
Abstract
Rural and minority women are disproportionately impacted by the obesity epidemic; however, little research has studied the intersection of these disparity groups. The purpose of this study was to examine the influence of racial identity on motivation for weight loss and exercise among rural, African-American women with an obesity-linked chronic disease. A total of 154 African-American women were recruited from the patient population of a Federally Qualified Health Center in the rural South to complete a questionnaire battery including the Multigroup Ethnic Identity Measure and separate assessments of motivation for weight loss and exercise. Multivariate analyses, controlling for age, education status, insurance status, and body mass index revealed that attachment to ethnic identity was predictive of motivation for exercise but not for weight loss. Our findings suggest that attachment to ethnic identity may be an important factor in motivation for change among African-American women, particularly with respect to exercise, with direct implications for the development of culturally and geographically tailored weight loss interventions.
Introduction
Motivation for weight loss and exercise
The obesity epidemic in the United States continues to rise, with national estimates currently placing adult obesity rates at 34.9%. 1 The obesity rate is not constant across populations, however, with both women and African-Americans disproportionately impacted by obesity. 1 The underlying reasons behind these differences are complex and likely involve the overlapping influence of multiple sociologic and demographic factors. While determining the fundamental root is challenging, it is likely that motivation for weight loss and exercise is influencing the ability of women—and in particular minority women—to achieve and maintain a healthy weight. 2 Understanding the factors that impact motivation for weight loss and exercise in minority women is particularly important, but understudied—currently, 56.6% of black women fit the qualifications for obesity, which is over 20% higher than the average American female. 3 Correspondingly, black women have the highest rates of diabetes of any female race/ethnicity categories, 4 indicating a strong need to examine motivation among minority women.
The literature has recently begun to explore those factors that motivate women in general to pursue weight loss and exercise goals.5,6 Many women who plan to lose weight and exercise cite better health outcomes as an important motivating factor.5,6 Others cite influences such as social support from family and friends, societal pressures encouraging thinness, and a desire to fit into clothing better.5,6 Of these motivating factors, health and appearance are frequently cited as the two predominant reasons women choose to pursue weight loss and exercise goals.
While women give many reasons why they hope to engage in weight loss and exercise behaviors, they also list many barriers that prevent them from achieving that goal. Time constraints commonly arise as a reason why women feel they cannot successfully try to lose weight or exercise, typically because their other commitments, such as work, children, and additional responsibilities, do not afford them enough time.6–8 The expense of engaging in weight loss behaviors, such as purchasing healthier foods such as fresh fruits and vegetables, 7 has also been specifically identified as a barrier for women to achieve a healthy weight.
Certain groups experience barriers to weight loss and exercise differently than their peers, such as members of a racial/ethnic minority and individuals who reside in rural settings. For instance, previous research has shown that some minority groups are conflicted by what they feel healthy behaviors represent. In one study, minority participants felt that health promotion behaviors, such as healthy eating and exercise, were associated with predominantly white, middle-class individuals. 9 Because the minority participants felt detached from that group, they were not motivated to engage in weight loss behaviors. As a result, racial/ethnic identity has been shown to impact the initiation of healthy behaviors even when an individual knows the benefits of engaging in the activities. 10 What is less understood, however, is how the strength of affiliation one has with her ethnic identity is related to weight loss behaviors and the motivation to engage in them.
Racial/ethnic identity
When considering the connection between racial/ethnic identity and motivation for weight loss, it is important to recognize that this identity itself is more salient and influential among members of racial/ethnic minority groups than among members of the majority culture. For instance, African-American women tend to feel more strongly attached to their ethnic identity than European American women.11,12 The level of identification with one's ethnicity can impact multiple facets of life, especially if one strongly identifies with their ethnicity.
Ethnic identity is often defined as a set of demographic characteristics, such as common culture and national origin.
13
It is commonly used interchangeably with racial identity, especially when a discussion of culture is present.
