
Abstract
Objective
To analyze and compare occurrence of adverse immediate neonatal outcomes in high and low-risk obstetrical population.
Methods
Retrospective cohort study of 2370 pregnant women.
The odds of adverse outcomes (i.e. low Apgar score (1–4 points) and intermediate Apgar score (5–8 points) at 1 and 5 minutes of life, birth to a small-for-gestational-age neonate (below 90th percentile of birth weight), and requirement for advanced level II-III nursery care) as well as odds of primary cesarean delivery–-were analyzed using logistic regression analysis.
Results
All of the studied outcomes were seen more often among the high-risk patients.
When the outcomes were analyzed within a given group some interesting observations were made.
The highest odds of abnormal Apgar scores (when compared to the low risk population) were seen in patients with preeclampsia–-6.06 (95% CI 3.28; 11.22) and twin pregnancies–-odds ratio of 6.63 (95% CI 2.24; 19.67).
Among Small-for-Gestational-Age newborns the most frequently identified maternal condition was preeclampsia (21.57%), out of all fetal conditions twin gestation (26.67%) was number one identified scenario.
The highest proportion of patients requiring advanced level nursery care (level II and III) was observed in those with twin gestation, pregnancies complicated by hypertension with and without diabetes.
The highest odds of having primary cesarean delivery in laboring patients (when compared to the low risk population) were seen in the patients with IUGR fetus–-odds ratio of 26.78 [95% CI 7.65; 93.75], followed by macrosomia–-odds ratio 5.74 [95% CI 2.14; 15.41], preeclampsia–-odds ratio 5.52 [95% CI 3.14; 9.69].
For additional findings and more information on select conditions, please, refer to the full-text article.
Conclusion
The studied outcomes are useful markers of fetal/neonatal status and can be used to compare perinatal outcomes between different medical conditions, different locales and to assess the dynamics of fetal/neonatal well-being over the course of time.
Level of Evidence
II Detailed information on the studied adverse neonatal outcomes can be found in the full-text version of this document.
Introduction
High-risk pregnancies represent a management challenge in obstetrics with multiple fetal and neonatal outcomes being affected.
Fetal and neonatal mortality is the extreme of the entire spectrum of the adverse outcomes. Even though the incidence of the mortality is on decline: fetal death rate 11.5 per 1000 in 1960s vs. 3.2 per 1000 in 1990s (1), interpretation of this relatively rare event is only possible with large population-based study. It is a subject to all of the flaws of meta-analysis–-an attempt to “amalgamate” very heterogeneous data collected from different centers (2,3).
There are much more prevalent markers of fetal and neonatal status that can be analyzed within a single institution, compared between different centers and studied over time.
This study offers a comprehensive comparison of many important neonatal outcomes between pregnancies complicated by a high-risk condition and those considered “normal”.
It also examines the outcomes of the select high-risk conditions and presents them in a structured manner.
Areas of the outmost concern and clinical significance are identified. In this respect this work may be considered as a pilot study directed at the areas of interest for the future in-depth investigation.
The results of the study are presented and discussed in a non-judgmental manner. The most important final points are fortified by presenting them at a glance in colorful fashion.
Materials and Methods
The retrospective cohort study was performed in a setting of a community hospital serving diverse multiethnic patient population in Queens Borough of the city of New York. It included both patients managed in a private sector and those managed exclusively by obstetrical service of the Saint Vincent Catholic Medical network. Perinatology services were made easily accessible for all patients.
The data were derived from the hospital delivery registry.
In the course of this population-based study the total cohort of pregnant women was divided into 2 groups: the “high risk” group and the “low risk” group retrospectively.
The “high risk” group included patients with preexisting or pregnancy-related medical conditions that are known to confer high risk for fetal compromise. These patients are typically managed with close antepartum monitoring for signs of fetal distress by means of non-stress testing, amniotic fluid index measurement and estimation of fetal weight. When it is appropriate, umbilical artery Doppler flow study and amniocentesis to document fetal lung maturity may also be performed. If there is an indication of fetal jeopardy the management eventuates into a timely delivery.
All other patients were assigned to the “low risk” group. Their surveillance included routine prenatal evaluation and prenatal clinic visits with fetal heart and fundal height measurement (see Fig.1).
