
Abstract
Objective
The aim of this study is to assess women's awareness of the benefit and use of folic acid during pregnancy and to assess whether their knowledge has improved following hospital visits.
Method
This is a prospective survey conducted in a large teaching hospital in the UK. The survey questionnaire consisted of 28 questions about demographic variables, behavioral variables, and knowledge about folic acid and neural tube defects (NTDs).
Result
A total of 603 women participated in this study. Some of them attended for the first time and others had more than one visit, either in their current or previous pregnancies. In about 25% of cases, the pregnancy was not planned. Between 14 and 19% of the women of First and Two+ Visit groups consulted their doctor or other healthcare professional before conception. Nearly 98% of the women stated that they had heard of folic acid, but only 42–52% knew the medical condition it protects against. The main sources of information for women who were aware of folic acid were midwives and general practitioners. Nearly 90% of women who attended their first antenatal visit were taking folic acid. However, only 40% of women knew that they should take it before pregnancy, and only between 36 and 46% knew the dietary sources of folic acid, although about 84% know the foods that should be avoided during pregnancy. This study found that attending antenatal clinic has not increased women's awareness about folic acid.
Conclusion
There is still a high proportion of women who do not know that folic acid should be taken before pregnancy and continued for the first three months of pregnancy. School education, primary care team, and family planning service should take the lead in providing information to women about folic acid.
Introduction
Neural tube defects (NTDs) are among the most common birth defects resulting in infant mortality and serious disability, with around 500 pregnancies being affected in England and Wales each year. 1
Numerous countries including the UK recommend that all women planning to become pregnant should take 400 μg per day of folic acid for at least one month prior to conception and for up to 12 weeks postconception. This recommendation was based on the findings of the Medical Research Council Vitamin Study Research Group in 1991 that periconceptional folic acid intake reduces the risk of NTDs.2–4
In the UK, a campaign was launched in 1995 by the Health Education Authority (HEA) to improve folate status awareness in women. The three-year campaign also aimed to target health and other professionals, such as teachers and journalists. 5
Various studies around the world have investigated the understanding of the importance of folic acid among women of child-bearing age, with some identifying associations between demographic and lifestyle variables with folate uptake.6–10
To our knowledge, there have been no surveys conducted to date to determine any differences in the understanding and use of folic acid among women before and after they had attended their first antenatal ultrasound scan (before seeing any midwife and after seeing the midwives).
Objective
The aim of this study is to investigate the awareness and use of folic acid in women before and after their antenatal visits to assess whether antenatal care provides appropriate information about folic acid and other nutrition.
Methods
During July 2013, a survey was conducted in the Jessop Wing Maternity Services of Sheffield Teaching Hospitals in Sheffield, UK. The survey included all women who came to attend for an ultrasound scan at the antenatal clinic. Women have the booking scan before they attend their first antenatal booking clinic. They then come at 20 weeks gestation for an anomaly scan and some attend later in pregnancy for a growth scan where indicated. A questionnaire was distributed to all women attending for a scan, of which some would have their first scan and others would have attended previously.
In the UK, pregnant women were offered an early ultrasound scan between 10 weeks 0 days and 13 weeks 6 days, usually named a dating scan, to determine gestational age, detect multiple pregnancies, and screen for Down's syndrome by assessing nuchal thickness. 11 In an uncomplicated pregnancy, this will be a woman's first visit to the antenatal clinic. Till then, a healthy primigravida will only have been seen by her general practitioner (GP) or midwife unless there was any medical or obstetric concern.
Furthermore, it is also a guidance that ultrasound screening for fetal anomalies should be routinely offered, usually between 18 weeks 0 days and 20 weeks 6 days. 11 In this study, a 10-minute questionnaire (see Appendix 1) was distributed with a covering letter detailing the purposes of the study (see Appendix 2). Women were asked to complete it while waiting to be called for their scan. Upon completion, they were asked to return the questionnaire in the provided envelope and were subsequently given an information leaflet highlighting all relevant information on the benefits and use of folic acid, as well as other general pregnancy health advice and other information intended to ensure that no undue fear or anxiety was caused by completing the survey. Prior to distribution, the questionnaire was checked by numerous senior members of the obstetric team to ensure that such a scenario would not occur and for intelligibility of the questions.
