
Abstract
Ceftobiprole is a new parenterally administered fifth generation cephalosporin which has been shown to have antimicrobial activity against a broad range of bacteria, and specifically against methicillin-resistant Staphylococcus aureus (MRSA) in complicated skin and skin structure infections (cSSSIs), with a cure rate non-inferior to vancomycin and ceftazidime. It has increased stability against β-lactamases and an increased affinity for PBP2’ in MRSA strains. Ceftobiprole has shown a low tendency to select for resistance, and because it is excreted mainly in the urine, a low potential for adverse drug interactions. It has been shown to cause few mild to moderate adverse effects in patients. The broad-spectrum of activity makes it an excellent choice for initial monotherapy in cSSSIs. There is also promise for use in all types of pneumonia, and synergistic possibilities with aminoglycoside and fluoroquinolone drugs. It is awaiting final approval by the FDA.
Introduction
In the early days of antimicrobial discovery, scientists were able to build an arsenal of drugs that they thought would conquer any microorganism: the sulfa drugs, penicillins, streptomycin, cephalosporins. When it became apparent that the microorganisms were capable of becoming antimicrobial-resistant, scientists began to look for new antimicrobial agents, both in nature, and by adjusting the structures of the original drugs. This led to a battery of antimicrobial agent families (often with several generations), and classification into groups based on the antimicrobial mechanism used. Even with this greatly enlarged arsenal, the fight against microbial diseases still rages on, with no apparent end or winner in sight. Most of the microorganisms that we are battling have multiple antimicrobial mechanisms, and we are now faced with some that are resistant to most, if not all, of the major drug classes. Methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), the ESBL (extended-spectrum β-lactamase) gram-negative organisms (such as Escherichia coli and Klebsiella pneumonia), and extensively drug-resistant tuberculosis (XDR-TB), among others, are taking a huge toll on lives and healthcare costs around the world. The biggest obstacle in the microbe-human battle is the length of time (and astronomical cost) associated with having a new drug approved for patient use. But the drug discovery scientists are pushing forward, hoping that the next drug will be the one to turn the battle in favor of the human hosts.
The largest group of antimicrobials are the β-lactam drugs. These drugs are all based on a core structure containing a β-lactam ring. The penicillins were the first β-lactam drugs to be used in humans. All β-lactam drugs work by binding to bacterial membrane-bound transpeptidases, also known as penicillin-binding proteins (PBPs), as substrate analogs. This covalent binding inhibits the ability of the transpeptidases to catalyze the cross-linking of peptidoglycan subunits (which form new bacterial cell walls), resulting in cell lysis. Bacteria have multiple PBPs which may have various specialized functions, and the various PBPs differ in sensitivity to the individual β-lactam drugs. Resistance to the β-lactam drugs can occur via several mechanisms including: production of modified PBPs; production of β-lactamases, enzymes which can hydrolyze the β-lactam ring rendering the drug useless; changing the permeability of the outer membrane to restrict passage of the drugs; and use of efflux pumps to rid the cell of the drug. Even with all of these potential resistance mechanisms, because β-lactam drugs have relatively low toxicity, have a relatively broad-spectrum of activity, and relatively low production costs, scientists continue to work on adaptations of these drugs as the best possible means to finding ways to deal with the increasing number of multi-drug resistant organisms.1,2
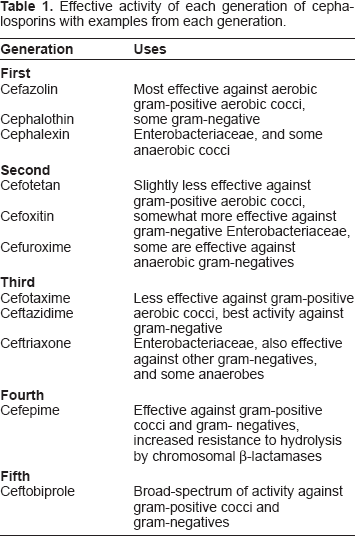
The cephalosporins were first used in the 1960's. These drugs can be classified into generations based loosely on features of antimicrobial activity (Table 1). The core structure is based on the structure of penicillin with the addition of a second side chain. Further changes to the side chains have produced the various cephalosporin family members. The cephalosporins are generally more stable to β-lactamases, and are more broad-spectrum than the penicillins. While each generation of cephalosporins improved certain aspects of the spectrum of antimicrobial activity, by the fourth generation, the ever growing problem of multiple drug resistance was still not solved. MRSA and the ESBL organisms remained resistant to the cephalosporins. With the fifth generation of cephalosporins there is hope that a new weapon, ceftobiprole, will be effective against MRSA, in addition to having a broad-spectrum of activity against the organisms usually susceptible to the third- and fourth-generation cephalosporins.