13
Understanding the attachment to ethnic identity is important, because it has been associated with various constructs related to motivation for weight loss such as self-esteem, stereotypes, and body satisfaction.5,11,14 In African-American populations in particular, attachment to ethnic identity has been tied to self-esteem, with individuals who felt a stronger tie to their ethnic identity scoring higher on measures of self-esteem.14,15 Additionally, ties to ethnic identity have been shown to relate to whether or not an individual embraces positive or negative stereotypes about their ethnicity, with stronger attachment to ethnic identity correlated with a focus on more
Ethnic identity also influences the internalization of beauty ideals, which in turn likely impacts an individual's body satisfaction (and thereby weight loss motivation). Some research indicates that ethnic identity can act as a protective factor against harmful ideals such as extreme thinness. For example, Oney et al 15 found that racial identity can moderate the relationship between body satisfaction and self-esteem and can maintain self-esteem even when body satisfaction is low. Ethnic identity also has been shown to strengthen the link between self-esteem and body satisfaction, wherein body satisfaction is higher if one also has a strong affiliation with their ethnic identity and high self-esteem. 15 Another study found that the higher acceptance of full-figure bodies in African-American culture can also help to lower the incidence rate of eating disorders in African-American populations. 11 Unfortunately, research suggests that strong ethnic identity can sometimes also complicate body satisfaction in minority women, due to the competing presence of majority culture's beauty ideals and ethnic beauty ideals. 16
While there are multiple factors that motivate individuals to engage in weight loss and exercise behaviors, like health promotion, appearance, and social support, many of these motivating factors appear to be affected by cultural beliefs. Because one's ethnic identity can both encourage and discourage participation in weight loss and exercise behaviors—even when they are known to promote health—it is possible that ethnic identity could alter motivation for losing weight and exercising. Because certain research has also indicated that ethnic identity acts as a protective factor against
Rural influence
Although prior research has attempted to examine the impact of racial/ethnic identity on weight loss motivation and behaviors, these studies have taken place predominantly with urban-based samples. This is problematic because rural residents face circumstances different from their urban peers that can hinder the use of weight loss and exercise behaviors. Rural residents often have lower access to healthy food and to workout facilities that could promote exercise behavior.17–19 Residents of rural areas also tend to have higher body mass index (BMI) and are less active than their urban peers.20,21 In rural areas, members of racial/ethnic minority groups face not only these rural-centered barriers to healthy living but are also more likely to face heightened degrees of racism and discrimination. 22 As a result, it is unclear to what extent prior findings connecting ethnic identity and weight loss behaviors translate into the unique cultural and socioeconomic climate of rural areas. Furthermore, prior studies have not adequately examined the different layers of motivation necessary to engage in and sustain weight loss; for instance, motivation for weight loss in the absence of motivation to engage in the activities necessary for weight loss (eg, exercise) is not as useful in the construction of interventions designed to promote health behaviors. This is particularly true with regard to African-American women, who face some of the highest burdens related to both prevalence and outcomes of diabetes and hypertension, whose main action of self-control is weight loss. Given the pronounced need for impactful interventions designed to help African-American women manage obesity-linked chronic diseases, examining ways in which culture, and specifically attachment to ethnic identity, influences motivation for weight loss behaviors could lead to new targets for culturally tailored interventions.
The purpose of this study was therefore to explore the relationship between attachment to ethnic identity and motivation for weight loss and exercise in rural, overweight African-American women currently under treatment for an obesity-linked chronic disease.
Methods
Participants
This study arose from a larger parent study in which 497 participants were recruited from the patient population of a network of Federally Qualified Health Centers located in the Southeastern United States from November 2013 through March 2015. Participants were recruited from the Federally Qualified Health Centers through one of the following three methods: direct approach by study staff, referral from front-desk staff of the clinic, and interest garnered from flyers posted within the clinic. Once informed of the study, participants were screened for eligibility. If they met the eligibility criteria (18 years of age, able to read or speak English, and diagnosis of diabetes and/or hypertension), informed consent was obtained. In this study, we selected a sub-sample of the original respondents. Specifically, the inclusion criteria (inclusive of the inclusion criteria of the parent study) of this study were as follows: (1) 18 years of age or older, (2) able to read or speak English, (3) diagnosis of diabetes and/or hypertension, (4) self-identified as female, (5) self-identified as African-American, and (6) had a current BMI of 25 or higher. These criteria left 154 individuals in the analytic sample of this study.
Procedures
Following informed consent, each participant completed a survey using the audio computer-assisted self-interview. To thank the participants for their time and effort, they were given a $15 gift card to a local retail supermarket. All procedures were reviewed and approved by the Institutional Review Boards of Georgia Southern University and Mercer University, complied with the principles of the Declaration of Helsinki, and all data were collected anonymously.