A trained second-year medical student collected the completed anonymous surveys and separated them according to the answer given to question 2 regarding whether this was the women's first visit or they had attended an antenatal ultrasound scan previously. This allowed two distinct groups to be created: a “First Visit” group, and a “Two+ Visit” group, allowing direct comparison to establish any differences in the understanding and use of folic acid following antenatal clinic attendance.
The questionnaire consisted of 28 questions about demographic variables (age, education level, obstetric history, malformations during pregnancies, usage of contraception, and initial contact with a healthcare professional in the current pregnancy) and behavioral variables including the use of folic acid, the sources of information regarding folic acid, knowledge about folic acid, and NTDs. For the majority of the questions in the survey, the answers were predefined.
The questionnaire was split into two segments: the first being details about the participant and the second being questions about folic acid. Question 12 (see Appendix 1), the first question in the second segment, asked whether the participant had heard about folic acid. If the answer given was “Yes,” they were asked to kindly continue with the remainder of the questions. If “No,” they were asked to skip to a point further in the survey, which did not assess the understanding of folic acid, as this was deemed not necessary. Our questionnaire was adapted from Bitzer et al's study. 12
Results
In total, 603 women completed the survey, of which 195 had come for their first visit and 408 had previously attended an ultrasound scan appointment. Of the returned survey questionnaires, some were not fully completed as some questions were left blank. Furthermore, some women were unable to complete the questionnaire because of lack of English proficiency. Unfortunately, we did not have the resources to provide an interpreter. Table 1 provides the demographic characteristics of the women in both groups.
Demographic characteristics of the women.

Obstetric history and conception
In the First Visit group, 26.4% of the women stated that this pregnancy was unplanned, which is very similar to the 26.3% in the Two+ Visit group. Of the First Visit group, 14% reported that they consulted their doctor or other healthcare professional before conception. This is comparable to the 19% in the Two+ Visit group.
Results for women with planned pregnancies who had stopped their contraceptive method without consulting their doctor or other healthcare professional and women who did not use contraception were similar between the two groups, with the First Visit group being slightly higher for both answers (29% compared to 24.9% for stopping their contraception, and 28.5% compared to 25.2% in women who used no contraception). The remaining women in the Two+ Visit group who answered this question (4.5%) did not recall their behavior at that time point, compared to 2.1% in the First Visit group.
Awareness and use of folic acid
Overall, in the First Visit group, 97.4% of the women stated that they had heard of folic acid (Table 2), and for the question: “Which medical conditions it protects against?” 51.9% of the answers were given as spina bifida (Fig. 1). Furthermore, a total of 11.9% of answers were given for anemia, autism, and Down's syndrome (Fig. 2). This is in contrast to the Two+ Visit group in which 42.8% of the answers identified spina bifida as having a known link. Despite a high response of 98.5% having heard of folic acid, the answers given as “I don't know” were higher; 34.2% in the Two+ Visit group compared to 26.6% in the First Visit group.
Knowledge and awareness of folic acid.

Where the assumptions were met, a Chi-squared analysis was performed. In all other cases, the P-value for the Fisher's Exact test is presented.
