
Abstract
Preeclampsia is a major cause of maternal mortality worldwide, with many preventive strategies tested. In this review we intend to provide a synthesis of available studies of these strategies that have been tested, including systematic reviews. We will not be performing systematic review of the studies here. Of these strategies tested only low dose acetyl salicylic acid (ASA) and calcium can be considered helpful for prevention at this time. A recent meta-analysis showed a benefit of low dose ASA for both high (RR 0.75, 95% CI 0.66 to 0.85) and moderate risk groups (RR 0.86, 95% CI 0.79 to 0.95). Therefore, low dose ASA in high risk groups may be useful, with a possible smaller benefit in moderate to low risk women. Another meta-analysis looking at calcium shows benefit for both high and low risk groups with an overall reduction in the risk of preeclampsia (RR 0.48, 95% CI 0.33 to 0.69). As a result, prenatal supplementation of calcium may be beneficial for the prevention of preeclampsia. However, vitamins C and E, zinc, fish oil, and magnesium supplementation have been discounted as potential preventive strategies. Nitric oxide, folic acid, and antithrombotics have not been well studied and there is insufficient data for reliable conclusions to be made. Areas of ongoing research that appear promising in the prevention of preeclampsia include modifiable metabolic factors, angiogenic proteins, angiotensin receptor antibodies, and syncytiotrophoblast microparticles. Strategies targeting these areas may provide opportunities for therapeutic interventions.
Introduction
Hypertensive disorders of pregnancy are major contributors to maternal mortality worldwide. In the United States, 17.6% of maternal deaths are attributed to hypertensive disorders of pregnancy. 1 Preeclampsia complicates 5%–8% of pregnancies. 2 This is higher in the presence of certain risk factors such as nulliparity, multifetal gestation, chronic hypertension, chronic renal disease, diabetes mellitus, vascular or connective tissue disease, antiphospholipid antibody syndrome, obesity, age over 35, and African American race. 2 Also, women with a prior history of preeclampsia in an antecedent pregnancy are at high risk for a recurrence (7.5% to 65% in different studies)3–5 in the subsequent pregnancy. These risk factors can be used to predict patients at increased risk, and thereby benefit from prophylactic measures.
The etiology of preeclampsia is unknown, and pathophysiology is poorly understood. Therefore, any preventive strategies developed are mostly speculative. There have been many interventions tried, but very few have been well studied enough to reach any conclusion on risk and benefit profiles.
We will provide a brief review of some of the most common preventive methods studied (antiplatelets, calcium, vitamins C and E, zinc, fish oil, magnesium, and nitric oxide), and emerging areas of interest. We will also summarize the most recent evidence. Though other strategies have been studied, including progesterone, anti-hypertensives, physical activity, and other dietary modifications, we will not review them here, as these have been addressed elsewhere, and there are no recent studies or updates that have clinical implications. We will not be performing a systematic review, but a synthesis of available data including systematic reviews. We will be focusing on meta-analysis, mainly the Cochrane reviews as they provide a more defined and structured analysis, and large individualized randomized studies when available.
Methods
We searched
What the Evidence Shows
Beneficial in selected patients Low dose aspirin
Endothelial cell dysfunction is observed as a pathophysiologic change that attributes to most of the clinical features of preeclampsia. Mainly through increasing sensitivity to normal endogenous pressors, activating the coagulation cascade, and increasing vascular permeability. 6 The observed imbalance between production of the vasodilator prostacyclin and the vasoconstrictor thromboxane led to the theory that low dose aspirin may alter this balance in favor of prostacyclin. There have been many randomized trials of aspirin for the prevention of preeclampsia in different risk groups.7–14
The most recent large RCT in nulliparous women published in 2003 14 showed that the aspirin (n = 1644) and placebo (n = 1650) groups did not differ significantly in the incidence of preeclampsia (1.7% vs 1.6%; RR 1.08, 95% CI 0.64–1.83). However, a recent meta-analysis of 59 trials, including the above trial, showed benefit for both high and low risk groups. 15 There was a trend for the relative risk reduction to be greater in women at high risk of preeclampsia (RR 0.75, 95% CI 0.66 to 0.85) than those at moderate risk (RR 0.86, 95% CI 0.79 to 0.95). This meta-analysis concluded that administration of antiplatelet agents to women at risk leads to a 17% reduction in the risk of developing preeclampsia. Amongst women in the primary prevention trials, for every 72 women treated, one case of preeclampsia is prevented. However, for high-risk women, only 19 need to be treated to prevent one case. Overall, adverse effects appeared to be low.