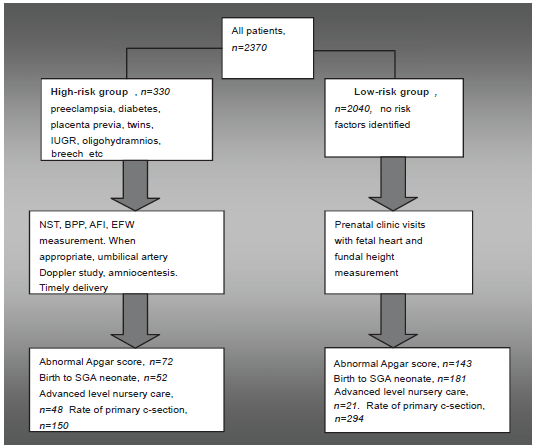
Study design.
The odds of adverse outcomes (i.e. low Apgar score (1–4 points) and intermediate Apgar score (5–8 points), birth to a small-for-gestational age neonate, and requirement for level II–III nursery care) as well as odds of primary cesarean delivery–-were analyzed using logistic regression analysis. In order to improve the sensitivity for detecting slightest variations in the neonatal status intermediate Apgar scores at either 1 or 5 minutes were also included.
Among the abbreviations, that will be used here: CHTN- stands for chronic hypertension, HTN- stands for hypertension, PIH–-stands for preeclampsia, GA-for gestational age, SGA-for small for gestational age neonates (10th percentile of weight at birth was used), LGA–-for large for gestational age neonates (90th percentile of weight at birth was used), IUGR-intrauterine fetal growth restriction (low estimated fetal weight before birth), NST-non-stress testing, BPP-biophysical profile, AFI-amniotic fluid index, EFW-estimated fetal weight, CI–-for confidence interval (95% range was used for all calculations).
Patients with gestational diabetes were divided into classes according to the Dr. White's Classification. The “mode of gestational age” term was used to define the most prevalent gestational age at the time of delivery.
High-risk pregnancies include many different conditions and each condition contributes to the composite outcome. In order to make the results suitable for comparison, prevalence of each high-risk condition was also reported, as well as the outcomes for the given condition (see Table 1).
