
Abstract
This study aimed to assess the incidence, clinical implications, and treatment strategies of device-related thrombus (DRT) following catheter ablation and percutaneous left atrial appendage occlusion combined in one intervention. A meta-analysis of observational studies was conducted to evaluate the incidence rates, treatment strategies, and clinical implications of DRT. A total of 21 studies describing DRT events and 1 case were included in the current study. The 21 included studies comprised 3 multi-center registries and 18 single-center registries, and we also included 1 case report analyzing the characteristics of DRT. The pooled incidence of DRT in one-stop intervention was 18/1,708 (1.2%; range = 0%-7.3%; 95% CI = 0.7%-1.8%; I 2 = 0). Of these DRT events, 56.25% were diagnosed in the first 3 months after the procedure. All cases were diagnosed via trans-esophagus echocardiogram. All of the patients diagnosed with DRT were prescribed anticoagulation treatment, and 63% (12/19) of the events were reported with an outcome of complete thrombus resolution. The duration of anticoagulation treatment varied greatly, from 30 days to 6 months. Unknown clinical events were reported relating to DRT. Device-related thrombus is an uncommon complication of one-stop intervention. It occurs mainly in the early period following the procedure. Anticoagulation appears to be an appropriate treatment method for dissolving occurrences of DRT.
Keywords
Introduction
Globally, atrial fibrillation presents a significant burden for society, with incidence rates ranging from 1.5% to 2%. 1 Management of this condition involves relieving symptoms and reducing the rate of related complications, especially stroke. Catheter ablation (CA) is being used increasingly frequently as an effective method of rhythm control in cases of atrial fibrillation. The left atrial appendage is reported as the primary source of thrombus formation in nonvalvular atrial fibrillation patients. 2 Percutaneous left atrial appendage occlusion (LAAO) has been applied as an effective alternative to oral anticoagulant (OAC), particularly in patients at high bleeding risk, to decrease the risk of stroke. Recently, Jiang et al conducted a meta-analysis on the efficacy and safety of CA combined with LAAO, concluding that a single procedure combining these 2 approaches is a feasible strategy with significant levels of efficacy and safety. 3 Therefore, one-stop intervention may become increasingly common in clinical practice in the future.
Due to the endothelialization of LAAO, patients still need to receive antithrombotic treatment in the short term. However, the appropriate type and duration of such treatments remain controversial. Furthermore, complications such as device-related thrombus (DRT), while uncommon, do occur in some patients undergoing LAAO. Data from a recent meta-analysis suggest that DRT may be associated with a four- to five-fold increase in ischemic events. 4 However, there is no existing analysis focusing on the incidence of DRT following one-stop intervention.
Therefore, in the current study, we sought to perform a systemic review and meta-analysis to assess the incidence rates, treatment strategies, and clinical implications of DRT in patients undergoing a one-stop intervention.
Methods
Search Strategy
To identify relevant studies, each of the authors (LXH and JTZ) independently searched the archives of PubMed, the Cochrane Library, EMBASE, and the Web of Science, as well as article references, from the inception of each database to August 2020. The keywords used were “atrial fibrillation,” “left atrial appendage occlusion,” “left atrial appendage closure,” “device-related thrombus,” “device-associated thrombus,” “thrombus,” “thrombosis,” and “thrombi.” Any disagreements were resolved through consensus and arbitration by mutual agreement.
Inclusion and Exclusion Criteria
The inclusion criteria were studies concerning patients with nonvalvular atrial fibrillation who received CA and LAAO in one procedure wherein DRT events were reported. The exclusion criteria were as follows: (1) studies involving editorial content, reviews, and duplicate reports; and (2) studies of patients with epicardial left atrial closure.
Data Extraction
The 2 authors each carefully reviewed the included studies independently. Any disagreements between the 2 authors were resolved through consultation with the senior investigator (MT). The following study characteristics were extracted: first author, year of publication, study design, number of patients, clinical characteristics, and data related to DRT (incidence, time of diagnosis, treatment at the time of diagnosis, associated events, resolution rate).
Statistical Analysis
All statistical analysis was performed using Stata 16.0 software (Stata Corp., College Station, TX, USA). The Higgins I-squared (I 2) statistical calculation was used to quantify the degree of heterogeneity. 5 To improve the reliability of the pooled result, the Freeman-Tukey double arcsine transformation was used to obtain the pooled DRT incidence rate. Publication bias was formally assessed using funnel plots and Egger’s linear regression test of funnel plot asymmetry. Forest plots were generated to show the relative effect size of the individual studies on each clinical outcome.
