
Abstract
This is a qualitative—quantitative study based on hospital records of female patients of reproductive age, presenting sexual dysfunction, and treated with 250 mg
Introduction
Sexual dysfunction in women is characterized by persistent and recurrent problems in sexual response or desire, which cause affliction and affect their relationship with their partner.1,2 Sexual dysfunctions may occur at any age and affect roughly 40% of women at some point in their lifetime, with 12% of women reporting afflictive sexual problems. 3
There are different types of sexual dysfunctions, characterized as (1) sexual interest/arousal disorder; (2) orgasmic disorder; and (3) genitopelvic pain/penetration disorder. 4 It is important to explain to the patient that transient sexual problems are common; however, if the problem persists over months or causes affliction to the patient or their partner, then the cause of the dysfunction should be investigated.5,6
There are several risk factors that may contribute to the emergence of female sexual dysfunction. These include the patient's well-being; important events in romantic relationships; partner's sexual problems; gynecological factors including childbirth, hysterectomy, vaginal pain, or pelvic pain; urinary tract alterations; and drug side effects (use of beta blockers, anti-depressant, or anti-psychotic drugs).7–11
Several therapeutic alternatives are used in the treatment of female sexual dysfunction; however, it is important to identify any possible contributing physical and emotional factors before beginning treatment.9,11,12 Therapeutic approaches include stress management and management of any relationship problems, treatment of vaginal dryness, dyspareunia, and investigation of possible drug side effects.10,11 The use of testosterone in the form of gels, creams, ointments, or in oral form is not recommended for pre-menopausal women, and carry the risk of side effects in addition to containing very high doses of testosterone.13–16 The use of medications for erectile dysfunction has proven to be largely ineffective.9,15,17 Dehydroepiandrosterone (DHEA) has been shown to be effective in improving sexual interest and satisfaction among women with adrenal insufficiency; however, the benefit of supplementation in women with normal adrenal function has not been confirmed.18–20
In this study, we evaluated the use of
Objectives
The primary study objective was to evaluate the efficacy of
Material and Methods
This was a qualitative-quantitative study performed at Hospital das Clínicas de Teresópolis (Teresópolis—RJ, Brazil). Subjects were included based on inclusion and exclusion criteria, followed by hospital records verification. Inclusion criteria for female patients are that they should be of reproductive age (over 18 years old), with a clinical presentation of sexual dysfunction, who were treated with tablets containing 250 mg
Exclusion criteria were pregnant or breastfeeding women, patients presenting hypersensitivity to any component of the study medication, and any other diseases or conditions that, in the opinion of the investigator, exclude the patient from the study. All study data were recorded in the clinical research form, in which subjects were identified using 3-digit sequential numbers.
In addition to physical examination results (vital signs, weight, body mass index [BMI]), safety analysis included the following laboratory test results: complete blood count, amylase, glucose and fasting glucose, serum prolactin, follicle-stimulating hormone, leutenizing hormone, thyroid-stimulating hormone, serum potassium, blood urea nitrogen, serum creatinine, total and fractionated billirrubins, alkaline phosphatase, aspartate aminotransferase, and alanine aminotransferase. Occurrence and severity of adverse events were also included in the safety analysis. The primary safety and tolerability measures included any changes in vital signs and physical examination in relation to pretreatment, any changes in clinical laboratory examinations in relation to pretreatment, and the occurrence of adverse events after the first dose of study medication. Any laboratory examinations out of reference range were recorded as adverse events. The secondary safety measure was the evaluation of overall tolerability of the study medication performed post-treatment by the study physician, using the same classifications of “Very Good”, “Good”, “Fair”, or “Poor” as were used for the overall efficacy assessment.