There are some limitations to the interpretation of these meta-analyses; for example the timing of the initiation of the treatment, the dose, and the impact on different subgroups of patients. As preeclampsia is a disease process that likely starts at implantation, aspirin may need to be started before conception to improve outcome. The studies in the Cochrane meta-analysis were arbitrarily divided to the intervention being initiated before or after 20 weeks of gestation. Higher doses than the 100 mg dose may also have a different impact on the outcome, however the safety of higher doses needs to be further evaluated. Additionally, patients with certain risk factors may benefit more from aspirin than other patients.
At this juncture, most authors recommend low dose ASA or in high risk groups, 2 and based on the above recent meta-analysis there may be benefit in moderate to low risk women (Table 1).
Recommendations for select patients.
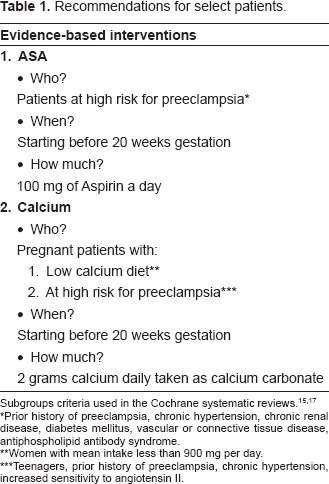
Subgroups criteria used in the Cochrane systematic reviews.15,17
Prior history of preeclampsia, chronic hypertension, chronic renal disease, diabetes mellitus, vascular or connective tissue disease, antiphospholipid antibody syndrome.
Women with mean intake less than 900 mg per day.
Teenagers, prior history of preeclampsia, chronic hypertension, increased sensitivity to angiotensin II.
Calcium
A low prevalence of preeclampsia had been reported in areas where the diet was rich in calcium. 16 This observation led to the theory that calcium supplementation may be beneficial for the prevention of preeclampsia. Numerous trials have evaluated the effect of calcium on the risk of preeclampsia, with the majority showing a non-statistically significant trend towards the reduction in the incidence of preeclampsia. However, a meta-analysis of 12 randomized trials shows benefit for both high and low risk groups 17 with an overall reduction in the risk of preeclampsia (12 trials, 15,206 women: RR 0.48, 95% CI 0.33 to 0.69). This reduction in relative risk was greatest for women at high risk for preeclampsia (5 trials, 587 women: RR 0.22, 95% CI 0.12 to 0.42), and for those with low baseline calcium intake (7 trials, 10,154 women: RR 0.36, 95% CI 0.18 to 0.70).
There is also some evidence to suggest that there may be a reduction in childhood systolic hypertension in the offspring of mothers who took calcium supplementation during pregnancy. 18 Calcium supplementation during pregnancy is simple, inexpensive, and there have been no reported side effects or adverse outcome in the mother or fetus. Therefore, selective prenatal supplementation for women with a low calcium diet (calcium consumption of less than 900 mg/day) and those at high risk for preeclampsia (prior history of preeclampsia, chronic hypertension, chronic renal disease, diabetes mellitus, vascular or connective tissue disease, and antiphospholipid antibody syndrome) may be a way to reduce the incidence of hypertension and its consequences in the mother, fetus, and next generation. The Cochrane review describes the type of intervention as: supplementation with calcium from at the latest 34 weeks of pregnancy, compared with placebo treatment. However, when looking at the majority of the studies, especially the individual 3 large studies, the CPEP, Belizan, and the WHO studies, all had women recruited at <20 wks. We therefore consider supplementation at 20 weeks to be beneficial.19–21
Still unproven (unknown, not enough evidence)
Nitric oxide
Nitric oxide is known to cause vascular relaxation and inhibit platelet aggregation, both of which are deficient in preeclampsia. This led to nitric oxide donors being entertained in the possible prevention of preeclampsia. However, a meta-analysis of 4 trials including 170 women comparing nitric oxide donors or precursors to placebo found insufficient data for reliable conclusions about the effects on preeclampsia (RR 0.83, 95% CI 0.49 to 1.41). 22 Moreover, due to the small numbers in these studies and the side effect of headaches, which led to discontinuing the treatment, more evidence using formulations with fewer side effects is needed to determine more clearly its role in the prevention of preeclampsia.