Preexisting high-risk conditions are presented in the order of frequency in the following.
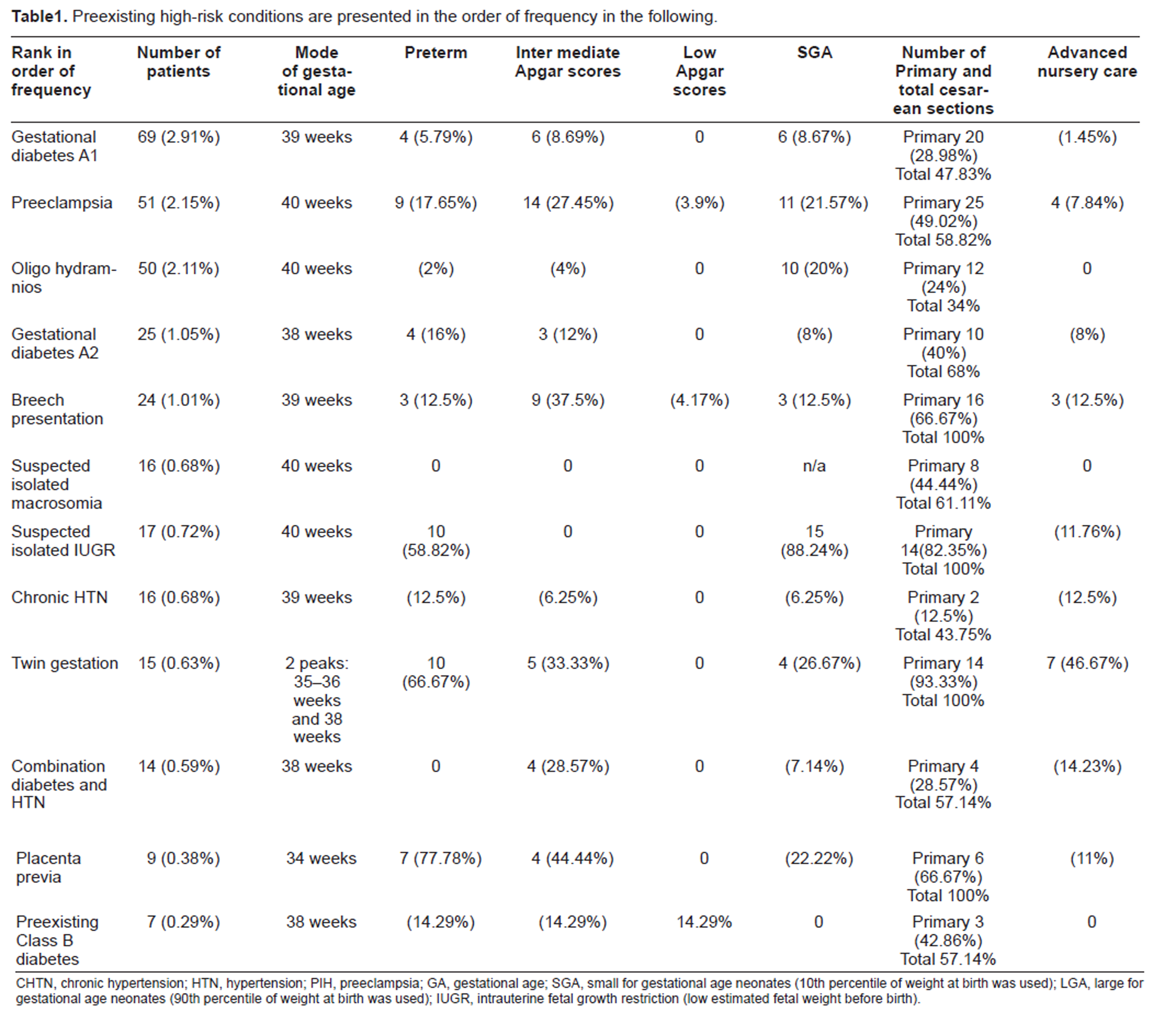
CHTN, chronic hypertension; HTN, hypertension; PIH, preeclampsia; GA, gestational age; SGA, small for gestational age neonates (10th percentile of weight at birth was used); LGA, large for gestational age neonates (90th percentile of weight at birth was used); IUGR, intrauterine fetal growth restriction (low estimated fetal weight before birth).
Results
Over the course of 15 months the total number of deliveries that took place in our hospital was 2370.
High-Risk Group
High-risk group included 330 patients (13.92% of the total population).
The results obtained in this group are summarized in the following Figure 2.
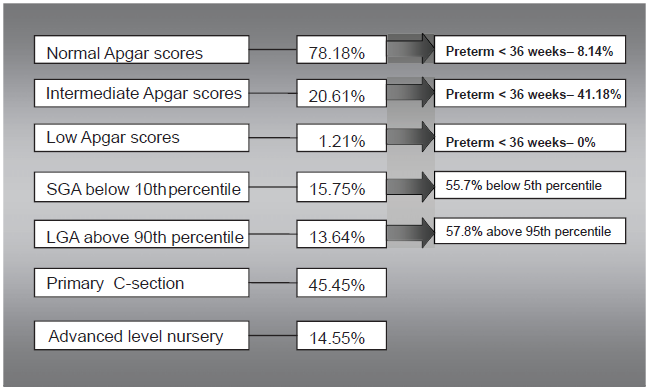
Summary of data on high-risk population.
Majority of the abnormal Apgar scores seen in this group were intermediate scores at 1 minute that recovered to normal level by 5 minutes. In patients with low Apgar scores immediately at birth the unsatisfactory scores were seen mostly in severe preexisting conditions (1.21%): 2 patients with severe preeclampsia, 1 patient with pre-gestational diabetes Class B. The most prevalent gestational age in these patients was 36–38 weeks (all of these patients delivered near term).
Only 7 neonates had persistent intermediate Apgar score at 5 minutes (2 patients with preeclampsia, 2 with twin gestation, 2 with insulin controlled diabetes (GDMA2 and GDMB), and 1 with breech presentation who came to the hospital in advanced labor). Fortunately, there were no neonates with low Apgar score at 5 minutes seen in this group.