The primary efficacy analysis included results of the Female Sexual Function Index (FSFI), a validated self-report measure of female sexual function. This is a 19-item questionnaire that is subdivided into six domains: desire, arousal, lubrication, orgasm, satisfaction, and pain. The scoring system followed the instructions given by the authors who developed and validated the questionnaire. The maximum possible score is 36 points and the minimum possible score is 2 points. 22
Secondary efficacy measures included the Patient and Physician Assessments, in which both the subject and the physician rated the patient's overall condition on a scale of 1–10 points, with “1” corresponding to the worst assessment and “10” the best. The study physician also evaluated the overall efficacy and safety of the study medication as “Very Good”, “Good”, “Fair”, or “Poor”. DHEA levels together with total and free testosterone were also included in the efficacy analysis (reference ranges: DHEA: 15–170 ng/mL; serum testosterone: 3–63 ng/dL; free testosterone: 2–45 pmol/mL).
At the end of the treatment period, subjects who completed the treatment cycle were asked to rate their willingness to continue treatment on a scale of 1 (very unwilling) to 10 (very willing).
The clinical research form was filled, coded, and the data were analyzed using GraphPad Prism version 5.1 software. Frequency tables were generated and central tendency measures were calculated (mean, median, mode). As appropriate, we used the Student's
Results
A total of 144 subjects were included in the initial analysis. Mean patient age was 41.01 years (±7.07). Sixty subjects (41.67%) were married, while 55 (38.19%) were divorced, 22 (15.28%) were single, and 7 (4.86%) were widows. Ethnicity (self-reported) was as follows: Asian (
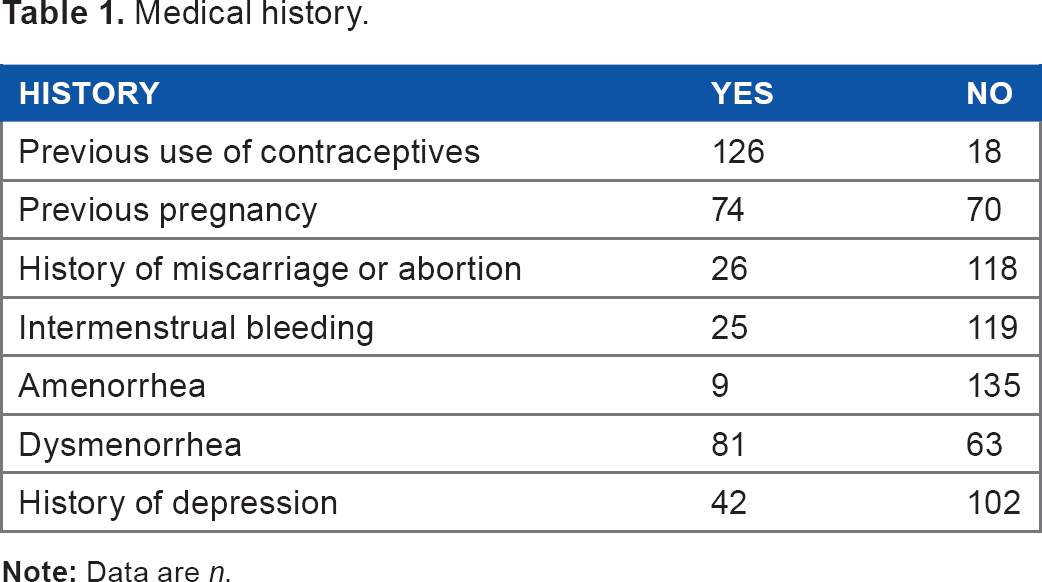
The relevant medical history including use of contraceptives, reproductive, and menstrual information together with data on depression is summarized in Table 1.
Medical history.