Results
Search and Synthesis of the Literature
A total of 569 articles were initially identified and screened from the literature search. After removing duplicate articles and screening the titles and abstracts of the remaining studies, 40 papers were retrieved for full-text review. Of these, 18 were excluded due to no reported incidence of DRT, duplicate reporting, or patients not having received one-stop intervention. The 21 included studies comprised 3 multi-center registries and 18 single-center registries, and we also included 1 case report analyzing the characteristics of DRT. Figure 1 shows the literature selection process.
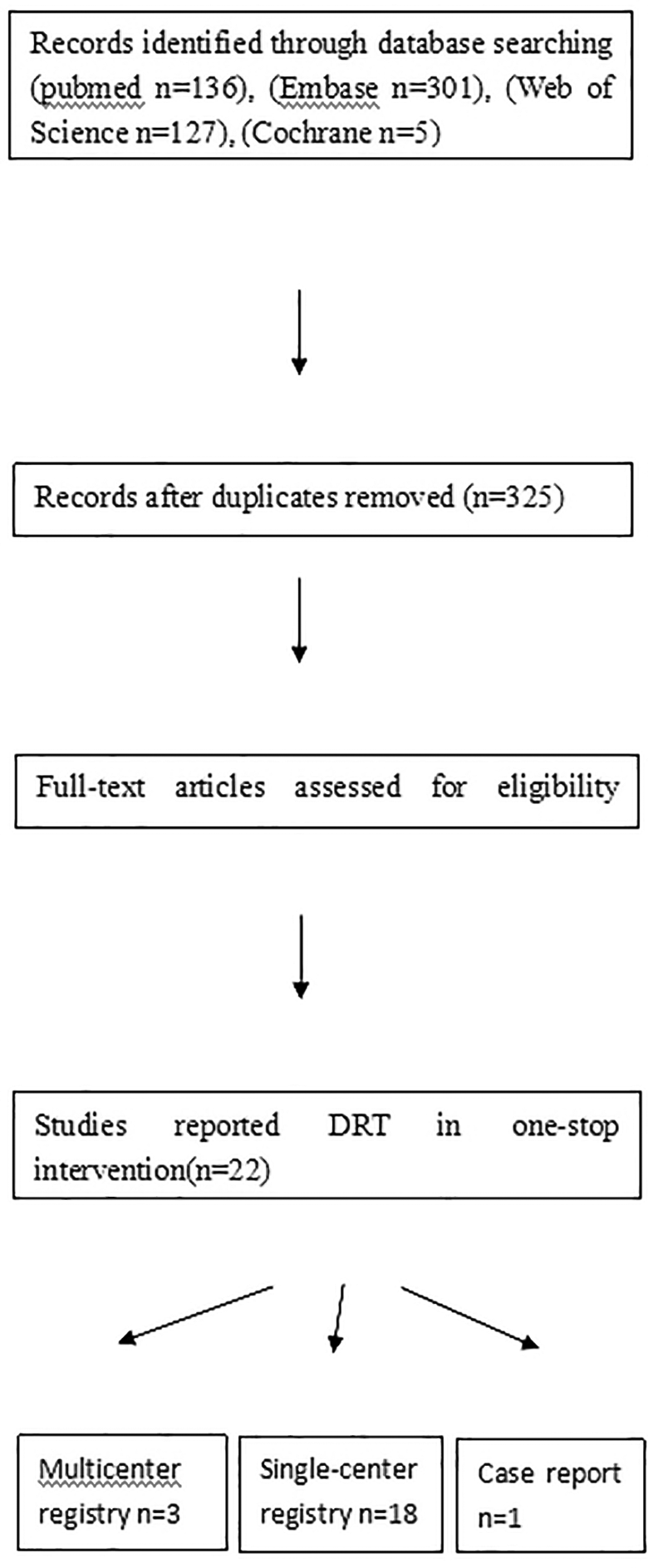
Flow chart of literature selection process.
Incidence of DRT After a One-Stop Intervention
The 21 included studies had a total of 1,708 enrolled patients, with sample sizes ranging from 20 to 349 (Table 1). The Watchman was the most commonly used device (at least 74.5%), and radiofrequency CA was the most commonly applied ablation method (at least 76%). The reported incidence of DRT varied between 0% and 7.3% across the various studies. In larger series (n ≥ 100), the incidence varied from 0% to 2.11%. In total, there were 18 cases of DRT identified out of the 1,708 sample patients (case reports were excluded when calculating the overall incidence of DRT) (Table 2). In our pooled analysis, the mean incidence of DRT was 1.2% (0.7%-1.8%) (Figure 2). The MINORS score ranged from 9 to 12. Publication bias was analyzed using Begg’s test (Figure 3).