Measures
Attachment to ethnic identity was measured using the Multigroup Ethnic Identity Measure (MEIM) scale, which assesses the level of identification with one's racial/ethnic group.
23
The scale first asks participants to identify what ethnic group they most identify with, followed by a series of 12 questions that assesses various ways an individual demonstrates attachment to their ethnic group (eg, “I feel a strong attachment toward my own ethnic group” and “I have a strong sense of belonging to my own ethnic group”). Each of the questions is answered using a 4-point Likert-type scale. Potential responses range from
Stage of change for weight loss and exercise was assessed independently of each other using standardized measures developed by the originators of the Transtheoretical Model and their collaborators. Additionally, standardized measures were used to assess participants' decisional balance (ie, how an individual relatively weights pros and cons regarding changing a behavior) separately for both weight loss and exercise. Stage of change for exercise was assessed using a 24-item inventory
24
utilizing a 4-point Likert-type scale (1 = strongly disagree, 4 = strongly agree; sample item: “As far as I'm concerned, I don't need to exercise regularly”). Stage of change for weight was measured using a 4-item index
25
asking participants to answer yes/no questions related to weight loss-related behaviors (eg, “In the past month, have you been actively trying to lose weight?”). Standardized scoring procedures are followed for both questionnaires in order to determine which stage of change participants are in for each outcome (ie, precontemplation, contemplation, preparation, action, and maintenance). The stages of change for exercise instrument demonstrated very strong reliability in this sample (
Analysis
In order to conduct our analysis, the stages of change for both exercise and weight loss were binarized, with those in the action stage or higher contrasted with those below the action stage; this split allowed for a comparison of those actively engaged in exercise and/or weight loss behaviors with those who were not actively engaged. In order to delineate high vs. low levels of decisional balance for both weight loss and exercise, the total endorsement of
Data were examined descriptively to summarize the demographic characteristics of the sample. In addition to our primary variable of interest—attachment to ethnic identity—we examined each variable that could have theoretically impacted the outcome variables to discern potential univariate relationships. Candidate variables examined included age, BMI, poverty status, comorbidity status, education level, employment level, and insurance status. We examined the continuous variables with analysis of variance and the categorical variables with chi-square tests. All variables that tested significant at the
Results
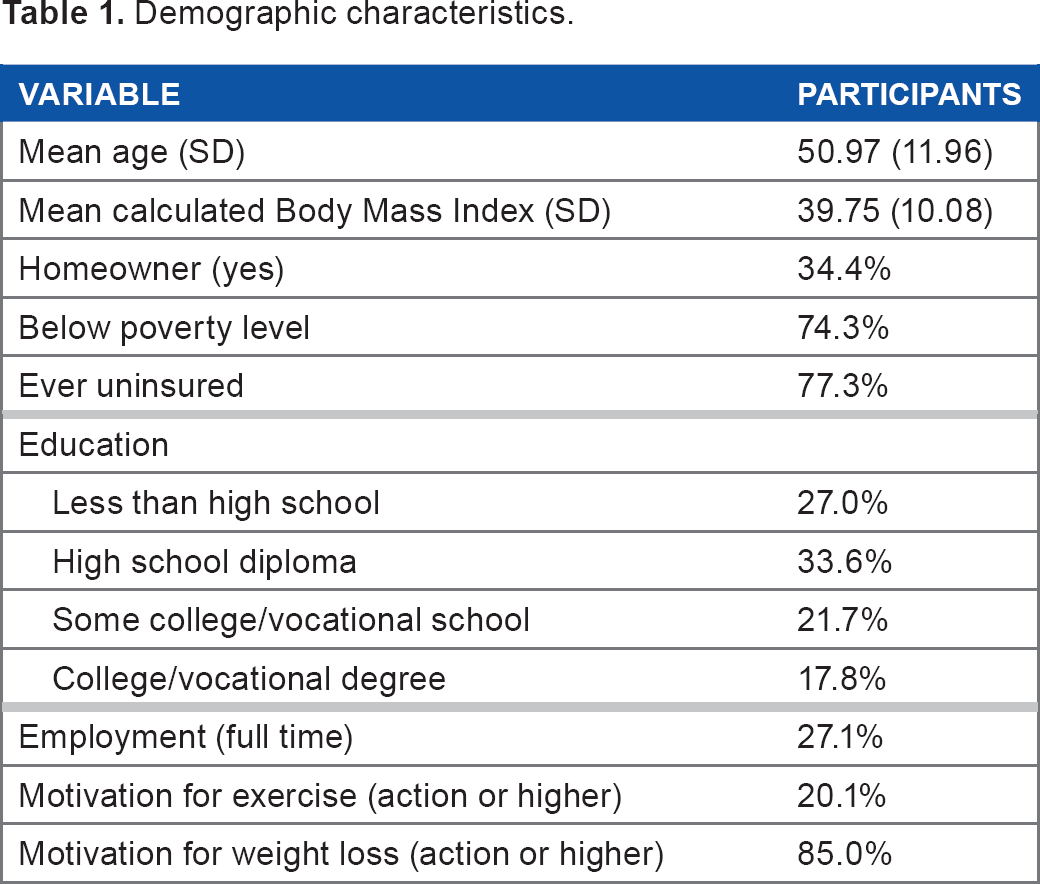
Participants in the analytic sample had a mean age of 50.97 (SD = 11.96) years and a mean BMI score of 39.75 (SD = 10.08). Almost three quarters of the sample had a household income less than $20,000 per year, and a similar proportion had been uninsured at some point in their life. Only 27.15% of the sample was employed full time, and 34.4% of the sample owned their home (see Table 1 for additional demographic characteristics).