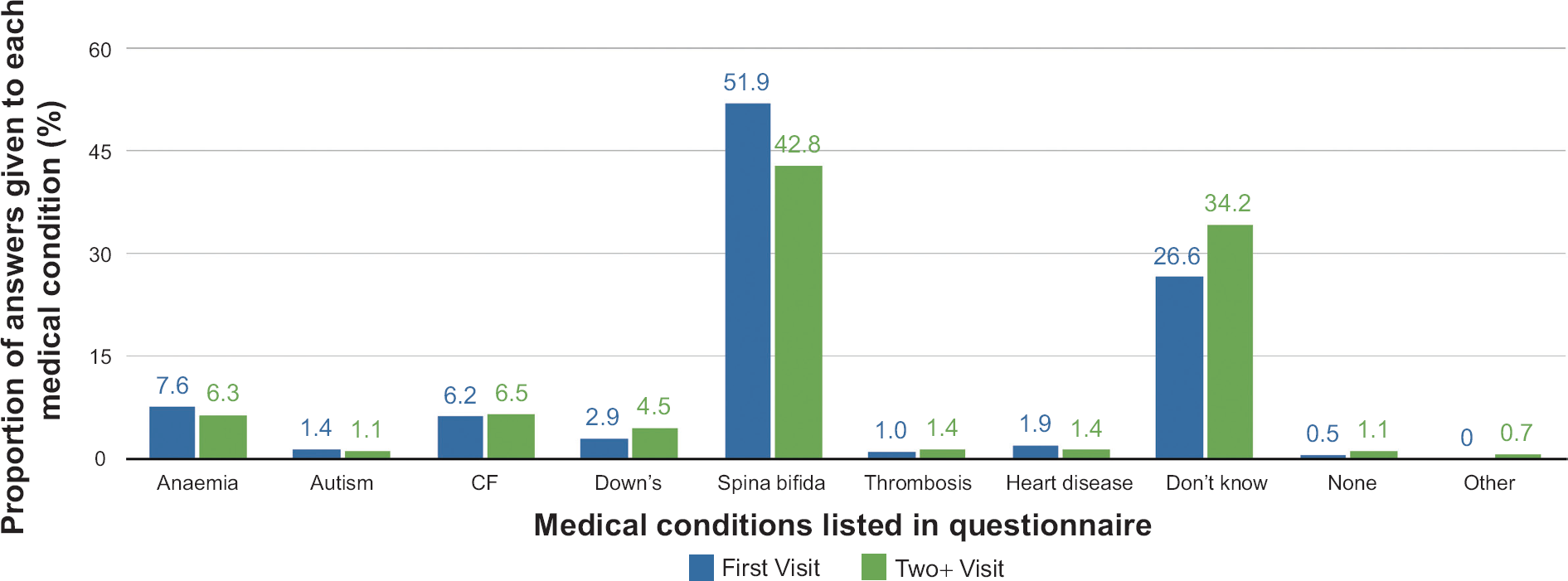
Proportion of answers given by women in each group when prompted to identify which of the listed medical conditions in the questionnaire had been shown to be protected against by the use of folic acid.
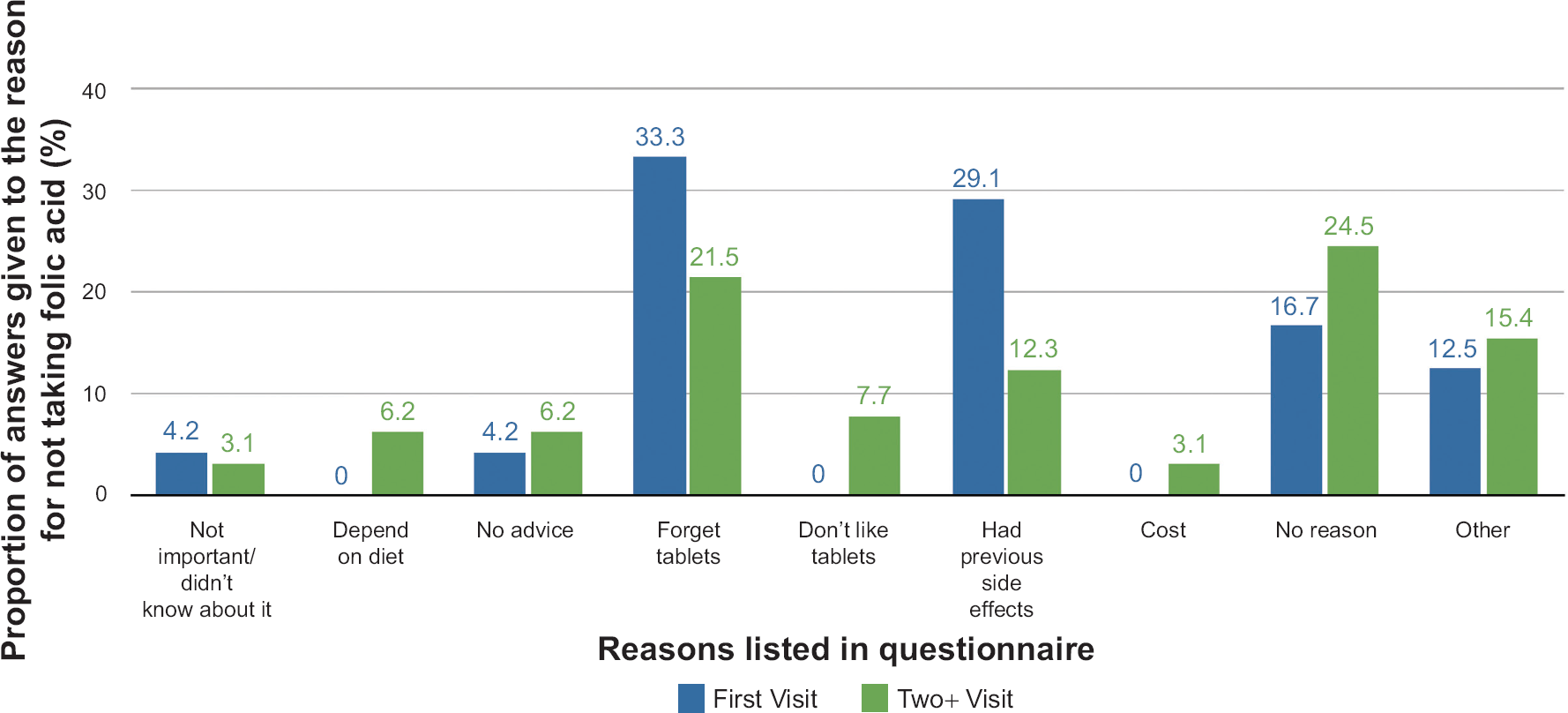
Proportion of answers given by women in each group when prompted to give a reason why they do not take folic acid.
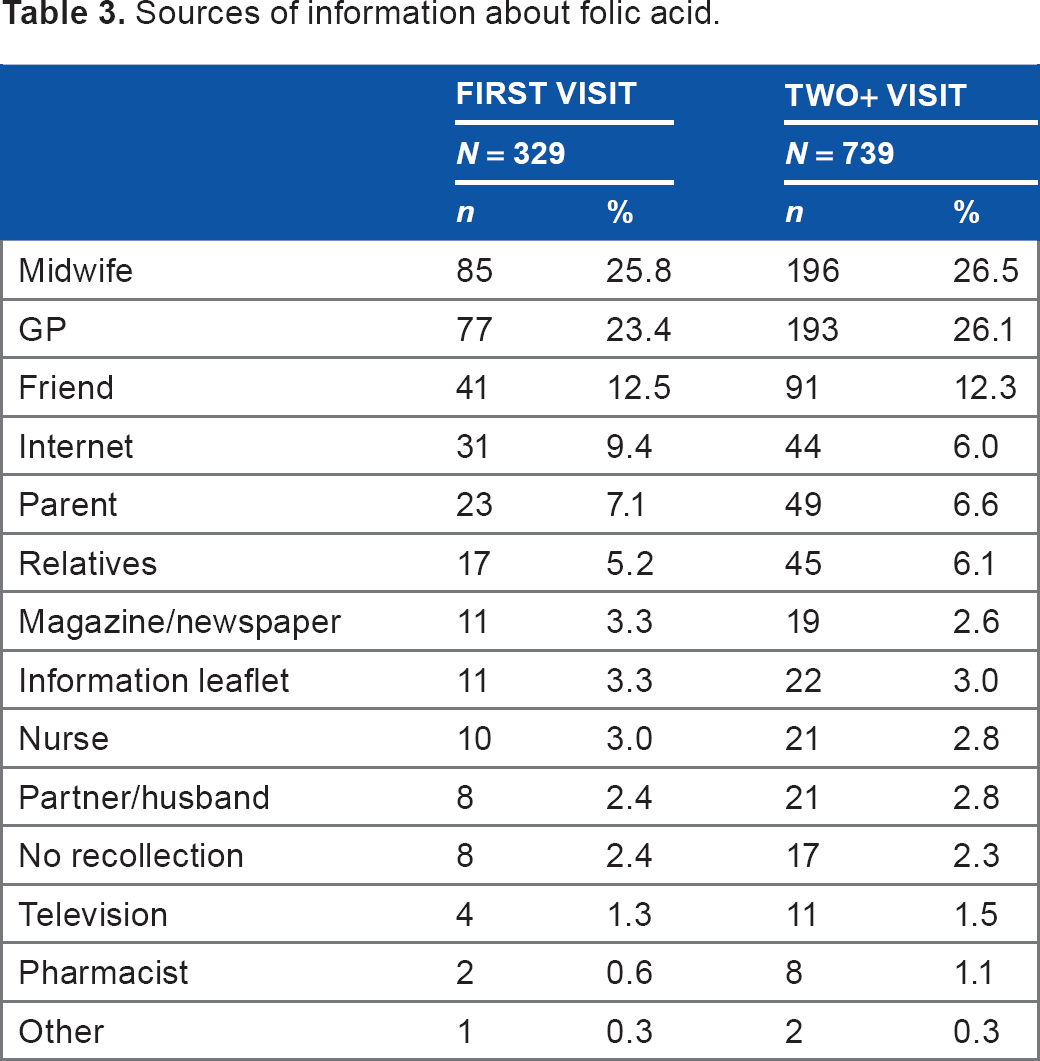
In both groups, of the women who were aware of folic acid, the main sources of information were midwives and GPs (Table 3).
Sources of information about folic acid.
When considering the time points at which the women became aware of folic acid, the results showed no significant difference between the two groups with 42.9 and 44.9%, reporting the time when they were planning to conceive, and 47.9 and 42.2%, reporting the time when they conceived, in the First Visit and Two+ Visit groups, respectively (Table 2).