Studies With Reported Events of DRT.
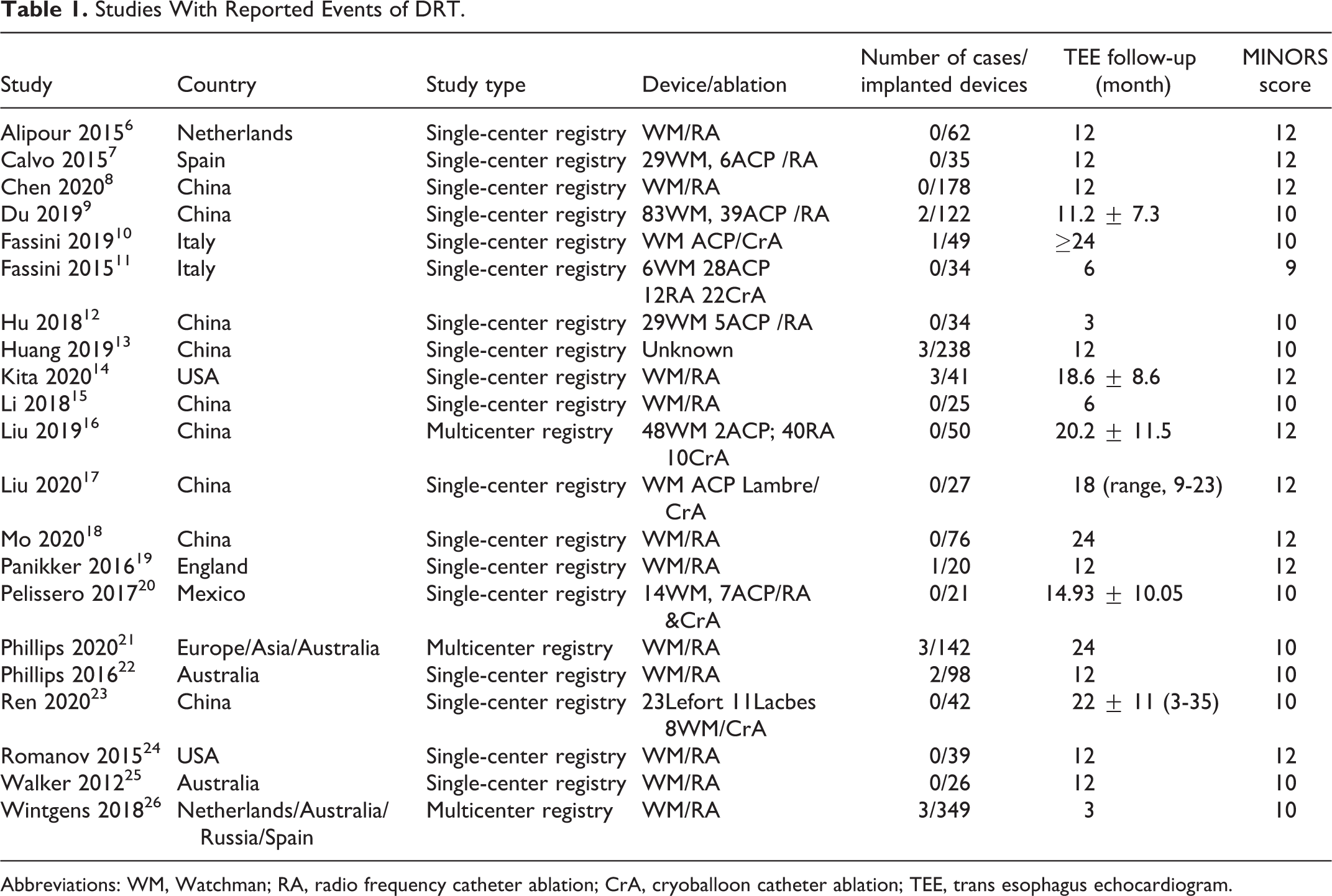
Abbreviations: WM, Watchman; RA, radio frequency catheter ablation; CrA, cryoballoon catheter ablation; TEE, trans esophagus echocardiogram.
Details of the Reported Cases.