Multivitamins
Despite the fact that individual vitamins studied, such as vitamins C and E, have not been shown to affect the incidence of preeclampsia, there has been recent evidence to suggest that multivitamin supplementation in pregnancy can reduce the risk. A recent observational study of 2,951 pregnant women in Canada showed that supplementation of multivitamins containing 1 mg of folic acid was associated with a reduced risk of preeclampsia (adjusted odds ratio, 0.37; 95% CI 0.18 to 0.75). 23 However, randomized controlled trials are needed to confirm this effect and its magnitude. This may be difficult and unethical since folic acid has been proven to improve pregnancy outcome, and folic acid supplementation has been recommended to prevent neural tube defects in the neonate. These findings, however, may partially explain the recent decline in the rate of preeclampsia documented in a population based study of the incidence of hypertensive disorders of pregnancy. 24 As more widespread awareness of the benefits of preconception folate supplementation, more folate consumption may have attributed to this trend.
Antithrombotics
Heparin emerged as a possible prophylactic strategy when the placentas of preeclamptic pregnancies were found to have infarcts. There have been no randomized trials thus far that have been published on using heparin in the prevention of preeclampsia. There are a few case series and cohort studies on the effect of anticoagulation with heparin on the development of preeclampsia. These reports mainly include patients with a history of adverse pregnancy outcome or a thrombophilia.25,26 A study evaluating thromboprophylaxis with low molecular weight heparin plus low dose aspirin suggested improved pregnancy outcome in women with previous severe preeclampsia. 26 More studies are needed to confirm these findings.
Discounted as preventative option for preecplampsia
Vitamins C and E supplementation
Oxidative stress has been described in the pathogenesis of preeclampsia. There is evidence that preeclampsia is associated with decreased levels of vitamins C and E, which are known for their anti-oxidant roles. 27 This provides the rationale for using vitamins C and E supplementation in pregnancy for the prophylaxis of preeclampsia. There have been many studies28–30 evaluating the effect of different antioxidants on preeclampsia risk and are summarized in meta-analyses.31,32 These Cochrane reviews assessed different antioxidants (vitamins C, E, selenium, lycopene) alone and in combination and found antioxidants were associated with no significant decrease in the risk of preeclampsia (9 trials with a combined total of 5,446 women). This is in agreement with another systematic review that included recent large randomized trials33–35 to assess the effects of the combination of both vitamins C and E on preeclampsia and perinatal outcomes, and demonstrated no significant differences between the vitamin and placebo groups on the risk of preeclampsia.
The results of a more recent randomized controlled trial of antioxidant vitamins to prevent serious complications associated with pregnancy related hypertension in low risk nulliparous women have been published in abstract form at the 29th SMFM Annual meeting in January 2009. This study is a RCT of 10,154 low risk primiparous women from 2003–2008 and differs from previous studies in that treatment is started earlier, between 9–17 weeks of gestation, and the primary outcome is adverse outcomes associated with preeclampsia rather than its incidence. This study concluded that “therapy initiated with the antioxidant vitamins C and E prior to 17 weeks gestation in nulliparous low risk women does not reduce the frequency of serious complications associated with pregnancy related hypertension, nor does this treatment reduce the diagnosis of preeclampsia.” 36
At this point, vitamins C and E supplementation in pregnancy do not appear to prevent preeclampsia and are not recommended. In fact, it may be harmful, since one study showed that vitamins C and E supplementation were associated with an increased frequency of gestational hypertension, low birth weight, and stillbirth. 35
Fish oil
The hypothesis that fish oil could prevent preeclampsia developed from epidemiologic studies that suggested a lower incidence of preeclampsia in populations that consumed more fish. 37 This was further evaluated by multiple studies.38–40 A Cochrane review of 4 trials, involving 1,683 women assessed the efficacy of a marine oil supplement in reducing the incidence of preeclampsia. There were no clear differences in the incidence of preeclampsia (4 trials, 1,683 women: RR 0.86, 95% CI 0.59 to 1.27) between marine oil treated and control groups. 41 Therefore, fish oil is not recommended for preventing preeclampsia.
Zinc
Low maternal serum zinc levels have been found to be associated with preeclampsia.42,43 Nonetheless, a systematic review of 7 randomized trials including 2,975 women showed no significant difference in the pregnancy hypertension or preeclampsia between the zinc and no zinc groups (RR 0.83, 95% CI 0.64 to 1.08). 44
Magnesium
Some observational studies reported that magnesium supplementation might be associated with a decreased incidence of preeclampsia. Yet a meta-analysis of 2 randomized controlled trials that included 474 patients45,46 did not demonstrate any benefit of magnesium supplementation on the risk of preeclampsia. 47
Future directions
Areas of interest that are emerging and appear promising include the role of metabolic factors, angiogenic proteins, angiotensin receptor antibodies, and syncytiotrophoblast microparticles.