A greater proportion of 89.7% of women in the First Visit group reported taking folic acid supplements at the time of the survey compared to 57.2% in the Two+ Visit group, which is explained by being further advanced in pregnancies; however, the results were similar between the two groups with regard to their sources of folic acid supplements with a supermarket or a shop being the most common source. Of the women who answered “Other”, some of the sources given included midwives at the Children's Centre, nutritionist, and online stores. A very high percentage of 96.6 and 94.3% in the First and Two+ Visit groups, respectively, answered that folic acid is taken once a day (Table 2).
When questioned on their understanding of when they are supposed to start taking folic acid, both groups had similar results with “Before getting pregnant” and “Before and during pregnancy” with roughly 40% of the replies in each group, and 18.0 and 22.3% in the First and Two+ Visit groups, respectively, replied as “During pregnancy”. Similarly, when questioned when they are supposed to stop taking the supplement, majority results of between 65 and 70% in each group correctly identified as “After the first three months of pregnancy (12–14 weeks)”. However, 22.1% in the First Visit group answered “I do not know” compared to 16.2% in the Two+ Visit group (Table 2).
The two groups showed similar results when asked how many times per week they forgot to take their folic acid supplement, with around two-thirds (64.5 and 61.3%) answering zero, and 29.5% in both groups answering one to two times per week (Table 2).