Demographic characteristics.
In the final multivariate models, age, education level, and insurance did not predict any of the outcomes in our analysis (see Tables 2–5). When examining the stages of change for exercise, however, we found that attachment to ethnic identity (odds ratio [OR] = 2.672,
stages of change for exercise.
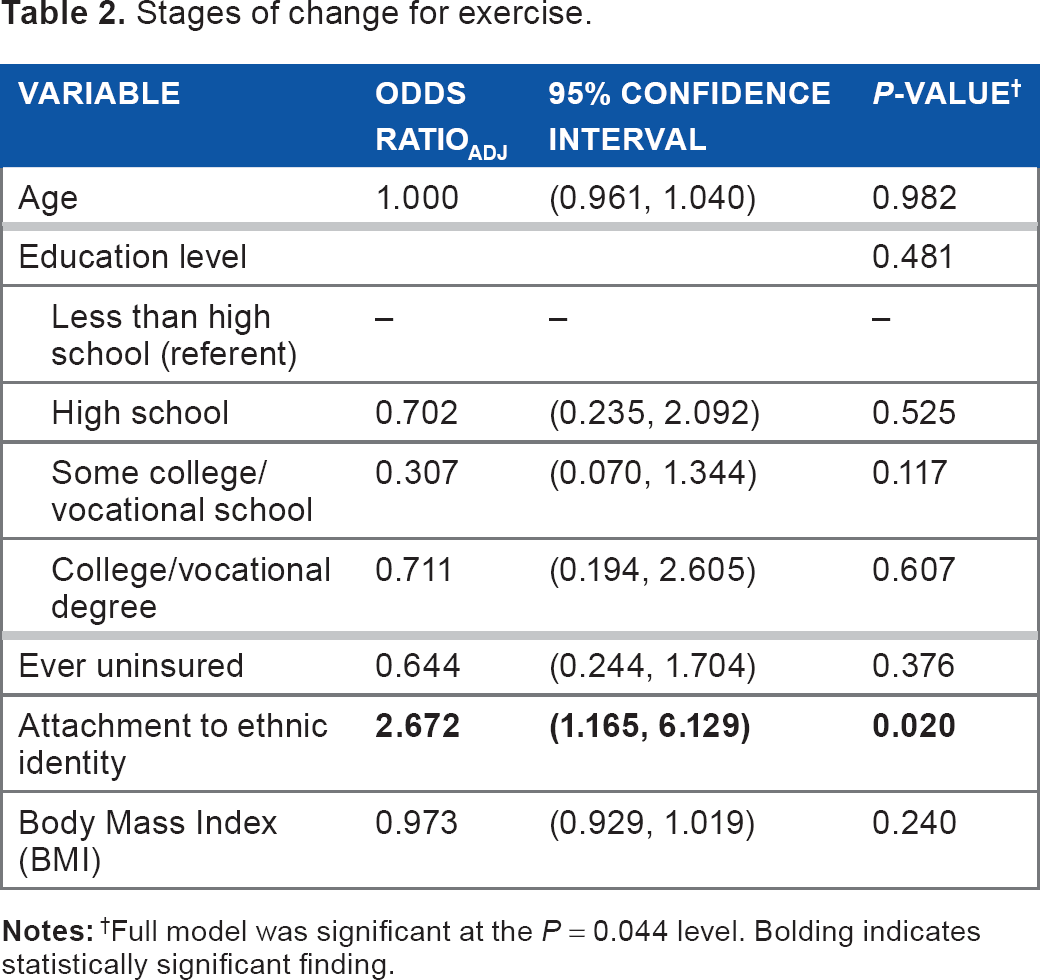
Full model was significant at the
Stages of change for weight loss.
