
Abstract
Objective
This meta-analysis explored the safety and effectiveness of different anticoagulant regimens after left atrial appendage occlusion (LAAO).
Methods
Databases, such as PubMed, MEDLINE, EMBASE, Web of Science, and Cochrane Library, were searched to identify eligible studies according to the inclusion criteria. The incidences of events, including device-related thrombus (DRT) formation, stroke, systemic thromboembolism, bleeding, cardiovascular mortality, and all-cause mortality, were analyzed using R version 3.2.3.
Results
The screening retrieved 32 studies, including 36 study groups and 4,474 patients. The incidence of outcomes after LAAO was calculated via meta-analysis. In the subgroup analysis, the rates of DRT formation, cardiovascular mortality, and all-cause mortality were significantly different among different antithrombotic methods. Single antiplatelet therapy was associated with the highest rate of adverse events, followed by dual antiplatelet therapy (DAPT). Vitamin K antagonists (VKAs) and new oral anticoagulants (NOACs) carried lower rates of adverse events.
Conclusions
Anticoagulant therapy had better safety and efficacy than antiplatelet therapy. Thus, for patients with nonabsolute anticoagulant contraindications, anticoagulant therapy rather than DAPT should be actively selected. NOACs displayed potential for further development, and these treatments might represent alternatives to VKAs in the future.
Keywords
Introduction
Atrial fibrillation (AF) is the most common arrhythmia encountered in clinic practice. The most severe complication of AF is thromboembolism, especially ischemic stroke. Approximately 20% to 30% of strokes are directly caused by AF. 1 Oral anticoagulants (OACs) significantly reduce the incidence of stroke in patients with AF, but long-term anticoagulant therapy might be impeded by bleeding complications in patients with a high risk of bleeding, restricting the use of OACs.2,3
Because 90% of blood clots in patients with nonvalvular AF originate from the left atrial appendage,4,5 left atrial appendage occlusion (LAAO) was developed with the fundamental goal of completely sealing the left atrial appendage, thereby eliminating the primary source of emboli and avoiding the need for anticoagulant therapy through mechanical occlusion.6,7 The 2016 European Society of Cardiology guidelines about AF explicitly stated that LAAO may be considered for patients with AF who have contraindications for OACs and a IIB indication. 1
With the development of LAAO, device-related thrombus (DRT) formation and embolic stroke after implantation of the occluder have attracted extensive attention. 8 After the implantation of the left atrial appendage occluder, which is perceived as a foreign object by the human immune system, thrombosis might occur on the occluder surface before complete endothelialization of the occluder surface (typically 45 days), leading to thromboembolic events. 9 Therefore, antithrombotic therapy is necessary in the early stage after occluder implantation, and anticoagulants and/or antiplatelet drugs should be administered in the early stages of LAAO. 10
The current guidelines for postimplantation antithrombotic therapy are unclear because of the lack of supporting data and significant heterogeneity encountered in clinical practice.7,11 LAAO is recommended as an alternative treatment strategy in patients with AF who are at high risk of stroke. Ideally, long-term anticoagulant therapy should not required in patients undergoing LAAO. However, if complicated antithrombotic management is needed after the operation, the original intent of improving the quality of life of patients via LAAO is lost. Although the mainstream recommendation is treatment with vitamin K antagonists (VKAs) for 45 days postsurgery, some individuals prefer dual antiplatelet therapy (DAPT). 11 Therefore, the type of antithrombotic drugs to be used and whether long-term antithrombotic therapy is required are issues that require further investigation.
In the present study, the status of postoperative antithrombotic therapy for patients with nonvalvular AF was reviewed. Meta-analysis was used to explore the safety and efficacy of different anticoagulant regimens after LAAO to provide guidance for the development of appropriate anticoagulant regimens.