Effective activity of each generation of cephalosporins with examples from each generation.
Ceftobiprole is considered to be a fifth generation cephalosporin, and is administered parenterally as the prodrug ceftobiprole medocaril (Fig. 1). 3 It has been approved for use in Canada, Switzerland, Russia, Azerbaijan, Ukraine, and Hong Kong for treatment of complicated skin and skin structure infections (cSSSIs) caused by MRSA. It has also been pending approval in the United States, having been granted FDA fast-track status in 2003 for cSSSIs and hospital-acquired pneumonia caused by MRSA, but questions by the FDA about some portions of the phase III clinical trials have caused withdrawal of marketing in Canada and Switzerland. The FDA felt that the studies at almost one third of the clinical trial sites had been inadequately monitored, and a delay in approval in the US is pending the completion of two new and adequately controlled trials.4–6 In addition, developer, Basilea Pharmaceutica Ltd., has recently acquired full rights to the drug from Cilag GmbH International, a Johnson & Johnson company, which marketed the product outside of the US. 7 Basilea has an agreement with Ortho-McNeil Pharmaceutical (Johnson & Johnson) which will market the product in the US. 3
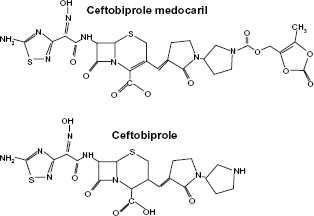
Prodrug–-ceftobiprole medocaril, and active drug–-Ceftobiprole. Adapted with permission. 43
Mechanisms of Action, Metabolism and Pharmacokinetic Profile
Ceftobiprole mediates antimicrobial effects by the same basic mechanism as all β-lactam drugs, via inhibition of cell wall biosynthesis after binding to PBPs. It has greatly increased stability against β-lactamases due to an oxyimino aminothiazolyl substituent at position 7 of the cephalosporin nucleus. This makes it a poor substrate for most class A and C β-lactamases, leading to a broad spectrum of activity against both Gram-positive and Gram-negative bacteria. In addition to an affinity for most PBPs, there is also an increased affinity for PBP2’ (or PBP2a–-which confers resistance in MRSA strains), due to a vinylpyrrolidinone moiety at position 3 of the cephalosporin nucleus. 8 This large hydrophobic side chain causes a conformational change in the PBP2', and forms a stable acyl-enzyme complex so there is only a very slow hydrolysis of the molecule.9,10 The MIC for MRSA strains is typically ≤2 μg/ml, compared to >64 μg/ml for ceftriaxone and >128 μg/ml for ceftazidime. Ceftobiprole also shows increased affinity for PBP2x in penicillin-resistant strains of Streptococcus pneumoniae, with an MIC of 1 μg/ml, compared to 8 μg/ml for ceftriaxone. 11
Ceftobiprole has shown a low tendency to select for resistance. In multipassage resistance studies, there was no development of stable resistance in MRSA, penicillin-resistant S. pneumoniae, Haemophilus influenzae, or Moraxella catarrhalis.12,13 While ceftobiprole is stable to hydrolysis by common β-lactamases in Gram-negative bacteria, it is susceptible to hydrolysis by many of the ESBL β-lactamase strains, having similar spectrum of activity against the ESBL strains as that of other cephalosporins, such as cefepime, cefotaxime, ceftazidime, and ceftriaxone. 14 It is also susceptible to class B metallo-β-lactamases.15,16 Elevation in MICs has been demonstrated in Pseudomonas aeruginosa strains after exposure to ceftobiprole, with initial MICs ranging from 2 to 8 μg/ml, then increasing to a range of 8 to 32 μg/ml. The mechanism involved in this resistance is through increased expression (5- to 168-fold higher) of the MexXY efflux pump, and not due to increased expression of the P. aeruginosa chromosomal AmpC β-lactamase.17,18
