
Abstract
A 32-year-old man underwent excision of an aneurysm of the left atrial appendage which had been causing palpitation and supraventricular tachyarrhythmia. Various techniques are useful for making the diagnosis and allowing differential diagnosis between this and other pathologies. In this report, the diagnosis was based on transthoracic and transesophageal echocardiography, and the patient was treated by surgical resection of the aneurysm on cardiopulmonary bypass. There were no postoperative complications. Four months later, the patient remained asymptomatic and in sinus rhythm.
Introduction
Congenital aneurysm of the left atrial appendage is extremely rare. The first case of this complication was reported by Semans and Taussig in 1938, and only 50–55 cases have been reported since in the literature. 1 Most of the cases are recognized by atrial fibrillation, flutter, or other supraventricular arrhythmia that results in palpitation, faint, cardiac insufficiency, and systemic embolism.2,3
The majority of cases are congenital and become evident during the second or third decades of life. 4 Resection of the aneurysm has proved to be an effective treatment which stops both supraventricular arrhythmia and systemic embolism. 5
Case Report
A 32-year-old man presented in New York Heart Association functional class I with dyspnea on exertion and faintness of two months’ duration. There was no history of heart failure, embolism, or rheumatic heart disease, but he had been treated previously for palpitation using propranolol. His heart sounds were normal. No murmurs were detected, but he had atrial fibrillation. Chest radiography revealed cardiomegaly. The transthoracic echocardiogram was interpreted as revealing a pericardial cyst or atrial aneurysm (Fig. 1). A subsequent transesophageal study confirmed an aneurysm of the left atrial appendage.
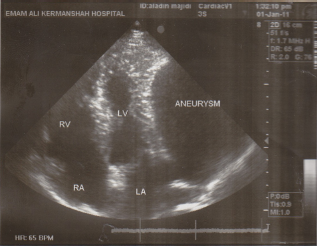
Transthoracic echocardiography: Apical four-chamber view showing an aneurysmal left atrial appendage.
At the time of surgery, via a median sternotomy on cardiopulmonary bypass, without aortic cross clamping, opening of the pericardium revealed a large 15 × 15 cm intrapericardial left atrial aneurysm filled with blood and compressing a deformed left ventricle (Fig. 2). There was also a large superior left vena cava.
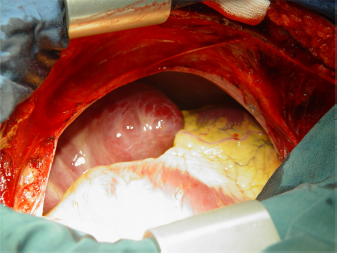
Surgical view through median sternotomy showing intrapericardial aneurysmal left appendage lying along the left cardiac border. Note the abnormal course of the left anterior descending artery.
After elevation of the apex of the heart, the neck of the aneurysm was visible and accessible. A nontraumatic vascular clamp was applied to the aneurysmal neck and the aneurysm was resected (Fig. 3), restoring sinus rhythm. The left atrium stump was closed using two rows of running sutures. There were no postoperative complications. Four months later, the patient remained asymptomatic and in sinus rhythm.
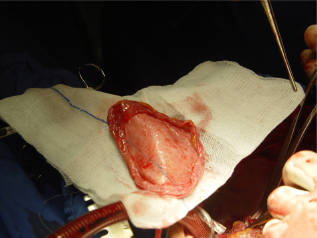
Surgically resected left atrial appendage from this patient.
Discussion
Aneurysm of the left atrial appendage is a very rare pathology, with few cases reported in the literature. 6 The majority of the cases are congenital, although there have also been reports of aneurysm associated with mitral valve pathology. 7 The origin of congenital aneurysm has been attributed to dysplasia of the pectinate muscles of left atrium. 8
Although there is some discrepancy in the literature with regard to what constitutes a congenital aneurysm and which aneurysmal dilatations of the atrium are secondary to congenital mitral regurgitation,9,10 this difference carries only academic value, because the clinical approach is the same, ie, resection of the aneurysm and repair or replacement of the valve as needed.11,12
There are established criteria for the differential diagnosis between a left atrial aneurysm and other pathologies, such as mitral valve disease or juxtaposition of appendages. 13 These criteria are the presence of a left atrium with normal characteristics and direct continuity of blood flow between the left atrium and the appendage. 14
Conclusion
In conclusion, a young or middle-aged patient with supraventricular arrhythmia and an abnormal chest x-ray may have a congenital aneurysm of the left atrial appendage. Diagnosis of a congenital left atrial appendage aneurysm indicates prompt aneurysmectomy, which eliminates all the symptoms and prevents potential complications. Although resection alone is usually adequate, surgery is sometimes combined with the Cox Maze procedure for ablation of auricular fibrillation, especially if there is dilatation of the left atrium or if electrocardiographic mapping indicates induction of fibrillation by auricular foci. 15 In the present case we performed resection alone because there was no dilatation of the left atrium.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Footnotes
Acknowledgments
This study was funded by the Imam Ali Heart Centre, Kermanshah University of Medical Sciences. We very much appreciate the commitment of personnel in the Division of Cardiac Surgery at the Imam Ali Heart Centre.