Preterm labor occurred in 15.45% of the high-risk patients. The highest probability of preterm labor was seen in patients with placenta previa (odds ratio 19.15, CI [3.87; 94.79]), multiple gestation (odds ratio 10.94, CI [3.59; 33.34]), suspected IUGR (odds ratio 7.82, CI [2.84; 21.48]), severe preeclampsia. These premature newborns contributed significantly to the composite rate of intermediate Apgar scores and 84.31% of them required advanced level nursery care.
15.45% of high-risk patients delivered after their respective due date. In these patients with late development of high-risk conditions, such as mild preeclampsia, suspected macrosomia and oligohydramnios–-proportion of primary cesarean delivery was 50.98%.
15.75% of “high-risk newborns” were found to be small-for-gestational-age neonates. Neonates with severely reduced birth weight below the 5th percentile numbered more than half and were more likely to have intermediate Apgar scores (27% probability vs. 23%).
13.64% of “high-risk newborns” were born large-for-gestational-age. Very large babies with weight above 95th percentile were seen in more than one half of cases. 64.44% of all LGA neonates were born to a diabetic mother. 86.67% of the LGA neonates were delivered by C-section.
14.55% of the neonates born in the high-risk group were found to be in need for the advanced level nursery care. The highest demand was observed in cases of twin gestation, pregnancies complicated by hypertension with and without diabetes.
62.42% of the high-risk women delivered by cesarean section and 72% of these c-sections were primary. After excluding contraindications to vaginal delivery, the remaining high-risk patients were allowed to labor. These laboring patients contributed to 70% of primary cesarean deliveries. The most common indications for C-section were fetal intolerance of labor, dystocia and failed induction of labor.
37.58% of the high-risk patients delivered vaginally.
Low–-Risk Group
Low–risk group included 2040 women.
The results obtained in the low-risk group are summarized in the Figure 3.
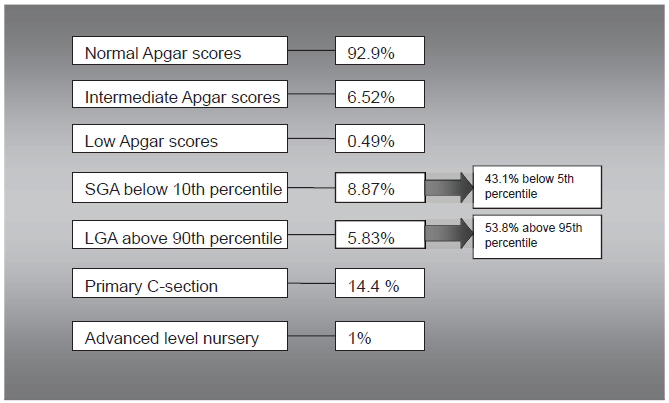
Summary of data on low-risk patients.
In this group majority of abnormal Apgar scores seen were again intermediate scores at 1 minute that recovered to normal level by 5 minutes. 10 neonates continued to have 5–8 points Apgar score at 5 minutes (4 with isolated meconium staining of the amniotic fluid, 3 with nuchal cord, 1 with suspected chorioamnionitis, 1 with dystocia, 1 without any historic risk factors).
In neonates with low Apgar scores at 1 minute 90% recovered to intermediate level at 5 minutes.
8.87%of mothers delivered Small-for-Gestational-Age neonate, 43.1% out of the newborns had severely reduced birth weight below the 5th percentile.
5.83%of patients gave birth to a Large-for-Gestational-Age neonate. Birth weight above 95th percentile was seen in 53.8% of neonates.
The overall rate of the primary cesarean delivery in the low-risk group was 14.4%. In the low risk group with abnormal Apgar scores the rate of primary cesarean deliveries was similar –14.7%.
Advanced nursery care was required in 21 neonates (1% of total low-risk population): with the most prevalent gestational age of 39 weeks majority of these babies (61.9%) were born with abnormal Apgar scores via cesarean delivery (61.9%).