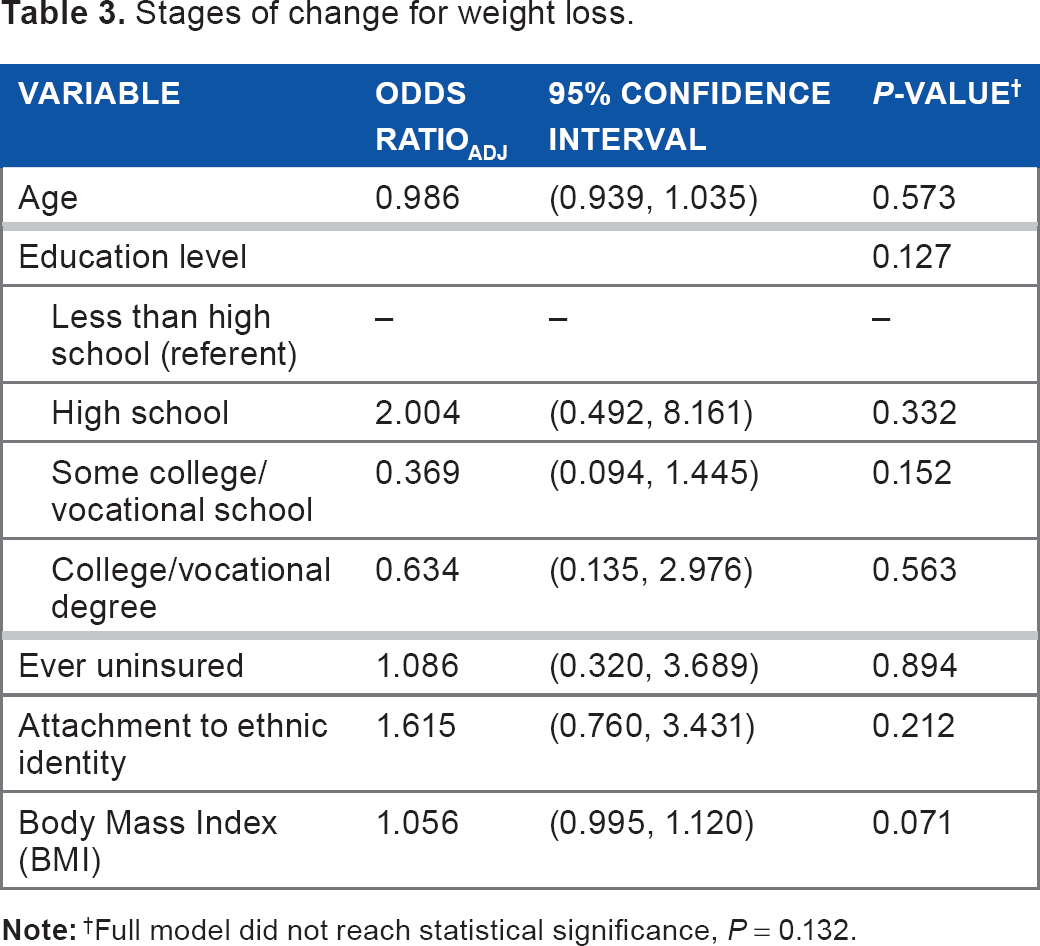
Full model did not reach statistical significance,
Decisional balance for exercise.
