
Abstract
As with all surgical specialties, gynecologists and obstetricians routinely employ surgical interventions, depending on the exact nature of the problem that they are treating. Surgery is the mainstay of gynecological therapies, and in obstetrics, surgery is frequent.
Most Frequent Surgeries in OB/GYN and their Incidence
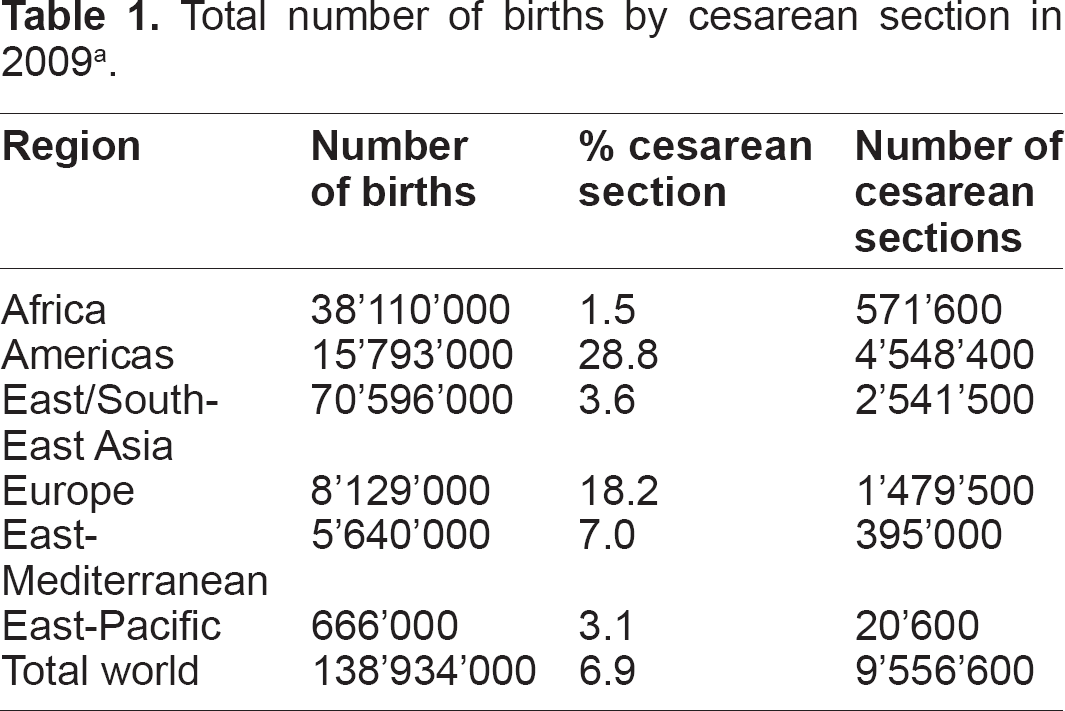
The worldwide prevalence of cesarean sections among medically-attended births is around 12% with great variations noted across different regions (for example, the prevalence rate varies from 3.3% in Africa to 31% in the Americas, and even 34% in the East-Pacific region). 1 The percentage of cesarean sections across total births (medically-attended and non-medically-attended) is approximately 7%, suggesting that the total number of such interventions in one year would approach 10 million worldwide.
Episiotomy is another common practice in obstetrics. A recent Cochrane study on episiotomy for vaginal births 2 states that episiotomy has become one of the most commonly performed surgical procedures in the world, in spite of having been introduced without strong evidence of its effectiveness. 3 The incidence of episiotomies varies widely depending on the country, ranging from 8% in the UK 4 to 15% in Australia, 5 25% in the USA, 6 67% in India, 7 and up to 95% in Brazil. 8 These numbers appear to be decreasing every year.6,9
In gynecology, hysterectomy is undoubtedly the most common surgical procedure, and probably the most common non-pregnancy-related major surgery performed on women. Its prevalence is variable from one region to another and also between countries of the same region. Although its occurrence is decreasing year after year, the hysterectomy rate remains high in the USA, 10 with 5.1 per 1,000 women undergoing this procedure in 2004, totaling 600,000 hysterectomies per year. Rates are usually lower in other countries; for instance, 4.4 per 1,000 women undergo the procedure in Chile, 11 while between 1.2 per 1,000 women in Norway and 2.8 per 1,000 women in the United Kingdom undergo the procedure.12,13 Similarly, as low as 1.2 per 1,000 women in India,14,15 and 1.0 per 1,000 women in Japan have a hysterectomy. 16 Interestingly, other gynecological surgeries account for a much smaller proportion of the total surgical procedures performed.