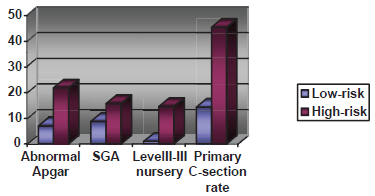
When the analyzed outcomes were compared between high-risk and low-risk patients all of the outcomes were more prevalent among the high–-risk patients (see Fig. 4): for example, chances of intermediate Apgar scores at 5 minutes of life were increased by odds of 4.39 (95% CI 1.66; 11.64, p 0.0028) in high-risk patients.
The high-risk patients were further divided into the subgroups based on their condition.
Figure 4 Comparison of the adverse outcomes between high and low risk groups (percentage).
The highest odds of abnormal Apgar scores when compared to low risk population were seen in patients with preeclampsia–-6.06 (CI 3.28; 11.22) and twin pregnancies–-6.63 (CI 2.24; 19.67) (Fig. 6). Then in order of the strength of correlation went odds of abnormal Apgar scores in breech presentation–-5.46 (CI 2.23; 13.39), combination of diabetes and hypertension–-5.30 (CI 1.64; 17.13), preexisting diabetes–-5.30 (CI 1.02; 27.59).
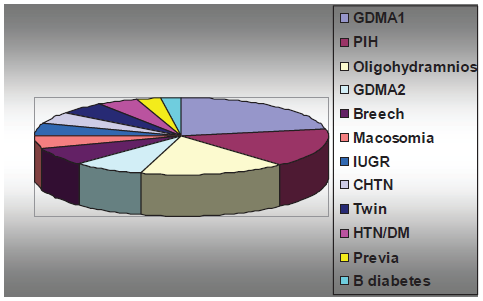
The following diagram illustrates the prevalence of the select high-risk conditions in our patient population.
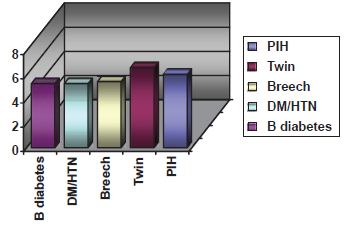
Odds of abnormal Apgar scores in high-risk pregnancies.
When an odds ratio for giving birth to a Small-for-Gestational-Age newborn was calculated, the highest odds comparing to the low risk population were seen in twin gestation–-odds ratio 4.13 with 95% confidence interval [1.30; 13.12], followed by preeclampsia–-odds ratio 3.13 [CI 1.57; 6.21] and oligohydramnios–-odds ratio 2.84 [CI 1.39; 5.78] (Fig.7).
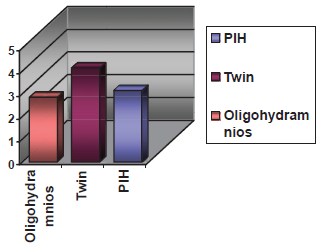
Odds of the birth of SGA neonate in high-risk pregnancies.
The highest proportion of neonates requiring advanced level nursery care was observed in twin gestations and pregnancies complicated by the hypertension with or without diabetes.
Depending on the prevalence of the given condition, statistically reliable determination of the odds ratio for the advanced nursery care was possible in preeclampsia–-8.18 [CI 2.70; 24.77].
With the respect of having primary cesarean delivery during labor the highest odds of primary c-section, when compared to the low risk population, were noted in the patients with IUGR fetus–-odds ratio of 26.78 [CI 7.65; 93.75], followed by macrosomia–-odds ratio 5.74 [CI 2.14; 15.41], preeclampsia–-odds ratio 5.52 [CI 3.14; 9.69], class A2 gestational diabetes–-odds ratio 3.83 [CI 1.70; 8.59], class A1 gestational diabetes–-odds ratio 2.34 [CI 1.37; 3.99].
The odds were not statistically significant for patients with oligohydramnios, chronic hypertension and combination of diabetes and hypertension (Fig.8).
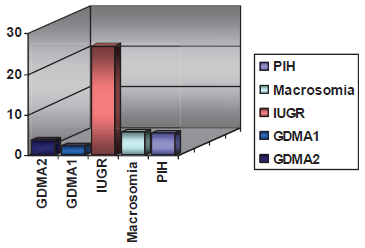
Odds of primary cesarean delivery in high-risk pregnancies.
In order to control for background patient characteristics published studies that reported similar prevalence of a given condition were selected for comparison.
In this study incidence of diabetes in pregnancy was similar to the cited 2%–5% (4).