Ceftobiprole is predominately excreted unchanged in the urine, and the highest concentration of the drug is detected in the urine within the first 2 h after the start of administration, with very little of the prodrug detected in the urine (0.7%–2.2% of dose).6,19 The renal clearance of ceftobiprole ranges from 4.1 to 5.1 liters/h (68.3–85.0 ml/min). 6 Patients with impaired renal function may need to have dosage adjustments. The National Kidney Foundation defines renal impairment using glomerular filtration rate (GFR) expressed as mL/min per 1.73 m2. 20 Patients with mild renal impairment (GFR of 60–89) do not need to adjust the dosage. Those patients with moderate renal impairment (GFR of 30–59) should use a dose of 500 mg every 12 hours, infused over 120 minutes. Patients with severe renal impairment (GFR of 15–29) should use a dose of 250 mg every 12 hours, infused over 120 minutes. The use of ceftobiprole is not recommended for patients on dialysis. 21
Janssen-Ortho, Inc., has also recommended doses and dose adjustments for cSSSIs with and without diabetic foot infections. For cSSSIs without diabetic foot infection, the recommended dose for infections involving only Gram-positive bacteria is 500 mg every 12 hours, infused over 60 minutes, for 7–14 days. For cSSSIs without diabetic foot infection involving only Gram-negative bacteria, or mixed Gram-positive and Gram-negative bacteria, the recommended dose is 500 mg every 8 hours, infused over 120 minutes, for 7–14 days. For cSSSIs with diabetic foot infection, the recommended dose for all infection types is 500 mg every 8 hours, infused over 120 minutes, for 7–14 days. 21
Ceftobiprole is administered as the prodrug to improve water solubility. It is rapidly hydrolyzed by plasma esterases to the active drug, with very little (<2%) of the prodrug detectable after the 30 minute infusion is completed.22,23 The peak plasma concentration occurs at the end of the 30 minute infusion, with the concentration then decreasing in a biphasic manner consistent with rapid distribution from the circulation, and the volume of distribution (18–20 liters) equal to that in the extracellular fluid compartment of adults.19,22 Peak concentrations are 35.5 μg/ml for a single dose of 500 mg and 59.6 μg/ml for a single dose of 750 mg. It has an estimated half-life of 3–4 hours, which allows for administration twice a day without drug accumulation.19,24 In a study done using patients with cSSSIs, it was shown that when given doses of 750 mg twice a day, the plasma concentration stayed above 2 μg/ml for >80% of the dosing interval. 25 A study performed to examine the penetration of ceftobiprole from the plasma into subcutaneous adipose tissue and skeletal muscle found that ceftobiprole distributes into the interstitial space fluid of subcutaneous adipose tissue and skeletal muscle in a manner that correlates with other cephalosporin drugs. This is important for cSSSIs, because the causative organism is often found in these fluid spaces. The concentration of ceftobiprole in the interstitial space fluid of these tissues remained above 2 μg/ml for at least half of the dosing interval. 26
There is limited data on tissue distribution of ceftobiprole in other human tissues. A study done on mice with pneumonia showed good penetration of ceftobiprole into the epithelial lining fluid and lung tissue. 27
Antimicrobial Efficacy
Ceftobiprole has been shown to have activity against a broad array of bacteria, and it will be particularly useful for treatment of MRSA infections. Data has been collected on bacteria samples provided by hundreds of locations around the globe for the last twelve years or more. Investigators have tested the activity of ceftobiprole against a great many different species of bacteria, and so have obtained vital information on this drug. A broad cross-section of this data has been used to compile the information in Table 2.28–37
In vitro activity of ceftobiprole against some clinically important bacteria.