Total number of births by cesarean section in 2009a.
Types of Abdominal Incisions in OB/GYN Surgeries
Several types of vertical abdominal incisions have been used in gynecologic surgery, including midline, paramedian and wide paramedian incisions. A midline incision is almost exclusively used in gynecologic oncology surgery.
Several useful transverse abdominal incisions are also available to the surgeon performing gynecologic surgery. Historically, the obstetrician/gynecologist (OB/GYN) has preferred this type of incision. Reported advantages include better cosmetic results, less pain, and a low incidence of hernia formation. Gynecologic oncologists have embraced certain types of transverse incisions for specific gynecologic cancer operations. Several disadvantages also exist, such as a limitation in the exploration of the upper abdomen, or greater blood loss among patients; moreover, patients who receive this type of incision are more prone to hematoma formation when compared with patients who receive a midline incision.
Pfannenstiel incision is probably the most commonly used, but the Maylard incision, Cherney incision, or modified Gibson incision also deserves mention.
Process of Wound Healing and Scarring—Keloid and Hypertrophic Scars
Cutaneous scarring is inevitable following damage to more than 33% of the thickness of the skin either through trauma or surgery. 17 A cutaneous scar is defined as dermal fibrous replacement tissue and results from a wound that has healed by resolution rather than regeneration. 18 Final appearance is largely influenced by the interval between wounding and complete healing. 19 Once a scar has formed, it undergoes several distinct macro- and microscopic changes during the maturation process; this process is completed (on average) after one year. 20 The classic steps of wound healing are hemostasis, inflammation, angiogenesis, epithelialization, fibrogenesis, and remodeling.
Excessive scars form as a result of aberrations of physiologic wound healing and may develop following any insult to the deep dermis, which can result from surgical procedures. By causing pruritus, pain, and contractures, excessive scarring can dramatically affect a patient's quality of life, both physically and psychologically. There are two types of excessive scars that can result from trauma to the skin: hypertrophic scars (HS) and keloids (KL). Per their definition, both scar types rise above skin level, but while HS do not extend beyond the initial site of injury, KL typically project beyond the original wound margins. 20 Hypertrophic scarring usually occurs within 4 to 8 weeks following injury, 21 has a rapid growth phase for up to 6 months, and thereafter gradually regresses over a period of a few years, eventually leading to flat scars with no further symptoms. 22 KL, in contrast, may develop up to several years after minor injuries and may even form spontaneously in certain predisposed individuals. Both lesions are commonly pruritic, but KL may be a source of significant pain and hyperesthesia. 21 In the majority of cases, HS develop in wounds at anatomic locations with high tension.
Histologically, both KL and HS contain an overabundance of dermal collagen. The occurrence of KL and HS has an equal gender distribution and the highest incidence is noted in the second to third decade.23,24 Incidence rates of hypertrophic scarring vary from 40% to 70% following surgery, and up to 91% following burn injury, depending on the depth of the wound.25,26 KL formation is seen in individuals of all races, except albinos, but dark-skinned individuals have been found to be more susceptible to KL formation, with an incidence of 6% to 16% noted in African population.27,28 The concept of a genetic predisposition to KL is strongly suggested because patients with KL often report a positive family history, unlike patients suffering from HS.
Regarding the pathophysiology of KL and HS, there is obviously a key role played by an anarchic and prolonged release of various cytokines, especially transforming growth factor-β (TGF-β), the level of which is significantly increased in patients with proliferative scars when compared to control patients. 29 Significant elevations of PDGF,30,31 VEGF,32,33 interleukin-1 (IL-1) and interleukin-6 (IL-6) 29 are also noted in patients with these scars. Interestingly, the production of these cytokines is under the strong influence of reactive oxygen species (ROS).34–38 All these data would argue in favor of early preventive management of HS and KL with topical and/or oral antioxidants.
Hypertrophic and Keloid Scars in OB/GYN
A paper published in Japan considered 446 women having undergone caesarean sections, and reported an incidence of 30% of HS observed 3 months after the operation. 39 In another study conducted in Thailand, 40 the authors focused on the comparative incidence of hypertrophic caesarean section scarring: of the total number of patients, 77% had HS formation; In another prospective study conducted in Canada, 41 postsurgical adhesions and KL were evaluated in 429 women of different races after caesarean delivery. Compared with Caucasians (0.5%), KL were significantly more common in African Americans (7.1%) and Asians (5.2%), which is in line with the current knowledge that KL is more likely to develop in individuals with darker skin.