Mean DHEA level at pretreatment was 57.83 ng/mL (±30.11), while there was a statistically significant (
FSFI scores improved among 106 (88.33%) subjects at the end of the treatment period, while 14 subjects (11.67%) had decreased total scores compared to pretreatment values (Fig. 1). There was a statistically significant improvement in the total FSFI score (
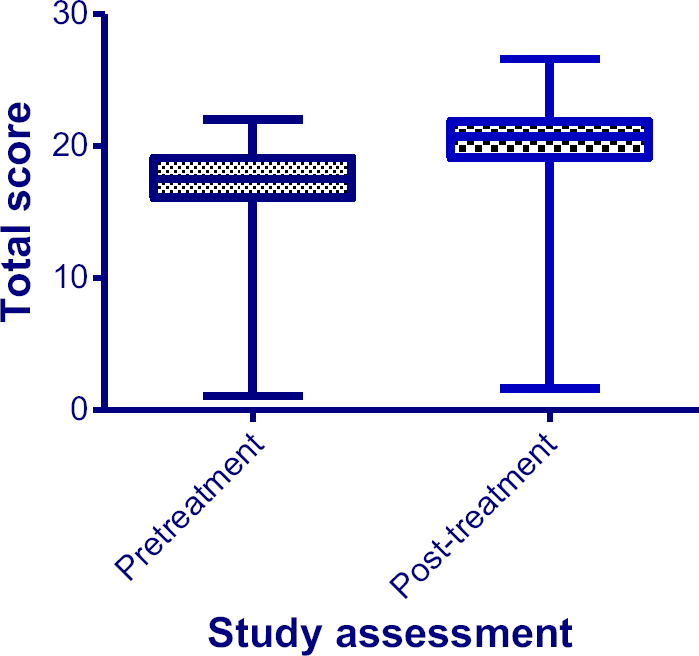
Mean total FSFI scores from pre- and post-treatment. There was a statistically significant improvement in the mean total FSFI score (
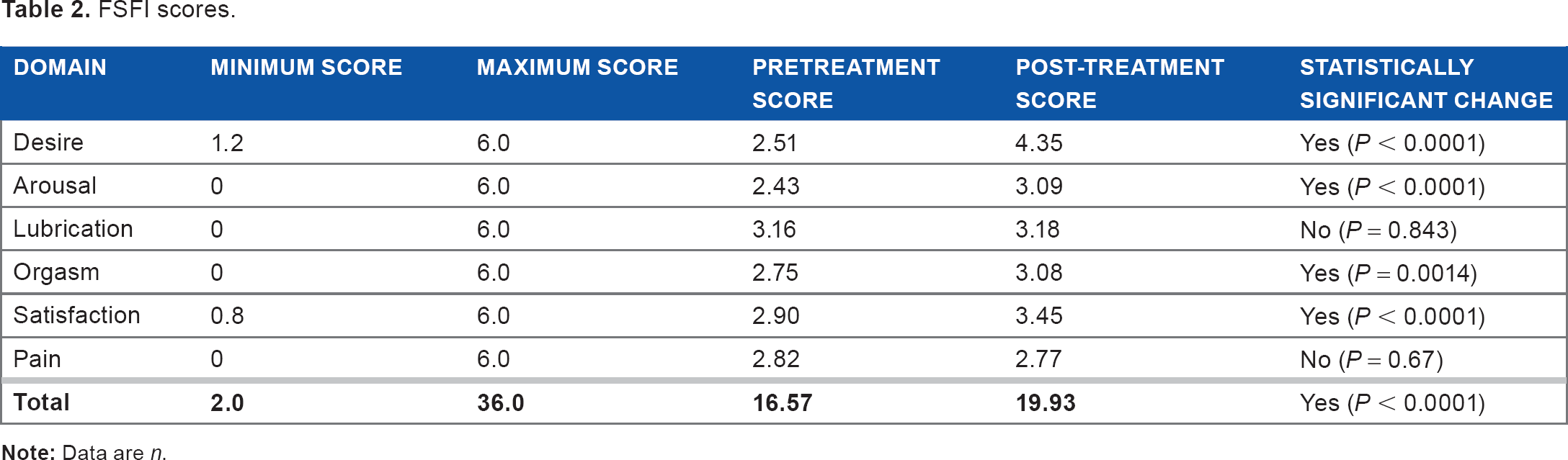
Table 2 summarizes the FSFI scores showing both the total scores and those of the individual domains. Statistically significant (
FSFI scores.