These patients were followed intensively in our high-risk clinic. The rate of abnormal Apgar scores and advanced nursery care requirement in class A1 gestational diabetes were very close to those observed in low risk population (8.67% and 1.45% respectively). Those indicators rose to their respective 12% and 8% when the gestational diabetes required insulin control.
Odds of macrosomia were significantly increased by 4.64 (CI 1.6454; 13.06) in patients with insulin- versus diet-controlled gestational diabetes. Contrary to the concerns expressed in the earlier articles about SGA in insulin-treated patients due to treatment-induced hypoglycemia and ketosis (5), in this study there was no statistically significant correlation found between insulin treatment and increased incidence of SGA newborns (6,7,8).
Increase in cesarean section rate with insulin treatment of diabetes was observed (possibly because of the increase in the physician awareness of the diagnosis).
Incidence of preeclampsia was found to be within the range reported for developed countries (similar to UK: 2.77%) with no maternal mortality reported (9,10,11,12).
The patients with preeclampsia displayed the highest odds of abnormal Apgar scores out of the entire high-risk cohort–-6.06 (CI 3.2772; 11.2217) when compared to low risk population. 17.65% of these patients delivered preterm and preeclampsia were the most prevalent maternal condition noted in the history of low birth weight neonates.
The primary cesarean delivery rate in preeclamptic patients reached 49.02%. With absolute indications for cesarean delivery excluded–-preeclampsia surpassed all other high-risk maternal conditions.
The odds of advanced level nursery transfer were also as high as 8.18 (CI 2.7028; 24.7704).
Patients with oligohydramnios at term composed 2.06% of the patient population fitting within the reported 1%–5% incidence range (13). Their neonates fared well as correlates with the previous studies (14,15) with only 4% of neonates born with abnormal Apgar scores and none of them required level II nursery transfer.
Fetuses in breech presentation were in 100% of cases delivered by cesarean section (16) with incidence of neonatal morbidity such as low Apgar score (4 and below) of 4.17%. It occurred in 1 term patient who came in advanced labor. Considering 3.1% to 4.7% neonatal morbidity reported earlier (17) this finding was within the acceptable range. It also correlates with reports of adverse neonatal outcome in laboring patients with breech fetus (18).
Small-for- gestational- age (SGA) neonates comprised 15.75% of high-risk population–-higher than the number of SGA normally distributed below the 10th percentile in the general patient population. The birth weight was adjusted for gestational age at birth.
When a maternal condition was identified among SGA neonates, it was most frequently maternal preeclampsia (21.57%). Out of fetal conditions twin gestation (26.67%) was number one identified scenario. Similarly, when an odds ratio for giving birth to SGA newborn was calculated, the highest odds comparing to the low risk population were seen twin gestation–-odds ratio 4.13 with 95% confidence interval [1.30; 13.12], followed by preeclampsia–-odds ratio 3.13 [CI 1.57; 6.21] and oligohydramnios–-odds ratio 2.84 [CI 1.39; 5.78].
The observed incidence of abnormal Apgar scores among SGA neonates was only about 23%–-much lower than the reported 50% (19). As expected majority of the neonates with abnormal Apgar scores belonged to the group with significantly decreased birth weight–-below the 5th percentile for gestational age.
Isolated IUGR contributed to 0.72% of all high-risk pregnancies. Clinical suspicion of this diagnosis was confirmed using ultrasound study and the need for expedited delivery was based on umbilical artery Doppler flow measurement with PPV (positive predictive value) of 88.24%. Even though 58.82% of the patients with isolated IUGR delivered preterm, the incidence of abnormal Apgar scores in this cohort was negligible and only 11.76% of them were judged to be in need of advanced level nursery care. The odds of primary cesarean delivery in the patients with IUGR fetus reached ratio of 26.78 [CI 7.65; 93.75].
The number of LGA neonates in high-risk group totaled 13.64%, out of them LGA above 95th percentile was noted in 57.78%. In both instances the incidence rate was higher than the rate expected with normal distribution of birth weight (20,21). Majority (64.44%) of all LGA neonates were born to a diabetic mother.