Abbreviations: WM, Watchman; RA, radio frequency catheter ablation; CrA, cryballoon catheter ablation; TEE, trans esophagus echocardiogram; Un, unknown; ASA, asprin; OAC, oral anticoagulation; NOAC, novel oral anticoagulation; PAF, paroxysmal atrial fibrillation; CAF, persistent atrial fibrillation; DAPT, dual antiplatelet therapy; SAPT, single antiplatelet therapy.
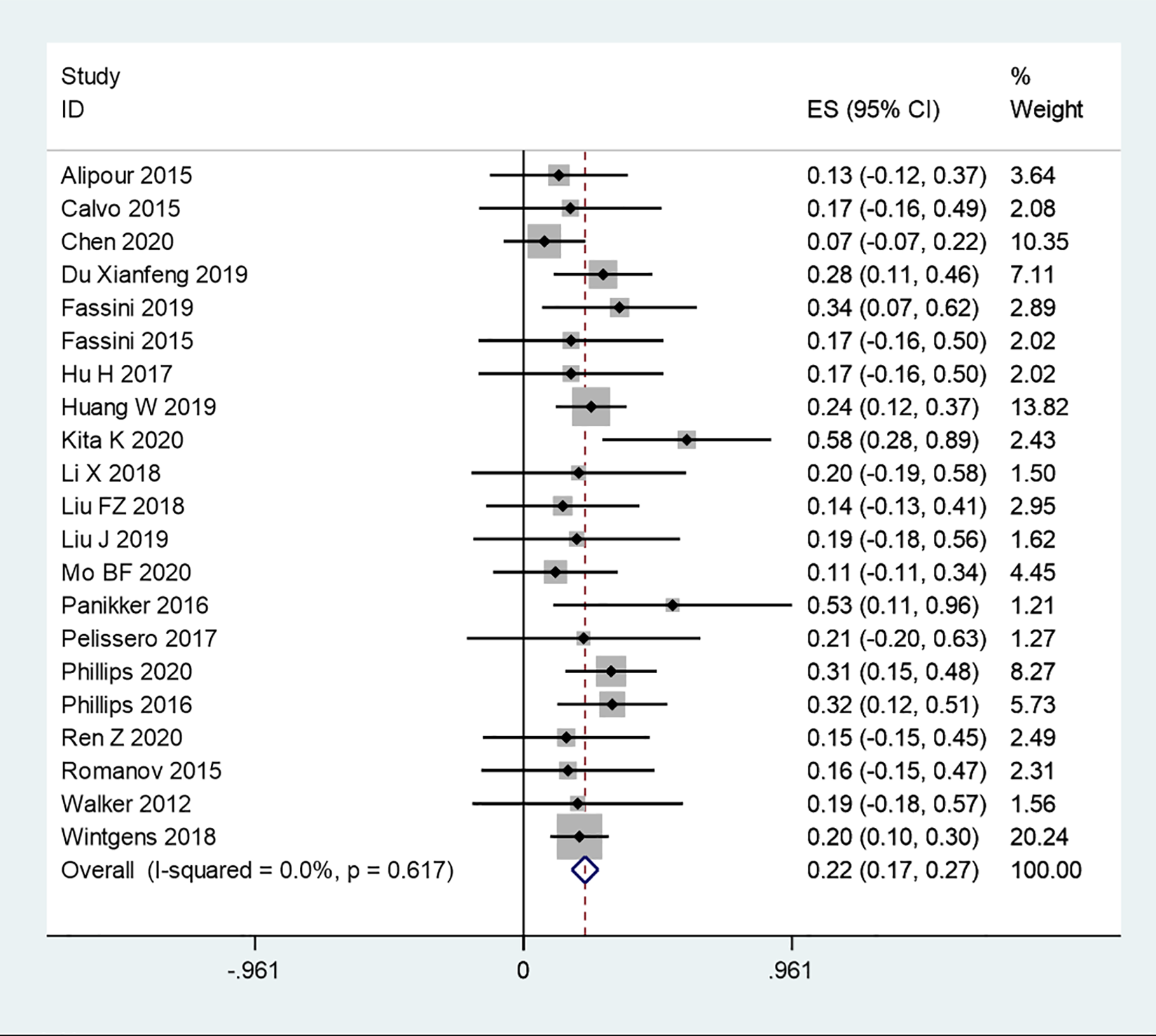
Pooled incidence of DRT following one-stop intervention (Freeman-Tukey double arcsine transformation, fixed effect model).

Assessment of publication bias (Begg’s test).