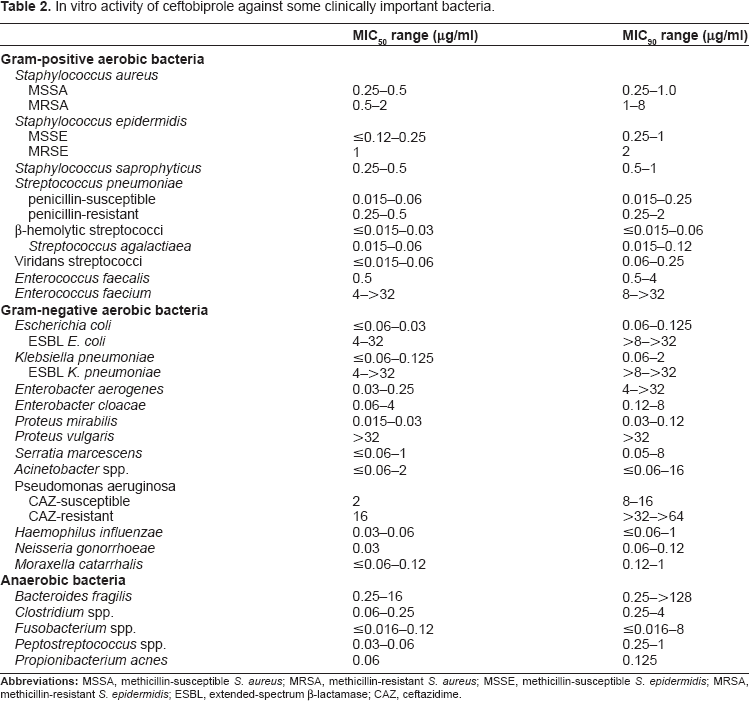
While ceftobiprole generally has good activity against aerobic Gram-positive cocci (especially MRSA), it is not very effective against the enterococci, and should probably not be considered for treatment of Enterococcus faecium infections (as monotherapy). The effectiveness of ceftobiprole against Gram-negative aerobic bacteria varies greatly. It has good activity against non-ESBL Escherichia coli and Klebsiella pneumoniae, but is clearly not effective against the ESBL strains of those bacteria. In addition, there is questionable activity against some Enterobacter and Serratia species, and has virtually no activity against Proteus vulgaris (but good activity against P. mirabilis). Use against Pseudomonas aeruginosa is highly questionable, especially against the ceftazidime-resistant strains, which appear to be totally resistant. Acinetobacter species have shown wide variability, with the susceptibility of A. baumannii being questionable. Susceptibility data for A. baumannii shows an MIC range of 0.5–>64 mg/L, with a bimodal pattern.31,38 Most Stenotrophomonas maltophilia isolates have been shown to be non-susceptible to ceftobiprole, having MICs of >32–>64 mg/L.29,31,38 Other Gram-negative bacteria that are susceptible to ceftobiprole include Haemophilus influenzae, Neisseria gonorrhoeae, and Moraxella catarrhalis.
Ceftobiprole has also shown activity against many anaerobic bacteria, especially the anaerobic Gram-positive cocci (which correlates with the activity against the aerobic Gram-positive cocci), such as the Peptostreptococcus species. Some Bacteroides species may not be susceptible, especially B. fragilis strains. Ceftobiprole has good activity against most Clostridium species, with the exception of C. difficile. The limited data available for C. difficile suggests that since the activity of ceftobiprole may not be optimal, that patients given ceftobiprole should be monitored for possible pseudomembranous colitis development. 33 Ceftobiprole also shown good activity against Propionibacterium acnes and most Fusarium species.30,35
There are undoubtedly many more species of bacteria that are susceptible to ceftobiprole, but the ones that are the most likely to be isolated from complicated infections have been included here. It is to be presumed that the key role for ceftobiprole will be for treatment of MRSA infections. Hopefully, widespread resistance to ceftobiprole will not become an issue for a long time.
Synergy
Ceftobiprole has not been shown to be effective against certain bacteria when used alone (mono-therapy), so studies into the possibility of combination therapy are vital. The discovery of a synergistic relationship with one or more drugs or drug classes will add greatly to the treatment of complicated infections, especially in this era of ever increasing antimicrobial-resistance in so many bacteria. Synergism has been defined as an increase in killing at 24 hours of ≥2-log10-CFUs/ml compared to the effect of the drug used alone. 39
Most of the studies involve the combination of ceftobiprole with either an aminoglycoside or a fluoroquinolone drug, and there have been mixed results. One study looked at the possible synergism between ceftobiprole and gentamicin against various Gram-positive cocci. There was no synergism against Staphylococcus aureus or Enterococcus faecalis strains, but there was synergism against some strains of coagnegative staphylococci and Enterococcus faecium. 40 A second study tested the effects of combining ceftobiprole and vancomycin against strains of S. aureus, and found no synergistic effects.41,42 A third study tested the combination of ceftobiprole and tobramycin against MRSA strains, and did not find any synergistic effect against either community acquired- or hospital acquired-MRSA strains. 39 Another study combining ceftobiprole and gentamicin or streptomycin against strains of E. faecalis, found that there was synergism with both combinations against some strains. 43
Two studies testing combination drugs against Pseudomonas aeruginosa strains had varied results. One study showed a synergistic effect for ceftobiprole and levofloxacin against P. aeruginosa.42,44 The other study tested combinations of ceftobiprole with amikacin, ciprofloxacin, levofloxacin, or tobramycin. Most effects were simply additive, but 27% of the strains tested with tobramycin, 12% of the strains tested with amikacin, and 10% of the strains tested with either ciprofloxacin or levofloxacin in combination showed synergistic effects.43,46 These results suggest that for multi-drug resistant bacterial strains, a combination of ceftobiprole with either an aminoglycoside or a fluoroquinolone drug may greatly improve the outcome of the treatment.