There were statistically significant improvements (
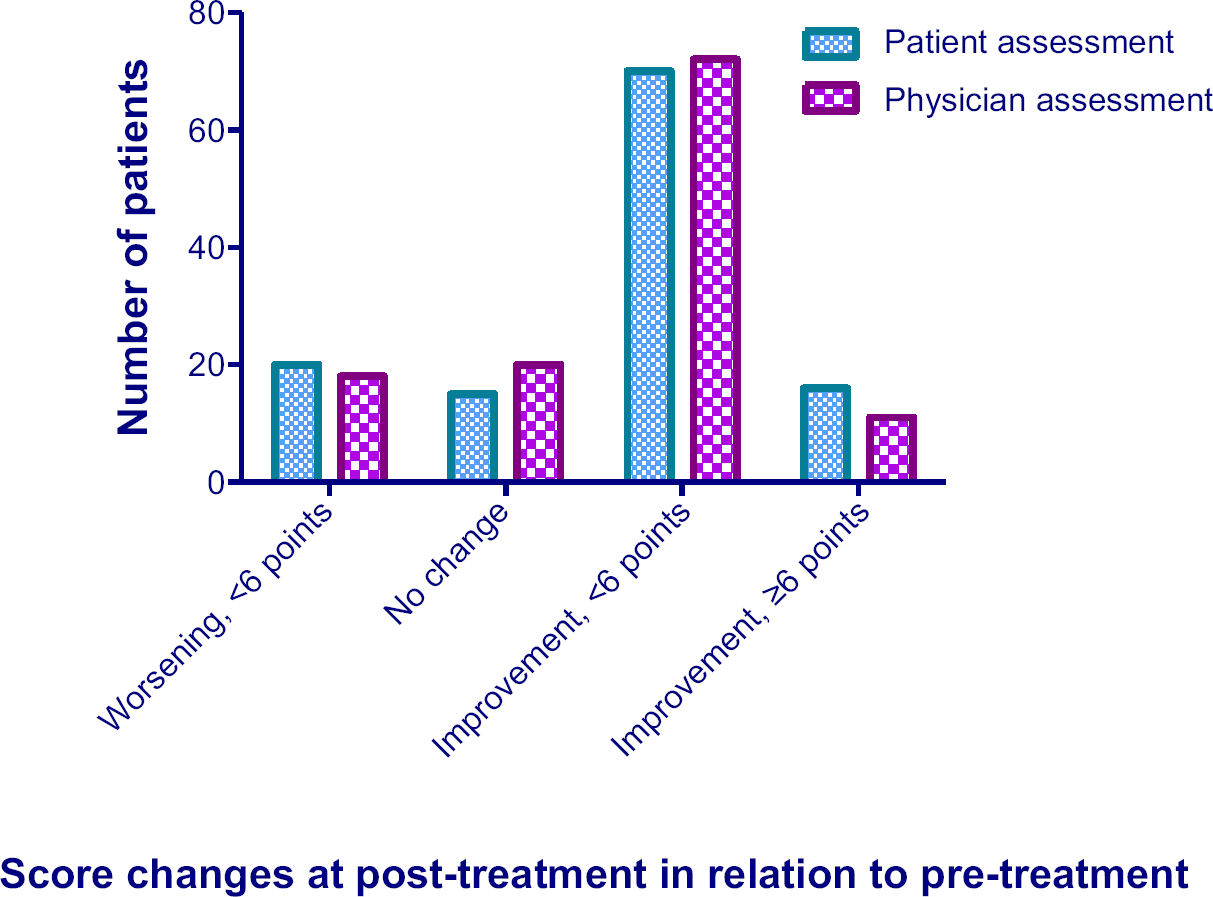
Patient and physician overall assessment scores from pre- and post-treatment. There were statistically significant (
The adverse events reported during the treatment period are summarized in Table 3.
Adverse events.