Methods
Search strategy
We conducted a literature search using PubMed, MEDLINE, EMBASE, Web of Science, and Cochrane Library (February 1, 2020) to identify eligible studies using the keywords “left atrial appendage closure,” “anticoagulant,” and “thrombus.” We also manually searched the reference lists of relevant studies to identify additional publications. The retrieved citations were reviewed independently by two investigators (SL and JW), and any disagreements were solved via discussion. This meta-analysis has been registered on PROSPERO under the registration number CRD42020151460.
Selection criteria
The following inclusion criteria were applied for the eligible studies: 1) prospective or retrospective studies; 2) patients with nonvalvular AF who had undergone LAAO; 3) patients received distinct antithrombotic regimens after LAAO; and 4) the study described the safety and efficacy outcomes of patients undergoing prolonged antithrombotic therapy. The following studies were excluded: 1) studies with <10 subjects; 2) studies with missing data; and 3) case reports, review articles, guidelines, and cell and animal studies. To avoid publication bias, studies that were follow-ups of other included studies or sub-studies of the same cohorts were also excluded from this meta-analysis. When multiple publications from the same study population were found, data from the most inclusive report were used.
Data extraction
A standardized, prepiloted form was used to extract data from the included studies. The following study characteristics were extracted: year of publication, study design, number of patients, and clinical characteristics. The primary efficacy outcomes of this study were as follows: the incidence of DRT formation, systemic thromboembolism, and stroke (hemorrhagic and ischemic). The primary safety outcomes were bleeding (minor bleeding and major bleeding), cardiovascular mortality, and all-cause mortality. DRT was defined as an echo density on the device visible on transesophageal echocardiography. Bleeding events were classified as major (intracranial, retroperitoneal, intraspinal, intraocular, or pericardial hemorrhage; decrease of hemoglobin levels >2 g/dL; and transfusion of ≥2 units of packed red blood cells) and minor (other bleeding events). Cardiovascular death was defined as death caused by a disturbance of the cardiovascular system, and all-cause death was defined as death from any cause.
Quality assessment
The methodological quality and risk of bias of the included studies were evaluated using the Methodological Index for Non-Randomized Studies. 12 This index consists of 12 items, each scored on a scale of 0 to 2, including the evaluation purpose, design, data collection, and follow-up of the study. The maximum ideal score is 16 for noncomparative studies and 24 for comparative studies.
Statistical analysis
The effect estimates were extracted from each study in the form of events in dichotomous data and means or medians for continuous data. Then, the pooled proportion was calculated using the inverse arcsine variance weights. Because of the existence of extreme values, we transformed the proportion of each study using the Freeman–Tukey double arcsine method. The heterogeneity between the studies was analyzed using the I2 statistic and the random–effects model. Funnel plots were generated to observe potential biases, and asymmetry was tested using Egger’s linear regression approach. Forest plots were generated to illustrate the relative effect size of the individual studies on each clinical outcome. The analysis was conducted using R version 3.2.3. P < 0.05 denoted statistical significance.
Results
Study selection
A total of 1065 studies were retrieved. After removing duplicates, 663 studies were subjected to further scanning. After reading the abstract and partial text of each study, unrelated studies, reviews, case reports, studies with unclear outcomes or incomplete data, and studies in which LAAO was combined with other surgeries were excluded. Finally, 32 studies13–44 that satisfied the selection criteria were included in this meta-analysis (Figure 1).

Screening flowchart.
Characteristics of studies
Four studies13,14,25,35 used two different antithrombotic regimens after LAAO. Therefore, each of these four studies was considered to include two research groups, and finally, 36 research groups were included in the analysis. The studies were published between 2011 and 2019, and the number of enrolled patients ranged 12 to 1019. These studies encompassed 4474 patients with nonvalvular AF (mean age, 74.38 ± 6.80 years). The mean CHA2DS2-VASC and HAS-BLED scores were 4.3 ± 1.5 and 3.1 ± 1.0, respectively. Table 1 summarizes the baseline characteristics of the patients in the included studies. The quality of all 32 nonrandomized controlled studies was evaluated, and the quality scores ranged from 8 to 18, indicating that the studies were of moderate quality. The postoperative antithrombotic regimen, follow-up duration, and clinical results are listed in Table 2. The definitions of these outcome events in each study were roughly similar, and the reported data were considered to be under the same definition.