A study conducted in Kenya 42 sought to compare the occurrence of HS after caesarean section performed with the Misgav-Ladach (ML) procedure vs. the traditional procedure. After a 6-week follow-up, the presence of HS was found to be significantly associated with the traditional procedure (48.8%) more than with the ML technique (2.1%). Moreover, in Africa, a thesis 43 focused on the different types of sutures used after caesarean sections, and the authors reported that 8.6% of patients presented with KL, while 7.4% of patients developed HS after caesarean section. To further support these findings, in Australia, a paper reported an occurrence of HS in 41% of patients at 12 weeks post caesarean section. 44
It is beyond any discussion that an episiotomy scar can be a source of altered body image. The size of the episiotomy scar may be disproportionate to the impact it has on a woman's body image. 45 In one particular study, it was found that every fifth woman thought that her vagina and perineum was disfigured by the episiotomy scar. 46 In another trial comparing a chromic vs. a PGA suture in episiotomy repair, 47 a noticeable scar was present in all patients with the chromic suture vs. only 57% in the PGA group. In spite of a thorough investigation, we did not find any mention in the literature of a study conducted assessing the incidence of HS and KL following episiotomy.
Surprisingly, when searching Medline we were unable to find any relevant data regarding the occurrence of such pathological scarring following hysterectomy. Nonetheless, given the similarity of incisions practiced in both caesarean sections and abdominal hysterectomies, we can deduce that the prevalence of KL and HS following these surgeries should be similar.
An anecdotal case report of an umbilical keloid occurred after laparoscopically assisted vaginal hysterectomy has been published. 48
Female genital mutilation (FGM) is not an OB/GYN surgery, but it could be considered to fall within the same gynecologic sphere. For this reason, the occurrence of KL and HS after FGM deserves to be mentioned in this review. The World Health Organization (WHO) estimates that between 100 and 140 million girls and women worldwide have been subjected to one of the first three types of FGM. 49 Obviously KL and HS are one of the multiple physical and psychological consequences for women suffering from FGM, and are usually located on the vulvar wound. Various studies have intended to establish the rate of keloid scars following FGM. Prevalence rates range between 7% in Mali, 50 30% in the Kilimanjaro area of Tanzania, 51 and have reached as high as 62% in Burkina Faso 50 and Sierra Leone. 52
Prevention of Hypertrophic and Keloid scars during Gynecological Surgeries
Prevention of pathologic scarring is undoubtedly more effective than any treatment. Thus, avoiding all unnecessary wounds in any patient, whether or not the patient is prone to KL and/or HS remains an obvious but imperfect solution. 53 Meticulous surgical techniques can reduce the formation of KL and HS; however, they cannot prevent all cases.
The technique of incision is of importance, and some authors report a better outcome for HS prevented with a wedge-shaped incision instead of the conventional vertical incision. 54
The site of incision is also a key concern: incisions should be made so that they follow skin creases and surgeons should avoid incisions that cross joints whenever possible. At this stage, Langer lines, which describe the orientation of dermal fibers within the skin, must be taken into account whenever possible. In the abdominal wall they are arranged in a primarily transverse orientation. Obviously, midline or paramedian incisions sustain more lateral tension and thus in general develop more KL/HS than incisions following Langer lines. On the contrary, transverse incisions such as Pfannenstiel's, Cherney's, Maylard's, or Joel-Cohen's cause less tension on the opposing wound edges due to the fact that they follow Langer lines, reducing the risk of developing KL/HS. It was recently demonstrated that mechanical force such as stretching/contraction of the skin is an important trigger that drives keloid generation even in patients who are genetically predisposed to KL. 55 In caesarean sections, the occurrence of KL in black women (who are naturally prone to hypertrophic scarring) was found to be dramatically reduced when using the Misgav Ladach technique as compared to the Kerr's method (2% vs. 49%). 42
The closure technique is also an important issue that should be considered. An evidence-based review of the literature published in 200556 concluded that the most effective method of midline abdominal closure was mass closure, as it incorporates all the layers of the abdominal wall (except skin) as one structure. However, this study did not contemplate the possible occurrence of KL/HS. In an evaluation of buried vertical mattress sutures used in 149 patients, 57 the cosmetic results were excellent to good in 78.5% of patients, while HS was present in 10% of patients, and keloid formation was noted in 1.3%, making it a good alternative for the prevention of KL/HS. Consecutive modifications of this buried vertical mattress suture were described, with better results achieved when compared with conventional bi-layered techniques (2% vs. 16% HS and KL formation, respectively); 58 this effect was most pronounced when use of the sutures was combined with wedge-shaped excisions. 54 The length-control suture (LCS) technique, in which a suture is passed in a closed-loop beneath the wound and anchored to the underside of the dermis, thereby pulling the apices of the wound inwards, was designed to minimize lengthwise forces and tension. The result was unquestionable 6 months after surgery as the scar was thin, soft, and flat in 97% of patients who submitted to this suture technique. 59 Progressive tension suture (PTS), which is practiced daily in aesthetic and plastic surgery following abdominoplasty, also appears to be effective at avoiding tensions on the terminal suture lines, which tend to favor KL/HS formation.