The intermediate Apgar scores were noted in 17.77% of LGA newborns. Counter-intuitively, majority of the scores were seen in patients with the birth weight falling between 90th and 95th percentile, perhaps, because this subgroup of patients contained slightly more patients with preeclampsia and class B pre-gestational diabetes; these patients also were more likely to undergo a trial of vaginal delivery. Primary cesarean section rate in LGA neonates was 71.11%, total c-section rate–-86.67% (22).
By comparison, patients with isolated suspected macrosomia delivered at slightly more advanced gestational age with lower primary c-section rate of 44.44%. In these patients there were no abnormal Apgar scores noted and none of the neonates received advanced nursery care.
Chronic hypertension was found in 0.68% of patients in this study. It is in the lower range of the prevalence of 0.6%–2% (up to 4.6%–22.3% for women near age of 40) reported by National Health Survey (23). This lower prevalence may in part be explained by the observation, that certain ethnic groups with known high prevalence of hypertension (e.g. patients of African American descent) constitute only a minority of patients in our locale (24). It is also a fact that substantial proportion of patients presents for prenatal care in the second trimester of pregnancy when preexisting chronic hypertension is masked by the normal nadir of blood pressure in pregnancy.
In the setting of chronic hypertension 12.5% of patients experienced a complicated course of pregnancy and delivered preterm. The abnormal Apgar scores and birth of SGA neonates occurred with 6.5% rate for each indicator; the primary cesarean delivery rate seen was 12.5%–-all at the level of the low risk population.
Combination of diabetes with hypertension (0.59%) was accompanied by higher incidence of abnormal Apgar scores (28.57%), primary cesarean deliveries (28.57%) and higher requirement for advanced level nursery care (14.23%).
Twin gestations comprised 0.63% of patient population with 2 peaks of gestational age at delivery observed: 35–36 weeks and 37–38 weeks. Composite rate of preterm delivery was 66.67% (25), abnormal Apgar –33.33%, SGA –26.67%, advanced nursery care –46.67%. All patients delivered by cesarean section.
When twins were analyzed according to their gestational age: overall, twins born at 35–36 weeks constituted the largest subgroup. They also fared the best with the lowest rates of abnormal Apgar scores–-21.43%, SGA –7.14%, advanced level nursery care –7.14%–-when compared to both very premature and term fetuses.
This is in agreement with an observation in literature that electively delivered newborns, even at term, have a higher incidence of respiratory complications (26).
Placenta previa in our population occurred with incidence of 0.38% with preterm deliveries as numerous as 77.78% (correlating very well with published studies (27,28)). By contrast, majority of the patients delivered at or after 34 weeks with resultant relatively moderate need for advanced nursery care (11%). There was no statistically significant increase in the rate of births to SGA infants.
Low risk group with abnormal apgars was further divided into subgroups with and without identifiable risk factors:
During the course of delivery intrapartum factors were noted in 19.58% of abnormal scores, as following, in order of frequency:
Presence of meconium noted during labor;
Repeat cesarean delivery;
Suspected chorioamnionitis;
Dystocia;
Placental abruption.
Majority of these patients (96.42%) delivered with intermediate Apgars scores and mode of gestational age of 40 weeks. Low score was noted in 1 patient with suspected chorioamnionitis.
Retrospectively identified factors:
Nuchal cord detected at delivery accounted for 39.86% of abnormal scores. Again majority of these babies were delivered with intermediate Apgars and only 7% of them delivered with low Apgars.
No intrapartum factors were identified in 32.87% of cases of abnormal Apgar score. In this subcategory: 89.36% of scores were intermediate at 40 weeks of gestational age. Low 1-minute Apgar scores were seen in 5 patients (10.64% of the unexplained abnormal scores) with mode of gestational age at 38 weeks.
When analyzed within the low risk population the odds of having abnormal Apgar scores in patients with nuchal cord were found to be 2.79 (95% confidence interval [1.97; 3.97]). The odds ratio was not statistically significant in the low risk patients with isolated presence of meconium in labor or elective repeat cesarean delivery.
Discussion
All of the studied outcomes were increased in high-risk patient population. This indicates that the studied outcomes are useful markers of fetal/neonatal status and can be used to compare perinatal outcomes between different medical conditions, different centers and to assess the dynamics of fetal/neonatal well-being over the course of time.