Baseline characteristics of the studied patients.

Data are presented as n (%) unless otherwise indicated.
TIA: transient ischemic attack.
*Complications were not reported in all studies. Hence, the left side lists the number of patients with each complication and the percentage of all reported patients, and the right side lists the total number of reported patients with each complication and the percentage of all included patients.
Antithrombotic regimen and follow-up results of the studies.

DRT, device-related thrombus; NA, not available, NOAC, new oral anticoagulant; VKA, vitamin K antagonist; DAPT, dual antiplatelet therapy; SAPT, single antiplatelet therapy; TIA, transient ischemic attack.
Result of the meta-analysis
Via meta-analysis, we obtained the overall incidence of various endpoint events after LAAO. The heterogeneity among the 36 study groups for DRT was I2 = 49%. The results illustrated that the pooled rate of DRT formation was 1.69% (1.02% to 2.48%). The meta-analysis of systemic thromboembolism consisted of 28 study groups, and the result of heterogeneity testing was I2 = 38%. The pooled rate of systemic thromboembolism was 0.03% (0.00% to 0.39%). In total, 35 study groups were included in the analysis of stroke/transient ischemic attacks (TIA), and the result of heterogeneity testing was I2 = 37%. The pooled rate of stroke/TIA was 1.18% (0.66% to 1.82%). There were 31 study groups for major bleeding, and the result of heterogeneity testing was I2 = 72%. The pooled rate of major bleeding was 2.38% (1.21% to 3.83%). Twenty-six study groups were included in the analysis of minor bleeding, and the result of heterogeneity testing was I2 = 76%. The pooled rate of minor bleeding was 2.32% (1.03% to 3.98%). There were 32 study groups in the analysis of cardiovascular mortality, and the result of heterogeneity testing was I2 = 54%. The results demonstrated that the pooled rate of cardiovascular mortality was 0.27% (0.00% to 0.83%). The analysis of all-cause mortality included 32 study groups, and the result of heterogeneity testing was I2 = 85%. The pooled rate of all-cause mortality was 4.27% (2.50% to 6.41%). Forest plots are presented in Figures 2–3.

Forest plot of efficacy outcomes. (a) forest plot of major DRT, (b) forest plot of systemic thromboembolism, (c) forest plot of stroke/TIA.

Forest plot of safety outcomes. (a) Forest plot of major bleeding, (b) forest plot of minor bleeding, (c) forest plot of cardiovascular mortality and (d) forest plot of all-cause mortality.
Subgroup analysis
We conducted subgroup analyses according to the different postoperative antithrombotic methods (Table 3). The antithrombotic regimens of the 36 study groups were divided into four categories according to the initial antithrombotic drugs: DAPT, new oral anticoagulants (NOACs), VKAs, and single antiplatelet therapy (SAPT). Then, the results for the four antithrombotic schemes were calculated. Regarding DRT, the rates of cardiovascular mortality and all-cause mortality significantly differed among the treatments (P < 0.05). Specifically, SAPT was associated with the highest incidence of DRT events (5.38%), followed by DAPT (2.31%), VKAs (0.89%), and NOACs (0.07%). The incidence of all-cause death decreased in the order of SAPT > DAPT > NOACs > VKAs, whereas that of cardiovascular death decreased in the order of SAPT > DAPT > NOACs = VKAs. Although statistical differences were not detected, DAPT and SAPT were linked to higher rates of thromboembolism, stroke/TIA, and minor bleeding than NOACs and VKAs. Moreover, NOACs were associated with the highest incidence of major bleeding (5.05%).
Subgroup analysis of different antithrombotic methods.