Obviously, close attention must also be paid to the choice of suture materials. A suture is any strand of material used to approximate tissue or ligate vessels. Various materials have been used for sutures throughout history; nonetheless, the ideal suture has not yet been invented. The main qualities of a good suture include being comprised of material with uniform tensile strength, knot security, non-allergenic properties, and good tolerability, and that have high tensile-strength retention during wound healing.
Sutures are usually classified as absorbable and non-absorbable. Absorbable sutures are prepared from the collagen of animals or synthetic polymers and are eliminated from the body by enzymatic action or hydrolysis. Absorbable sutures also have limitations. For instance, the absorption in some individuals may accelerate and lead to premature diminution of tensile strength. The absorbable sutures commonly used in OB/GYN practice are surgical guts or sutures that are elaborated from synthetic polymers such as polyglactin 910, polyglycolic acid, poliglecaprone, polydioxanone, and polyglycinate.
Non-absorbable sutures are not digested through enzymatic activity or hydrolysis. They are composed of multiple filaments of metal, synthetic, or organic fibers fashioned into a strand by twisting, braiding, or spinning. The most commonly used are natural (silk or cotton), stainless-steel wire (Flexon®), nylon, polypropylene, or braided synthetic sutures.
The possible occurrence of KL/HS may depend on the suture material used by the surgeon. Disregarding cosmetic outcomes, the previously mentioned evidence-based review that aimed to find the best abdominal closure concluded that number 1 or number 2 absorbable monofilament suture materials were optimal. 56 When keeping in mind the possible occurrence of KL/HS following surgery, should we use absorbable or non-absorbable sutures? After surgical wound repair in the occipital region during rhytidectomy using absorbable or non-absorbable suture materials, there was no statistically significant difference in the incidence of KL or HS between both groups. 60 In a similar study conducted on presternal scarring, 61 monofilament nylon sutures were shown to diminish the risk of hypertrophic scarring; on the contrary, in skin closures of laparotomy wounds (a common gynecological surgery), an absorbable subcuticular suture appeared to yield better results in terms of KL/HS formation than interrupted non-absorbable sutures. 62 This trend was confirmed in orchidopexy wounds sutured with subcuticular polyglycolic acid, where hypertrophy was less likely to occur after the use of interrupted black silk sutures. 63
A priori, absorbable sutures appear to be the best option in abdominal wound closure in term of prophylaxis of KL/HS. In the literature, Dexon®, a polyglycolic acid absorbable suture, was particularly scrutinized. While no increase in HS formation was found following the use of a Dexon® intracuticular suture in pediatric orthopedic surgery, 64 an increased incidence of HS was observed in paramedian and inguinal wounds 65 and in caesarean sections 42 sutured with Dexon®. There was no statistically significant difference in the occurrence of KL/HS when polyglactin 910 (Vicryl®) was used in comparison with polydioxanone (Quill®). 66
In breast reduction patients, Monocryl®, a monofilamentous absorbable poliglecaprone suture, resulted in fewer HS formations compared with Vicryl®, a multifilamentous suture, sustaining the opinion that a monofilamentous suture should be used over a multifilamentous one. 67 On the other hand, use of a non-absorbable polybutester suture (Vasufil®) was found to diminish the risk of hypertrophic scarring when compared to the use of nylon sutures when closing wounds from a midline laparotomy. This was thought to be due to the polybutester suture's special properties, allowing it to adapt to changing tensions in the wound. 68
Finally, a discussion of the use of stitches must not be avoided. In a study comparing the cosmetic outcomes (including scar hypertrophy) at 6 and 12 months following lower midline laparotomies, the outcomes were significantly better using interrupted Donati stitches vs. running nylon skin sutures. 69
Prevention of Hypertrophic and Keloid Scars in the Follow-up of Gynecological Surgeries
Among current strategies, pressure therapy has been the preferred conservative management for both the prophylaxis and the treatment of HS and KL since the 1970s; however, there is little scientific evidence supporting their usefulness. 70 The mechanism of action of pressure garments is poorly understood, but it may be attributable to the limiting of a patient's supply of blood, oxygen, and nutrients to the scar tissue. 71 However, compression therapy is ultimately limited by the inability to adequately fit the garment to the wound area, and by patient discomfort, which frequently reduces compliance.