Universally used Apgar scores reflect the status of a neonate at birth; this indicator becomes especially significant with scores below 4 points for longer than 5 minutes, when accompanied by severe acidemia or neurological manifestations (29,30). Fortunately, in our center there were no low 5-minute scores seen among the high-risk patients during the course of study.
Small–-for–-gestational-age (SGA) birth weight is normally distributed in the general population and is usually constitutional. In the high-risk patients increase in incidence of SGA above the baseline level is probably attributable to the greater rate of placental insufficiency. In some instances and in high-risk conditions, such as preeclampsia–-SGA birth weight was shown to be an independent predictor of adverse neonatal outcome (31,32). There are limited resources in modern obstetrics to abate this condition once it developed.
Overall, extremes of birth weight were seen more frequently in high-risk population in the course of the study.
Increased requirements of advanced level nursery care (level II for premature neonates and level III or NICU–-for severe cardio-respiratory decompensation, congenital anomalies, etc.) were also noted among the high-risk group and are self-explanatory (33). In part, it is a reflection of the precautionary attitude of medical providers in an attempt to provide close medical surveillance for newborns born as a result of high-risk pregnancy.
In many parts of the world, in countries such as Australia, Latin America and United States there were raising concerns over the increasing rate of cesarean delivery (34,35). In this study cesarean section rates were analyzed among different patient groups and the predominant indications were identified.
When absolute indications for cesarean delivery are excluded and a patient is allowed to labor, a primary c-section in labor is usually performed because of dystocia, fetal intolerance of labor or failed induction of labor. Dystocia is likely to become a predominant indication for primary cesarean section in a setting of complicating diabetes, suspected macrosomia or postduedate pregnancy. While in preterm or lower weight fetuses, fetal intolerance of labor is more likely explanation for the increased cesarean section rate, such as extremely increased odds of primary C-section noted in IUGR fetuses.
Detailed information on multiple adverse neonatal outcomes in select high-risk conditions can be found in the “Results” section of this document. These data complement limited facts on the neonatal outcomes of interest available from published studies.
Conclusions
The studied outcomes are useful markers of fetal/neonatal status and can be used to compare perinatal outcomes between different medical conditions, different locales and to assess the dynamics of fetal/neonatal well-being over the course of time.
The intermediate Apgar scores among the high-risk patients seem to be closely related to prematurity, while low Apgar scores–-to the severity of the underlying condition. With the appropriate state-of-the-art management of high-risk pregnancies the abnormal Apgar scores in this group of patients can be anticipated and appropriately addressed with advanced level nursery care. Fortunately, during the course of study there were no low Apgar scores seen among the “high-risk neonates” at 5-minutes of life. This observation places the prevalence of persistent low Apgar scores in high-risk population below 0.3%.
While with contemporary obstetric management a decent neonatal outcome became a reality in many high-risk conditions, in many respects, preeclampsia remains a major culprit in terms of the analyzed adverse neonatal outcomes. Much less prevalent twin gestation is in close proximity. These two conditions displayed the highest odds of abnormal Apgar score (odds ratio of 6.06 in preeclampsia and 6.63 in twin gestation), the highest chances of giving birth to a Small-for-Gestational-Age neonate (odds ratio of 3.13 in preeclampsia and 4.13–-in twin gestation) and the greatest rate of transfer to advanced level nursery.
The highest odds of having primary cesarean delivery in laboring patients, when compared to the low risk population, were seen in the patients with IUGR fetus (odds ratio of 26.78), followed by macrosomia (odds ratio–-5.74) and preeclampsia (odds ratio–-5.52).
Further studies in the area of the improvement of neonatal outcome in pregnancies with complicating preeclampsia and in twin pregnancies might prove beneficial.
In low risk pregnancies a possibility of abnormal Apgar scores (intermediate scores at birth in up to 6.52% and low scores in 0.49%) still exists and in almost one third of those cases no known contributing factors can be identified.
With follow-up studies being invaluable, this information can be used to increase awareness of the patients and medical staff of the remote, but nevertheless a possibility of an adverse outcome in case of otherwise uneventful pregnancy and delivery.
Disclosure
The author reports no conflicts of interest.