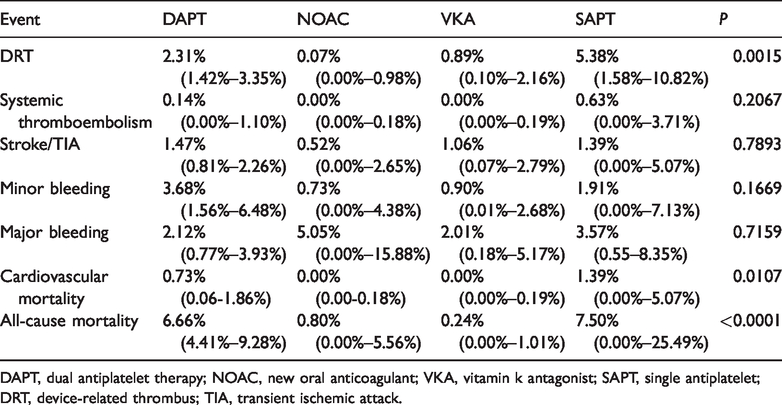
DAPT, dual antiplatelet therapy; NOAC, new oral anticoagulant; VKA, vitamin k antagonist; SAPT, single antiplatelet; DRT, device-related thrombus; TIA, transient ischemic attack.
Heterogeneity analysis
Meta-regression analysis was performed on the outcome indicators of major bleeding, minor bleeding, cardiovascular mortality, and all-cause mortality to assess their high heterogeneity. We analyzed the influence of publication year, sample size, and literature quality on heterogeneity. The difference in sample size was identified as a source of heterogeneity for major bleeding and cardiovascular mortality (P < 0.05), the quality of the literature was identified as a source of heterogeneity for minor bleeding (P < 0.05), whereas none of the three factors was a source of heterogeneity for all-cause mortality.
Publication bias
Regarding publication bias tested using funnel plots and Egger’s test, there was no significant difference in the outcomes of DRT formation, systemic thromboembolism, stroke/TIA, minor/major bleeding, and all-cause mortality, as indicated by the statistically symmetrical funnel plots. However, Egger’s test revealed bias in the outcome of cardiovascular mortality (P < 0.001; Figure 4).
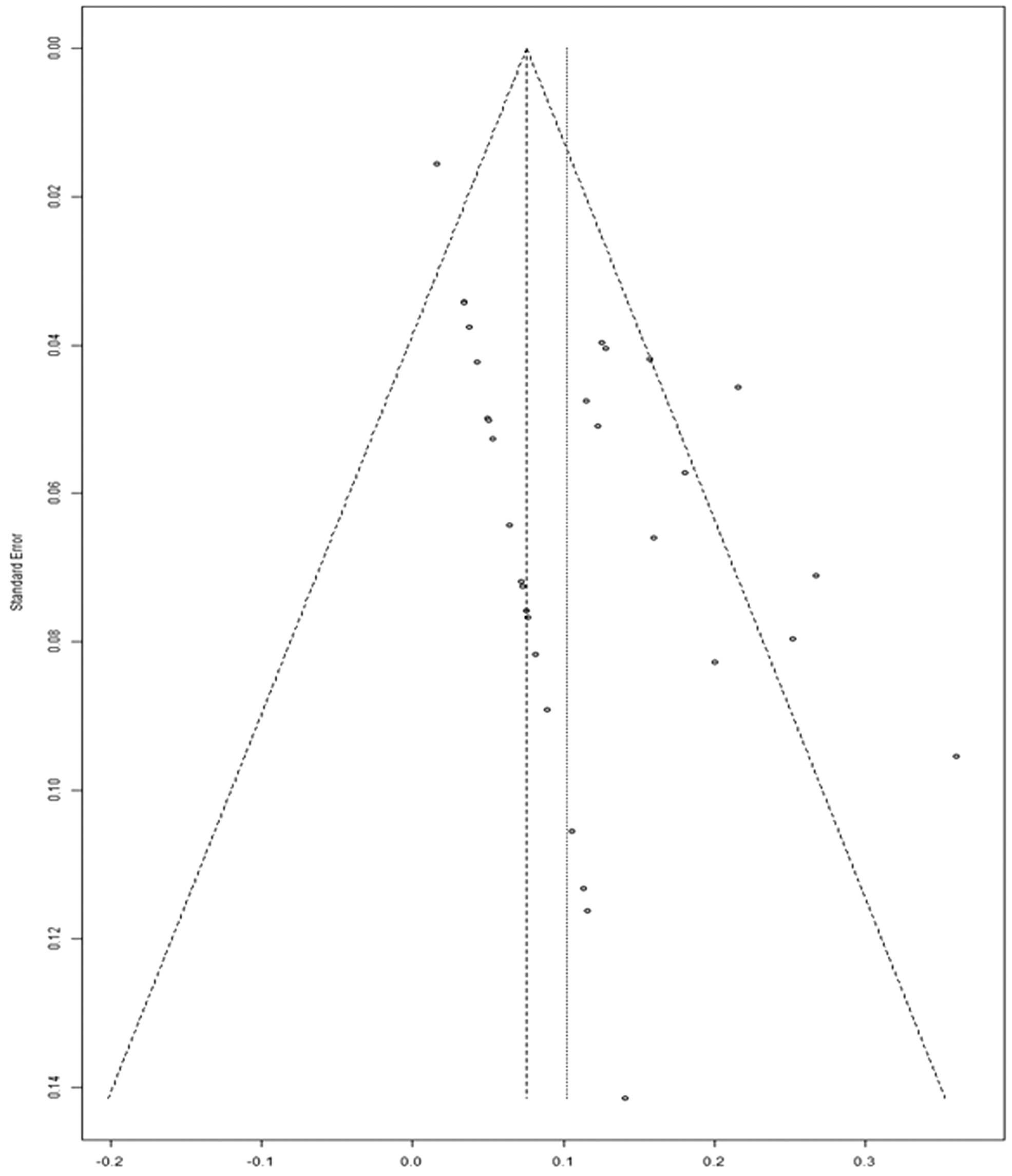
Funnel plot of cardiovascular mortality.
Discussion