Once the wound has closed, avoiding tension and stretching of the wound is beneficial. Probably the most simple and cheapest scar prevention is Micropore® paper tape. In a randomized, controlled trial conducted assessing the scars following caesarean section, one group of patients applied paper tape to their scar for 12 weeks, while the control group received no postoperative intervention. Interestingly, paper tape significantly decreased scar volume, and at 12 weeks after surgery, 41% of the control group developed HS compared to none in the treatment group. 72
Topical gel sheeting has been popular in the management of scars since its introduction in the early 1980s, and its beneficial effects have been largely documented in the literature.73,74 It is commonly believed that occlusion and hydration are likely the specific mechanisms of the therapeutic activity of silicone gel sheeting rather than a truly pharmacological anti-scarring property of silicone. 75 Application of silicone sheets is usually recommended for ≥12 hours for two months or more, beginning two weeks after re-epithelialization.
Flavonoids are found in well-known topical scar creams (Mederma®, Contractubex®, Merz Labs). So far, efficacy studies testing the ultimate benefit of these products have provided controversial data.76–80
Topical superoxide dismutase (SOD) has been found in our practice to give good results on both KL and HS. SOD is the most potent antioxidant known to date. It is a strong anti-fibrotic, anti-inflammatory, and anti-pruritic agent.81,82 Its anti-fibrotic properties are mainly due to blocking TGF-β expression, but they are also due to its ability to revert myofibroblasts into normal fibroblasts. 83 On the other hand, SOD reduces inflammatory cell migration by regulating adhesion molecules and cytokine expression (namely TNF-α, IL-1, IL-6, and MCP-1). 84 Surgeons currently prescribe topical SOD (Sodermix®, LSI Labs) around the world with apparently successful results, but there is currently a dearth of published data in this regard.
Why Should We Recommend Preventive Therapy after OB/GYN Procedures?
From the published data, it can be deducted that after abdominal incisions, the prevalence rate of HS is at least 50% and can reach 70%. KL are less frequent, but can be of great concern, especially among black women. Physical discomfort or impairment due to scarring often pale in comparison to the psychological effects that these disfiguring lesions have on a scarred individual. In a clinical trial conducted on scar patients, 85 the majority of respondents were unhappy with their scar's appearance due to their perceived stigma and psychological associations, and thus adopted different coping behaviors to hide or compensate for them. Often this made them unsociable and it interfered with their communication skills, personal relationships, work life, and leisure activities. Concerns about the diagnosis and persistent nature of scars were common, while unempathetic managements by their physicians and frustration toward current treatments compounded distress.
On the other hand, a Brazilian paper 86 should attract our attention. It reported the occurrence of HS as a consequence of plastic surgeries, especially following abdominoplasty, a surgery where the incision is comparable to most gynecological incisions. Surprisingly, the incidence of HS was very low (lesser than 1%) even in a population primarily comprised of individuals with darker skin that were prone to the development of KL and HS. To explain these low numbers, it was emphasized that plastic surgeons are very meticulous in their sutures, and that they usually closely manage the scar post-procedure, especially with prophylaxis measures.
All these data taken together should prompt OB/GYN practitioners to pay due attention to the management of scars in order to avoid the development of KL and HS in their patients.
Footnotes
Author Contributions
Wrote the first draft of the manuscript: CD. Contributed to the writing of the manuscript: CD. Agree with manuscript results and conclusions: CD. Jointly developed the structure and arguments for the paper: CD. Made critical revisions and approved final version: CD. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.