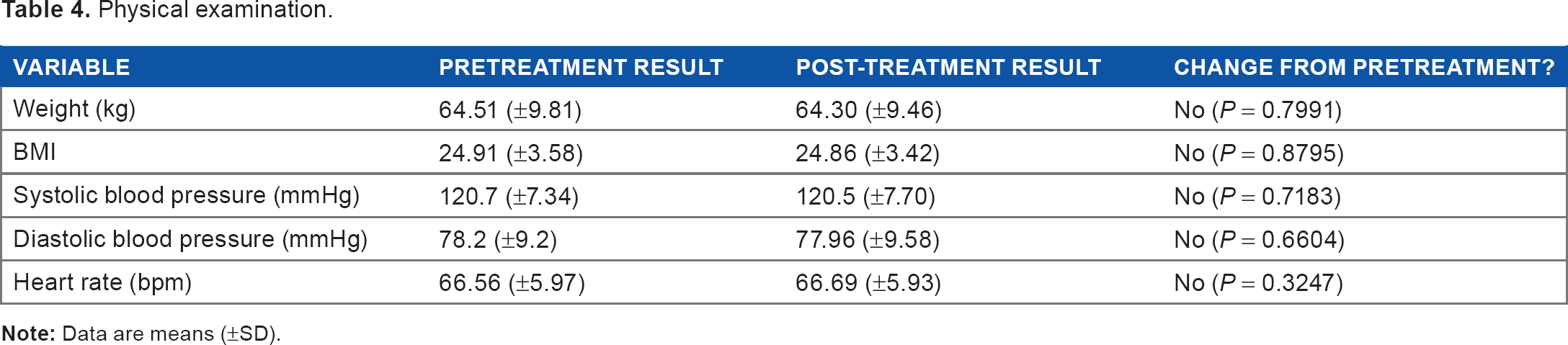
Table 4 summarizes the results of the physical examination performed pre- and post-treatment. No significant changes were recorded post-treatment.
Physical examination.
Discussion
The results show that the treatment was effective in terms of improvement in the FSFI questionnaire, with the majority of patients showing improved post-treatment scores together with statistically significant improvements in the total score of the questionnaire as well as in most of the individual domain scores. Although side effects were reported, there were no reports of serious adverse effects during the treatment period. The safety evaluations including laboratory tests and physical examination results did not undergo significant alterations during the treatment period.
Overall,
The assessment of the female patient presenting with sexual dysfunction should take into account a wide variety of factors, including an important emotional component. Interestingly, during pretreatment assessment, we observed a relatively high number of patients self-reporting depression during the assessment of medical history, a finding that reflects the data present in the literature.25,26
Protodioscin is a chemical substance derived from the
However, the lack of correlation between increasing DHEA levels with both free testosterone and serum testosterone levels is confounding. Contrary to expectations,34,35 mean testosterone levels decreased among the total treated subjects, despite the presence of a clinical response. It may be because the DHEA levels in women have a greater impact on FSFI domains in relation to testosterone, explaining our positive results. A larger, prospective, randomized, comparative study would likely provide further insight into the effect of
Conclusion
The co-occurrence of enhanced female sexual function and increased DHEA levels is suggestive of physiological alterations underlying clinical improvement following treatment. Our results strongly support the safety and effectiveness of
Author Contributions
Conceived and designed the experiments: CRBG, RL, MG, LO. Analyzed the data: LO, AS. Wrote the first draft of the manuscript: MG, LO, CSA. Contributed to the writing of the manuscript: RL, CRBG, CSA, CPN, GFG. Agreed with manuscript results and conclusions: CRBG, RL, GFG, CSA, CPN, MG, LO, AS. Jointly developed the structure and arguments for the paper: CRBG, RL, LO. Made critical revisions and approved final version: CRBG, RL, GFG, CSA, CPN, MG, LO, AS. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
The authors would like to thank Daiane Bergamim, Flavia Dweck, and Renata Ribeiro Coutinho for their help with data verification, Silvia Maciel for CRF verification, and Oscar Roberto Guimarães for help with laboratory test data.