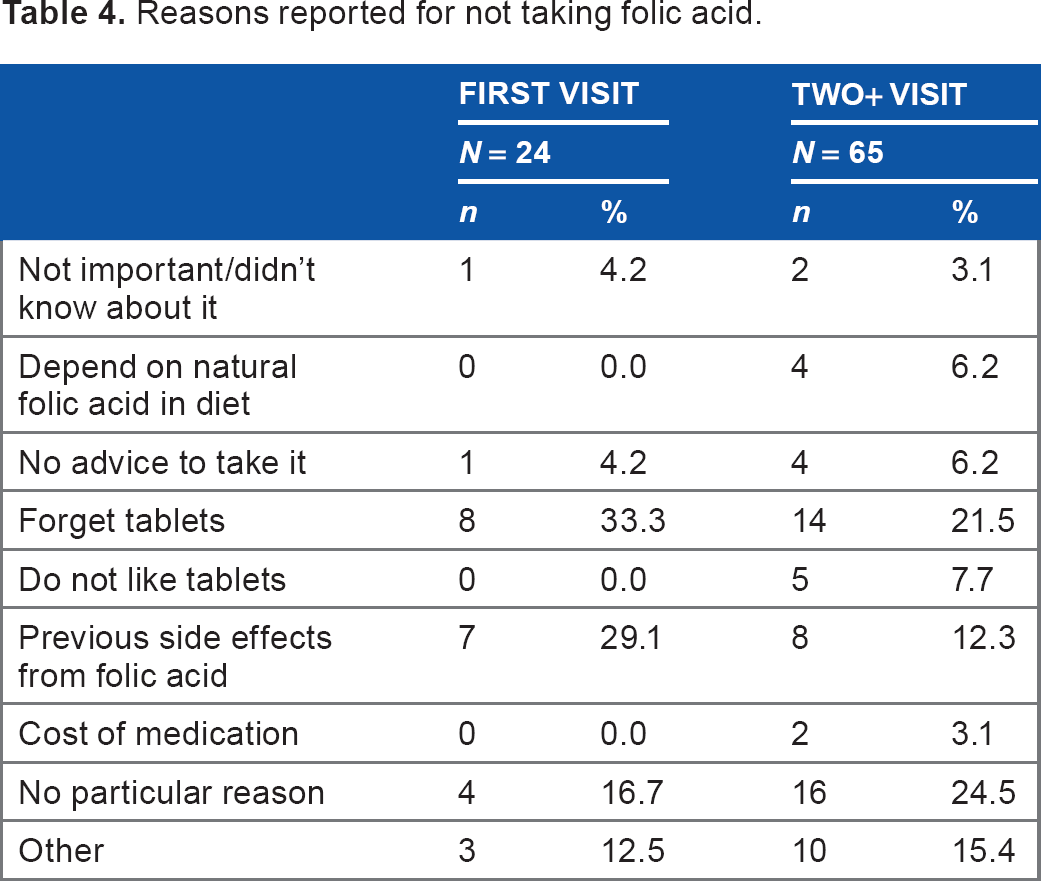
Of the women did not take folic acid, when asked why they did not take folic acid the most common answer in the First Visit group was that they forgot to take the tablets (33.3%) followed by having previous side effects from the supplement (29.1%). This is in contrast to the Two+ group's most common answer of “No particular reason” (24.5%) followed by forgetting tablets (21.5%) (Table 4). Of the women who answered “Other”, reasons given included not being aware of pregnancy before the first trimester, conflicting advice and information given by different healthcare professionals, and having previous healthy children without taking folic acid so did not see the point of taking supplements in current pregnancy.
Reasons reported for not taking folic acid.
Knowledge of food rich in folic acid was also assessed. A total of 36.6% of the First Visit group could correctly identify any source of food rich in folic acid (green vegetables, cereals, liver, fish, citrus fruits, and yolk) compared to 43.9% of the Two+ Visit group. Then, when prompted to list foods that should be avoided during pregnancy, 83.1% of the First Visit group and 80.3% of the Two+ Visit group could identify any food such as soft, unpasteurized cheeses, raw or lightly cooked eggs, cold cured meats, foods high in vitamin A such as liver, liver products like pâté, some types of fish, unpasteurized milk, or peanuts.
Discussion
We wished to compare the understanding and use of folic acid between women who had not attended their first antenatal clinics with the ones who had done previously. Any differences that were observed could at least be partly resulting from information and advice they had gained during their appointment.
Only 40% of women in this study knew that folic acid should be taken at least one month before pregnancy and only between 36 and 46% of women knew the dietary sources of folic acid. Our study found that antenatal clinic visits have not improved women's awareness about folic acid. In fact, following this study, we discovered that we do not have any information leaflets about folic acid in the clinic, and midwives and doctors do not usually discuss this in the clinic. We have recently updated our information leaflets to pregnant women and added folic acid and other nutritional information to the leaflets.
