patient navigators will play increasingly diverse roles across the health-care continuum and in the policy arena, but the effectiveness of navigators as demonstrated in our case studies may depend on their ability to advocate for and bridge the health-care system with wraparound services for the diverse communities they serve. Advocate roles can be complex; our team's prior study of the navigator-patient relationship pinpointed numerous challenges for navigators in maintaining professional and personal boundaries when providing logistical care coordination, social, and emotional support. 22 As illustrated by these stories, some patients' needs were beyond the ability of DPNC navigators to address, as was the case for Sally, whose home eviction required her to leave the country despite the navigators' best efforts to resolve her housing problem. Understanding to what extent navigators can leverage resources in resource-thin environments may be critical for innovative safety-net delivery systems and warrants additional investigation. 10
Given the significant poverty and health inequities faced by patients seeking care in developing countries as well as the oftentimes-strained health-care systems within these settings, the use of the
Study Limitations and Next Steps
Notably, while this study offers rich descriptions of the patient navigator perspective, it did not assess quantitative measures of the patient navigation experience such as time spent navigating certain barriers or number of patient encounters. Furthermore, while future research is underway to track longitudinal health outcomes among this patient population, this information is not included within this report. Though the generalizability of this study is inherently limited by the specific patient population included, the complex needs faced by these patients are not unique to the Access DuPage population. Other cancer navigation studies have documented similar patient navigation needs including: assisting with finances, insurance, transportation, end-of-life issues, dependent-care help, scheduling of appointments, and activities of daily living;25,26 addressing social and cultural barriers to care; and bridging the gap between social and medical needs. 27 Yet, as noted by Guadagnolo et al, few studies have patient navigation service delivery metrics to inform the resources necessary to implement comprehensive patient navigation services. Accordingly, our study provides new insight into possible future community-based participatory research program evaluation measures from the patient navigation perspective. 25 Additional future efforts should continue to highlight the patient navigator experience via qualitative interviews as well as quantitative measures of patient navigation services provided in domestic and international settings. Although a recent navigation efficacy trial for cancer care concluded that navigation likely has the greatest impact in low-resource settings and among populations most at risk for delayed follow-up, 21 exploration of patient navigator experiences at different resource level settings may also yield additional insights. Within USA, longitudinal studies assessing the impact that the Affordable Care Act has on patient navigation services may be paramount for future research, funding, and evaluation efforts in this arena.
Conclusions
As highlighted through the cases presented, patient navigators individually tailored navigation strategies to guide each patient and aided them in overcoming the oftentimes fragmented, complex, or confusing care. Tailored strategies to resolve barriers ranged from researching affordable housing, transportation, and prescription options to helping patients apply for health insurance and developing critical bonds with local health clinics and community organizations to improve patients' access to resources. As the DPNC navigators exemplify, patient navigators can be champions of addressing existing health disparities among underserved populations. As health care reform opens the door for many to the healthcare system, it also continues to leave the most vulnerable patients behind, 28 so we may need navigators to play myriad roles across the health-care continuum. It is our hope that by giving a voice to the navigators' accounts, we are able to shed light on the extraordinary tasks and accomplishments that patient navigators have embraced and to provide insight to future navigation programs both domestically and abroad.
Footnotes
Abbreviations
DPNC, DuPage County Patient Navigation Collaborative; IBCCP, Illinois Breast and Cervical Screening Program; IRB, Institutional Review Board; MRI, magnetic resonance imaging; NIH, National Institutes of Health; PCMH, Patient-centered medical home.
Author Contributions
Provided substantial contributions to the conception and design of the project, project supervision, acquisition of data, interpretation of data, funding acquisition, drafting of the manuscript, and critical revisions of the article: MAS. Provided drafting of the article, critical revisions of the article, interpretation of data, administrative support, and completed unstructured interviews with patient navigators: ATS. Provided drafting of the article, critical revisions of the article, acquisition of the data, interpretation of the data, and administrative support: NJN. Composed patient navigator accounts included in the article and contributed to drafting of the article: NH. Composed patient navigator accounts included in the article and contributed to drafting of the article: CF. Composed patient navigator accounts included in the article and contributed to drafting of the article: CB. Provided conception and design of the project, project supervision, funding acquisition, and acquisition of data: KM. Provided conception and design of the project, project supervision, funding acquisition, and acquisition of data: RE. Provided drafting of the article, critical revisions of the article, and interpretation of data: LST. Provided contributions to the conception and design of the project and project supervision: XQD. All authors read and approved the final article.