Timing and Modality of Diagnosis
Of the 16 reported cases of DRT, the majority (9) were diagnosed during the first 3 months following one-stop intervention, 6 were diagnosed at 3-6 months post-intervention, and 1 case was diagnosed between 6 and 12 months post-intervention. No cases were reported more than 12 months after the intervention (Figure 4). In all the reported cases, the diagnosis was made via trans-esophagus echocardiogram (TEE) imaging.
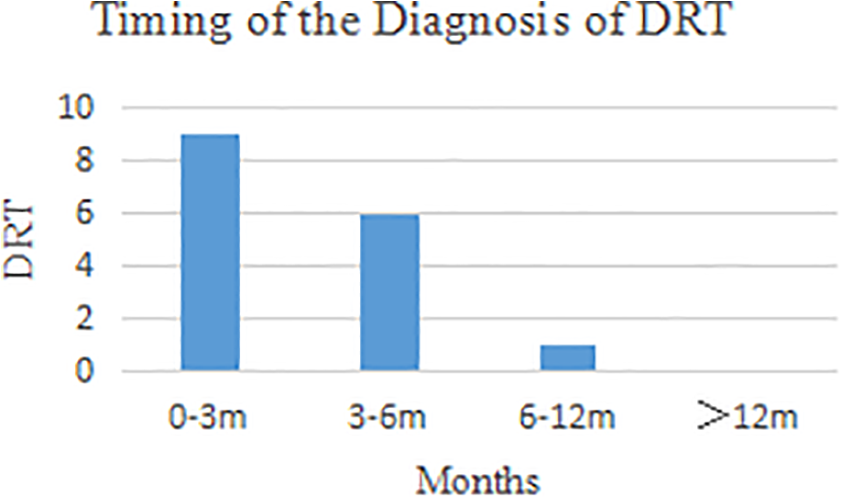
Timing of DRT diagnosis following one-stop intervention.
Clinical Implications, Treatment Strategies, and Predisposing Factors of Device-Related Thrombus
Most of the reported cases of DRT were asymptomatic and discovered by TEE follow-up; however, 1 case was reported with severe ischemic stroke, and the patient then died. 27 Overall, only 0.06% of the one-stop intervention patients in the pooled sample presented with ischemic stroke that was assumed to be related to DRT (1/1,079). All cases were implanted with the Watchman occlusion device. Only 1 of the 16 cases (6.25%) was ablated using cryoballoon ablation.
All patients receiving the one-stop intervention received anticoagulation treatment for different durations, ranging from 45 days to 3 months. In all DRT cases, anticoagulation treatment was continued or restarted following DRT diagnosis. One of these patients received warfarin together with aspirin. Data regarding the duration of antithrombotic treatment were missing in most cases, but from the reported data, the duration of treatment ranged from 1 month to 6 months. Ultimately, complete thrombus resolution was achieved under antithrombotic treatment. The recurrence rate was unknown, because the follow-up time was too short.
Predisposing factors were scarcely mentioned in the reports that we analyzed. Carlson and Doshi reported a case with anticoagulation discontinued at 45 days, 27 and Kita et al recognized that 2 patients with DRT had self-discontinued OAC prematurely. 14
Discussions
The current study is the first meta-analysis focusing on the occurrence of DRT in nonvalvular atrial fibrillation patients treated with concomitant CA and LAAO.
Compared with patients with sinus rhythm, nonvalvular AF patients have a five-fold increase in stroke risk. 28 The LAAO technique has gradually become an alternative to long-term anticoagulation treatment, especially in patients with high bleeding risk, and CA is an effective treatment method for symptomatic AF patients. Recently, Jiang et al conducted a meta-analysis and concluded that the one-stop intervention approach showed significant efficacy and could be safely and successfully performed in AF patients. 3 Because this one-stop intervention can merge a number of procedures within one operation, it may be more cost-effective than other treatment pathways and thus could be a positive prospect for the future. However, the long-term outcomes of this new therapeutic strategy have not been well established. DRT is a potentially serious complication of LAAO. Alkhouli et al conducted a meta-analysis focusing on the occurrence of DRT post-LAAO, and they found that cases of DRT were associated with a four- to five-fold increase in ischemic events. 4 Therefore, we performed the current meta-analysis to study the incidence of DRT following combined CA and LAAO therapy.