Although there has been a significant overall mean reduction of 32% in the prevalence of NTDs in the UK over a 10-year period up to 1999, 13 the expectations of a 72% reduction estimated by a Cochrane review of five clinical trials had not been met. 14 The contributory factors for these are the high number of unplanned pregnancy (25% in our study compared to 38% in Bitzer et al's study), low percentage of women (40% in this study) knowing that they should take folic acid at least one month before pregnancy, and lack of compliance to daily dose (about 30% in this study compared to 37–44% in Bitzer et al's study.) 12
Preconceptional counseling about the value of folic acid should be integrated in the school sex education and into family planning consultation either at the Primary Care Team or the dedicated family planning services. Folate-fortified oral contraceptive pills might also play a part in reducing the incidence of NTDs.
Limitations
A few points need to be considered in the interpretation of the results. We discovered from the results and comments given by the women that the choice of wording of some of the questions in the survey resulted in some confusion. Question 17 (see Appendix 1) asked “Do you currently take folic acid?” There was a significantly higher result in the First Visit group; however, the result does not give clear indication as to whether the women who answered “No” took folic acid previously in the pregnancy. However, it is expected that the proportion of women in the First Visit group taking folic acid will be significantly higher than Two+ Visit group, because the majority of the latter group will be beyond 12 weeks gestation. Both groups had a clear majority answer of over 65% knowing that folic acid supplements are usually stopped after the first trimester. These women may well have passed their first trimester at the time of completing the questionnaire, especially those in the Two + Visit group. Possibly, the question should have rather asked whether the women had taken folic acid during their current pregnancy, and not necessarily at the time of answering the survey. This may also explain the low response rate for question 24 regarding the reasons why they did not take folic acid. Only 24 and 65% of women in the First and Two+ Visit groups, respectively, gave an answer to this question, although it would be expected that the response rate would be close to the values for individuals who answered “No” to questions 17 and 12.
Furthermore, since the Two+ Visit group would have invariably been further along in their pregnancy than the remaining women, there may have been an element of recall bias in remembering some of their behaviors and interactions at the start of their pregnancy, such as what they did when making plans to become pregnant (see question 10, Appendix 1).
Women were divided to two groups based on their answer to question 2: “Is this your First visit, Second visit, More?” Women answering “First Visit” were allocated to the First Visit group and the others to the Two+ Visit group. An issue in this allocation was that some women with previous pregnancies answered “First visit,” understanding that the question meant their first visit in their current pregnancy, whereas some gave another answer thinking that the question meant if they had ever had an appointment in the past, although for their current pregnancy they were attending their first scan. We believe that the question should have been much clear to assess attendance for which visit in the current pregnancy. This might have diluted the differences between those who previously exposed to antenatal care and those who have not.
On completion and return of the questionnaire, women were given an information leaflet detailing various aspects of folic acid and its protective abilities. Some women then left this leaflet on the tables in the waiting room of the clinic where the questionnaire was carried out. This could have been a factor of confounding if a different woman later on saw it and read the information before answering the questions in the survey.
Conclusion
There is still a high proportion of women in the UK who do not know that folic acid should be taken before pregnancy and should be continued for the first three months into pregnancy despite the campaign which was launched in 1995 by the HEA to improve folate status awareness in women. This has not improved even after visiting antenatal clinics. Our study as well as other recent published papers on the same subject endorses the idea that women should receive both verbal and written information about folic acid during their school sex education, when attending to discuss family planning at the family planning service or their own GP and during their antenatal visits. Questions about folic acid should also be integrated in the medical history taking in all women during their reproductive period.
Supplementary Data
Appendix 1
The full text of the questionnaire distributed to study participants.
Appendix 2
The full text of the covering letter distributed with the questionnaire, detailing the purposes of the study.
Author Contributions
Conceived and designed the experiments: RK. Analyzed the data: MM, RK. Wrote the first draft of the manuscript: MM. Contributed to the writing of the manuscript: RK. Agree with manuscript results and conclusions: RK. Jointly developed the structure and arguments for the paper: RK, MM. Made critical revisions and approved final version: RK. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgments
Authors would like to thanks Ms Kathleen Baster from the statistical Department at the University of Sheffield for her help in the statistical analysis.