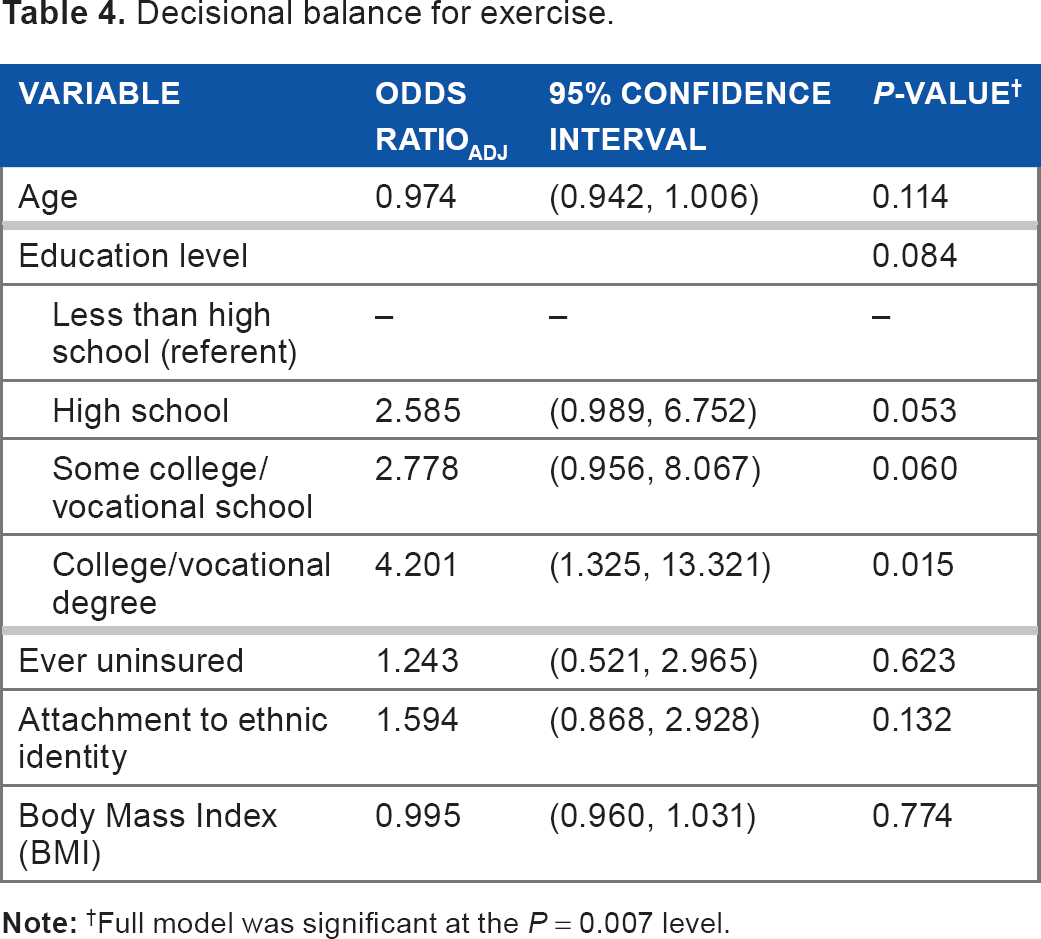
Full model was significant at the
Decisional balance for weight loss.
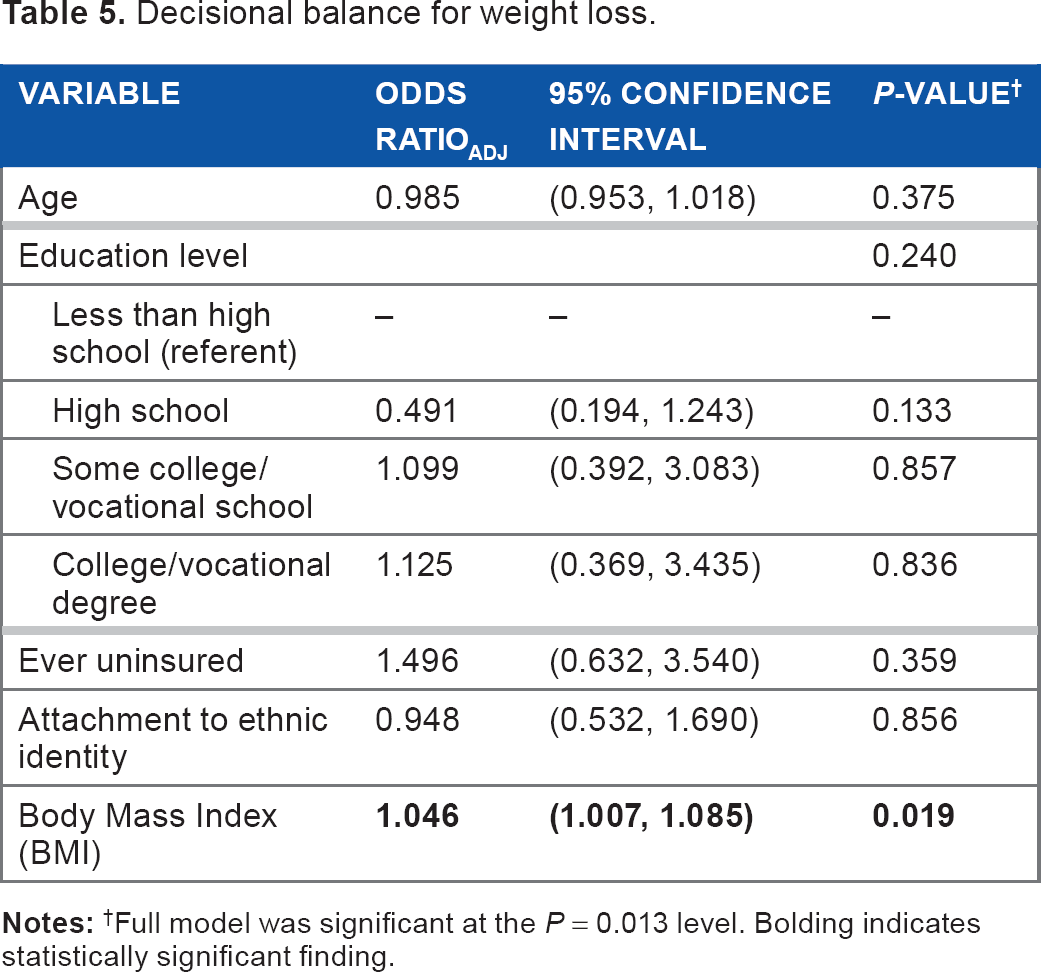
Full model was significant at the
Discussion
Overall, our findings suggest that attachment to ethnic identity may be an important factor in motivation for change among African-American women, particularly with respect to exercise. Across all variables examined for the stage of change for both exercise and weight loss, attachment to ethnic identity was the only variable that significantly predicted being in the action stage of change or higher, exerting more influence than demographic factors often associated with motivation for change (eg, poverty).29–31 It could be that the relative homogeneity of the sample in terms of socioeconomic status partially controlled for these other effects; however, both education level and insurance status were included in the model due to the strength of their univariate effect. The fact that these effects disappeared once accounting for attachment to ethnic identity is particularly interesting. While the concept of culturally tailoring interventions is certainly not new, our findings suggest that it may be particularly important and relevant when considering prevention/intervention with African-American women in particular.
The most important factor in the current study's findings, however, is the direction of association. Not only was attachment to ethnic identity the only variable associated with motivation for change, but the association was also protective; that is, women who were more attached to their ethnic identity were more likely to be motivated to engage in exercise activities. This becomes particularly important when considering the study population; all women in the study were overweight, rural African-American women currently under treatment for an obesity-related chronic disease. Therefore, this link could provide important contextual information in the development of culturally tailored exercise and weight loss interventions to help address the clear disparity in weight and weight-related outcomes among minority women. Often, barriers to motivation become the focus of intervention work as intervention programs seek to help individuals overcome obstacles to behavior change that may or may not be readily resolved (eg, low access to healthy food options). 30
By identifying a specific facet associated with protective behaviors, the study suggests that there may be promise in exploring ways to incorporate positive cultural messages into health behavior interventions. Specifically, our findings suggest that cultural factors may be particularly salient for rural African-American women when making the decision to engage in exercise behaviors. The magnitude of effect was fairly strong, with a single point increase on the MEIM scale more than doubling the likelihood that women were in the action stage of change or higher. While the study design was exploratory and cannot adequately identify which specific aspects of attachment to ethnic identity are most relevant in this relationship, it does highlight an important area for future investigation. It could be that positive stereotypes regarding athletic ability in African-American populations lead to an elevated sense of connection between ethnic identity and exercise, or that notions of physical strength have a strong cultural link. Future exploratory research is needed to fully examine the underlying cultural norms connecting ethnic identity and exercise activities, as well as what messages and cultural factors are influencing those norms.