In our study, the pooled incidence of DRT was approximately 1.2%, which is consistent with a recent meta-analysis conducted by Jiang et al. 3 Meanwhile, Alkhouli et al reported a slightly higher 4% pooled incidence of DRT post-LAAO (not combined with CA). 4 This could partially be explained by the patients enrolled; for example, patients who are suitable for CA are more likely to maintain their sinus rhythm. Additionally, the true incidence rates might be difficult to evaluate due to the variations in surveillance protocols among the selected studies as well as the small sample sizes. In our study, a majority of the cases of DRT were diagnosed within a short time after the intervention, probably due to the delayed endothelialization process. However, cases of delaying thrombosis should not be neglected. They could be secondary to mechanical factors or systemic patient factors such low ejection fraction (EF) and spontaneous echo contrast. The formation mechanism of DRT is still obscure, and there is limited evidence in relation to one-stop interventions. Multiple studies have declared the proinflammatory effects of ablation within the left atrium, and left atrial appendage (LAA) may contribute to the formation of DRT. 29,30
One of the cases in our analysis was reported with severe stroke following diagnosis of DRT. Dukkipati et al have previously highlighted a relationship between DRT and ischemic events, 31 and Alkhouli et al’s meta-analysis showed that DRT is associated with a four- to five-fold increase in ischemic events. 4 The PROTECT AF study reported a DRT-associated annualized stroke rate of 0.3% per 100 patient-years. 32 According to the multi-center Amplatzer Cardiac Plug (ACP) registry, no embolic complications were reported in more than 1,000 patients, and no relationship was identified between DRT and stroke. 33 Although it seems to be reasonable to regard DRT as contributing to ischemic stroke, we are unable to draw a substantial conclusion based on the currently available data.
The occurrence mechanism of DRT appears to be multifactorial and very complex. Identifying predictors is very important for recognizing patients at high risk of DRT formation and taking effective preventive measures. In the literature regarding one-stop interventions, a limited amount of data has been gathered to date; therefore, conclusive evidence regarding these predictors has not yet been accumulated. According to evidence from individual studies based on LAAO-only procedures, several factors could be independent predisposing factors for DRT, including both clinical factors (stroke history, permanent atrial fibrillation (AF), advanced age, large LAA, low EF, vascular disease history, higher CHA2DS2-VASc score, etc.) and procedural factors (deep implantation, lack of discharge antithrombotic treatment, etc.). 31,33 –36 However, Pracon et al’s study demonstrated no clear association between post-LAAO antithrombotic regimen and DRT incidence. 36
To date, no consensus has been reached regarding the treatment of DRT arising following one-stop intervention. An overwhelming majority of the DRT cases reported in the studies selected for our analysis were completely dissolved after anticoagulation. Only 2 cases were mentioned the kind of NOAC in detail. Recently, Calabrò et al reviewed current evidence supporting the use of NOACs in patients with established atrial and/or left atrial appendage thrombosis. In those patients, the rationale for the use of NOACs is based on their effectiveness in limiting fibrin accretion, thereby favoring endogenous fibrinolysis, 37 resulting in the resolution of already formed thrombi. In their opinion, NOACs may be considered as first-line therapy in patients with AF and documented left atrial/LAA thrombosis. NOAC can mostly minimize the risk of intracranial bleeding, as well as the most severe bleeding. According to the mechanism of NOAC dissolving thrombi, it may be reasonable to apply NOAC to DRT. However, the evidence on the treatment DRT is still scarce. 38 One small-scale study described a recurrence of DRT, and the rate was 35%. 39 While, applying antithrombotic therapy to dissolve a DRT may increase the risk of a bleeding complication; therefore, the treatment of DRT still needs to be investigated carefully.
Limitations
All the studies analyzed were observational studies with DRT reported as an adverse event. Most of the selected studies did not describe the thrombus characteristics. The demographics, treatment strategies, and prognosis data of the patients with DRT were also unrevealed. The proportion of DRT cases following one-stop intervention was very small, so it was difficult to achieve any substantial conclusion regarding predisposing factors and clinical implications of DRT. In addition, the definition of DRT is not unified, so diagnosis can be operator-dependent. Finally, the follow-up duration in the selected studies may not have been long enough to observe later occurrences of DRT.
Conclusions
Our meta-analysis suggests that cases of DRT are infrequent following combined CA and LAAO one-stop intervention, with most cases occurring relatively soon after the procedure. More and larger prospective studies are needed to verify the real prevalence of DRT following this one-stop procedure and to investigate predisposing factors, treatment strategies, and clinical implications.
Footnotes
Acknowledgment
The authors would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.