This study used meta-analysis to study the incidence of postoperative complications after LAAO and the effects of the antithrombotic regimen. According to our meta-analysis, the incidence of postoperative adverse events for LAAO was as follows: DRT, 1.69%; systemic thromboembolism, 0.03%; stroke/TIA, 1.18%; major bleeding, 2.38%; minor bleeding, 2.32%; cardiovascular mortality, 0.27%; and all-cause mortality, 4.27%. The pooled incidence of adverse events after LAAO surgery was similar to that reported in previous large studies. 45
Presently, the antithrombotic regimens after LAAO surgery are as follows: (a) OAC therapy for 45 days after surgery, DAPT after confirmed successful blockade, and lifelong aspirin monotherapy; (b) DAPT for 3 to 6 months after surgery and then long-term aspirin use; (c) NOACs; and (d) aspirin alone. The PROTECT-AF and PREVAIL trials, two large multicenter randomized controlled studies, primarily compared the efficacy and safety of LAAO to oral warfarin in preventing stroke in patients with AF.46–48 In these two trials, warfarin (+/− aspirin) was administered for 45 days after surgery, followed by DAPT for 6 months and then aspirin. The results illustrated that although a risk of bleeding was plausible in the early stage, regimen (a) was feasible in the high-risk population without anticoagulant contraindications. According to these two studies, regimen (a) was widely adopted. 49 However, the PROTECT-AF and PREVAIL groups did not include patients with contraindications against coagulation, and LAAO is indicated for patients with a high risk of bleeding from OACs. 50 Thus, it was unclear whether antiplatelet therapy could prevent DRT formation.