Interestingly, while ethnic identity was associated with increased motivation for exercise, it was not associated with increased motivation for weight loss. Previous research has shown that rural African-American women are more motivated to lose weight than their nonminority counterparts; 32 therefore, it could be that the high level of motivation for weight loss precluded sufficient variation to see a companion connection between motivation for weight loss and ethnic identity. The fact that motivation for exercise was related to ethnic identity rather than motivation for weight loss is actually of higher significance—the current study suggests that within overweight African-American women with obesity-linked chronic diseases, those who are more attached to their ethnic identity are also more motivated to engage in exercise behaviors (one of the critical components of successful weight loss). Prior research has shown that motivation for weight loss is more readily achieved than motivation for the activities necessary for weight loss, leaving a stark need for an understanding of what influences motivation for engaging in underlying weight loss behaviors (such as exercise). Our finding that this may have a strong cultural link—above and beyond other more intuitive demographic links—underscores the importance of culturally tailoring interventions for minority rural women.
However, most weight loss/exercise programs are not culturally tailored, instead taking a one-size-fits-all approach across cultural groups. Future research should specifically investigate which aspects of African-American culture appear to be most strongly increasing motivation for exercise behaviors, so these factors can be incorporated into intervention programs designed specifically to match the cultural realities of rural African-American women. For example, it could be that the use of culturally congruent models is important in health education materials, or that peer or social network-driven interventions could be particularly impactful for African-American women's motivation for exercise. Future research should explore which specific cultural tailorings would be most desired and impactful. In addition, it is interesting that while ethnic identity was associated with motivation for exercise, it was not associated with motivation for weight loss. This could be due to the high level of motivation for weight loss (85% of the sample), leaving little room for ethnic identity to demonstrate a significant impact. Furthermore, ethnic identity was not related to decisional balance for either exercise or weight loss—in other words, while ethnic identity may be associated with the underlying motivation to engage in exercise, our study suggests that it is not similarly related to the way in which rural African-American women perceive the pros and cons of engaging in exercise activities. This only further underscores the need for future research designed to investigate the potential cultural link, and the mechanism by which it is occurring (since it does not appear to be impacting motivation through impacting decisional balance).
The study's findings should be viewed in light of its limitations. First, while participants came from a multisite network of clinics, all participants were recruited from the same multicounty region of the rural Southeast. Second, because the study was not designed to specifically examine which cultural factors were associated with the observed differences, we are unable to identify specific potential intervention components; future qualitative research in particular may be helpful in elucidating what specific cultural aspects are associated with the desire to engage in exercise activities. Third, our study's sample was limited to individuals with a current diagnosis of hypertension or diabetes, and it could be that factors influencing motivation are not the same in nonclinical samples. However, because overweight individuals with an obesity-linked chronic disease are directly impacted by their weight status, the development of interventions specifically for this population is highly needed. Fourth, while the MEIM is used increasingly in adult populations and demonstrated excellent reliability in our sample, it was originally developed to assess ethnic identity attachment in younger populations. Fifth, because recruitment included both direct approach and passive recruitment methods, we are unable to calculate precise participation rates. Finally, given that the average BMI was well above obese (and bordering some definitions of morbid obesity), it could be that additional comorbid conditions such as sleep apnea and cardiovascular complications impact motivation for exercise. The presence of these conditions, however, is likely not tied to ethnic identity attachment, suggesting that our findings hold.
Conclusion
Our study suggests that, among overweight African-American women with a current diagnosis of diabetes and/or hypertension, attachment to their cultural identity may be an important predictor of motivation to engage in exercise behaviors. This effect was more pronounced than any other relationship investigated and merits future research (particularly mixed-methods) to identify the specific aspects of culture that impact motivation and ways in which that motivation can be enhanced in other women.
Footnotes
Acknowledgments
This study was completed as part of the 2015 Disparities Elimination Summer Research Experience program and was supported by grant P20MD006901 through the National Institutes of Health/National Institute on Minority Health and Health Disparities. The views expressed are those of the authors and do not represent the views of NIMHD, NIH, or DHHS.
Author Contributions
Conceived and designed the experiments: KBS, JCW. Analyzed the data: KBS, JCW, SM, WP, MC. Wrote the first draft of the manuscript: KBS, JCW, SM, WP, MC. Contributed to the writing of the manuscript: KBS, JCW, SM, WP, MC. Agree with manuscript results and conclusions: KBS, JCW, SM, WP, MC. Jointly developed the structure and arguments for the paper: KBS, JCW, SM, WP, MC. Made critical revisions and approved final version: KBS, JCW. All authors reviewed and approved of the final manuscript.