Metabolic factors
Metabolic disturbances, such as maternal obesity and insulin resistance, increase a woman's risk of developing preeclampsia.48,49 The mechanisms by which these metabolic derangements predispose to preeclampsia are still poorly understood. Maternal prepregnancy obesity is one of the strongest modifiable risk factors for the development of preeclampsia. There is evidence that the associated inflammation in obese patients predisposes them to preeclampsia. 50 It has also been postulated that the additive insults of insulin resistance and alteration in angiogenesis may lead to preeclampsia. 49 Further insight into the relationships between these metabolic derangements and preeclampsia may shed more light on the pathogenesis of preeclampsia. Interventions that may correct these metabolic derangements such as good glycemic control and prepregnancy weight reduction deserve further study for the prevention of preeclampsia. A randomized trial of metformin in pregnant patients with polycystic ovary syndrome demonstrated a significant reduction in pregnancy complications including preeclampsia. 51 These results appear promising, however, before metformin is prescribed throughout pregnancy for these PCOS patients, further data is necessary in regards to confirming these findings, proving its safety and providing information on follow-up of the offspring of these pregnancies.
Angiogenic proteins
A significant imbalance has been discovered between the proangiogenic (vascular endothelial growth factor [VEGF] and placental growth factor [PIGF]) and antiangiogenic factors (soluble fms-like tyrosine kinase [sFlt-1] and soluble endoglin [sEng]) in preeclampsia patients. High serum levels of sFlt-1 and sEng and low serum VEGF and PIGF have been observed in preeclampsia patients.52,53 Their pathogenic role in preeclampsia was further illustrated by the exogenous administration of sFlt-1 into pregnant rats via adenovirus mediated gene transfer resulting in increased arterial pressure and proteinuria, and decreased plasma free VEGF and PIGF concentrations similar to that observed in the preeclamptic patients. 54 VEGF infusion has also been shown to attenuate the increased blood pressure and renal damage observed in pregnant rats overexpressing sFlt-1. 55 Further research into correcting this imbalance by either blocking these antiangiogenic factors or replacing the proangiogenic factors offers potential for a preventive strategy or even a cure.
Angiotensin receptor-activating autoantibodies
Recent studies have found that women with preeclampsia have autoantibodies that activate the angiotensin receptor and result in biologic responses that are relevant to the pathophysiology of preeclampsia. 56 The introduction of these angiotensin receptor activating antibodies into pregnant mice resulted in classic features of preeclampsia including hypertension, proteinuria, and increased production of sFlt-1. 57 It has recently been demonstrated that these autoantibodies can be blocked by a 7-amino-acid peptide, and thus may provide an opportunity to prevent this disease. 57
Syncytiotrophoblast microparticles
In preeclampsia there has been found to be increased circulation of syncytiotrophoblast-derived debris compared with normal pregnancy. 58 These microparticles may play an important role in stimulating the systemic inflammatory response. In-vitro preparations of trophoblast microparticles have been demonstrated to lead to an antiangiogenic state that would contribute to the clinical features of preeclampsia. 59 Further research is required to determine the role of these microparticles in the pathogenesis of preeclampsia, and possible interventions that may block their effect, thereby preventing this disease process.
Genomics, proteomics, and matabolomics
Studies evaluating the genetics, proteomics, and metabolomics of different disease processes have been reported and appear promising. As the development of preeclampsia appears to involve several different mechanisms, the use of these data-generating approaches has the potential to contribute significantly to future research in preeclampsia and aid in our understanding of this condition. This may, in turn, offer opportunities for new diagnostic and preventive strategies.
Conclusions
Although the interventions for the prevention of preeclampsia thus far are still imprecise, it has not been a complete disappointment. There has been significant progress made. Further research into the pathogenesis of preeclampsia is needed, as this will offer more opportunities in finding effective preventative strategies. We advocate the next wave of research to focus on better understanding the pathophysiology of preeclampsia at the cellular level. Funding these areas of research may be more cost effective than universal implementation of interventions that are of minimal benefit. As preeclampsia is a multifactorial disease process, multidisciplinary and collaborative research between different disciplines, and between basic and clinical researchers, is highly recommended. Also, collaboration with the pharmaceutical industry, along with other potential partners, may help develop novel therapeutic strategies to prevent preeclampsia. The preventive interventions that have already been studied may need to be reexamined from different aspects. This includes identifying what specific subgroups may benefit more from each strategy. Reexamination of previous strategies should also include earlier timing of the intervention than in past trials. In most previous trials the interventions were later in pregnancy than the early placentation period, and thus may have been too late for the intervention to show a benefit. It would also be beneficial to fine tune drugs that already work in terms of formulations, dosing, and see what effect their combination may have, such as ASA and calcium. Further research into nitric oxide and folic acid would also be of interest.
Conflict of Interest
There are no conflicts of interest for either of the authors.