The subsequent ASAP registry study was the first prospective, multicenter, nonrandomized study of patients with nonvalvular AF with warfarin contraindications. 43 The study enrolled 150 patients after 6 months of postoperative DAPT followed by long-term aspirin use. During follow-up, six (4%) patients developed DRTs; among them, only one patient experienced ischemic stroke on day 341. Based on the results of ASAP, the antiplatelet drug regimen was found to be applicable in several other single-arm registry studies, and the incidences of ischemic stroke and thrombus formation on the device surface were both low during the follow-up period.
In the current analysis, in addition to major bleeding events, antiplatelet regimens (SAPT and DAPT) were linked to higher rates of adverse events than anticoagulant regimens. In particular, significantly lower rates of DRT formation, cardiovascular death, and all-cause death were noted for NOACs and VKAs. We concluded that the efficacy of anticoagulant therapy is significantly better than that of antiplatelet therapy, and the safety of anticoagulant therapy was not inferior to that of antiplatelet therapy. Therefore, we speculated that antiplatelet therapy could not replace anticoagulant therapy. Another paper matched and compared patients treated with anticoagulant or antiplatelet therapy in various large studies, reaching the same conclusion. 51
In some studies, patients were divided into nonanticoagulant contraindication and anticoagulant contraindication groups, and regimens (a) and (b), respectively, were recommended for these groups. 52 In fact, there are patients with relative contraindications for anticoagulant rather than absolute contraindications, such as previous bleeding and poor international normalized ratios. If these patients were classified as having contraindications for anticoagulants and preferences for antiplatelet therapy, then the effectiveness of antithrombotic therapy might be reduced. Some studies suggested that the risk of DRT formation after LAAO could be assessed using the platelet count, ejection fraction, CHA2DS2-VASC score, echocardiographic features, and occlusion conditions.53,54 It is also reported that old age and previous history of ischemic stroke are predictors of DRT formation. 55 Thus, we speculated that patients’ ability to receive anticoagulant therapy should be carefully evaluated; however, no patient should be forced to receive DAPT. For relatively contraindicated patients with an acceptable risk of bleeding, at least 45 days of anticoagulant therapy is recommended.
Finally, according to current data, although NOACs were linked to the highest incidence of major bleeding, these drugs were associated with lower rates of DRT formation, cardiovascular death, and all-cause death than the other regimens, and they carried similar risks of embolism and stroke. These observations were similar to those at a 3-month follow-up in the EWOLUTION study. 56 In addition, Bösche et al. 35 and Enomoto et al. 25 compared the safety and efficacy of NOACs to DAPT and warfarin, respectively, after LAAO, finding that NOAC treatment was safe and effective. Thus, it could be deduced that NOACs have a critical role as antithrombotic therapies after LAAO, but this finding must be substantiated in larger clinical trials. 57
Study limitations
The majority of the articles included in this meta-analysis were single-arm studies. Conversely, few randomized controlled trials were identified, and the level of evidence was not high. The number of studies including different antithrombotic schemes varied greatly, and only two studies assessed SAPT. Furthermore, the present study analyzed the efficacy and safety of various antithrombotic regimens, but it did not distinguish the plausible effects of different types of sealers on postoperative adverse events. In addition, heterogeneity was analyzed in this study. The sample size and study quality explained some of the heterogeneity, but no source of heterogeneity was identified for all-cause mortality. We detected publication bias for cardiovascular mortality outcomes, which may have been attributable to incomplete and inaccurate outcome reporting in some of the lower-quality studies.
Conclusion
Although most patients globally receive DAPT after LAAO surgery, the results of this meta-analysis indicated that anticoagulant therapy is associated with better safety and efficacy than antiplatelet therapy. Concerning patients with nonabsolute anticoagulant contraindications, anticoagulant therapy should be selected. In addition, NOACs have satisfactory development potential, and they may serve as alternatives to VKAs in the future.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Nanjing Medical Science and Technology Development Fund (QRX17060) and Jiangsu Pharmaceutical Association Shire Biopharmaceutical Fund (S201606).