Clinical Studies
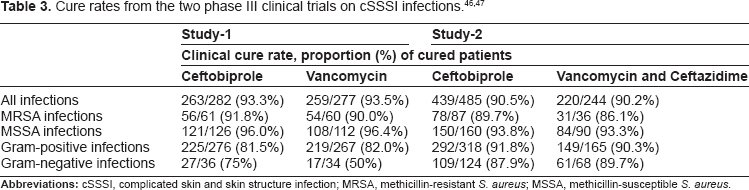
There have been two major phase III double-blind, randomized clinical trials conducted using patients with cSSSIs. The first trial was conducted comparing the use of ceftobiprole with the use of vancomycin in the treatment of cSSSIs caused by Gram-positive bacteria, and the second trial compared the use of ceftobiprole with a drug combination of vancomycin and ceftazidime in the treatment of cSSSIs.46,47 The first study collected data on patients from 101 study sites located on five continents (Europe, Asia, Africa, South America, North America). There were a total of 784 randomized patients, of whom 613 had an isolated pathogen upon entry into the trial. Complete data was collected on 559 patients, 282 treated with ceftobiprole (500 mg, infused over 60 min, every 12 hours) and 277 treated with vancomycin (1000 mg, infused over 60 min, every 12 hours) for 7 to 14 days. The types of cSSSIs assessed included abscesses, wounds, and cellulitis. The cure rates (cure being defined as resolution of all signs and symptoms of infection, or no further antimicrobial therapy necessary) were 93.3% for those treated with ceftobiprole, and 93.5% for those treated with vancomycin, therefore ceftobiprole was found to be noninferior to vancomycin for cSSSIs caused by Gram-positive bacteria. The cure rates were similar for those patients whose infections were caused by MRSA: 91.8% for those treated with ceftobiprole and 90.0% for those treated with vancomycin. 46
The second study used data collected from 92 sites on the same five continents as the first study. There were a total of 828 randomized patients. Complete data was collected on 729 patients, 485 treated with ceftobiprole (500 mg, infused over 120 min, every 8 hours), and 434 patients treated with vancomycin (1000 mg, infused over 60 min, every 12 hours) and ceftazidime (1000 mg, infused over 120 min, every 8 hours) for 7 to 14 days. The types of cSSSIs assessed included: diabetic wound infections, wounds, abscesses, and cellulitis. The cure rates were 90.5% for those treated with ceftobiprole, and 90.2% for those treated with both vancomycin and ceftazidime. The cure rates were compared for infections caused by Gram-negative bacteria and those caused by Gram-positive bacteria. Those patients who were treated with ceftobiprole had cure rates of 91.8% for Gram-positive bacteria, and 87.9% for Gram-negative bacteria. Those treated with the vancomycin and ceftazidime combination had cure rates of 90.3% for Gram-positive bacteria, and 89.7% for Gram-negative bacteria (Table 3). There were 12 ceftobiprole-treated patients with infections in which P. aeruginosa was the only isolate. Of these 12, 9 (75%) were cured, 6 of these 9 isolates had MICs of ≤4 μg/mL, and all 3 isolates from patients not cured had MICs of ≥8 μg/mL. 47
Additional phase III studies have been conducted assessing the effectiveness of ceftobiprole for treatment of pneumonia. One study was a double-blind, multicenter study using 781 patients with nosocomial pneumonia or ventilator-associated pneumonia (VAP). These patients were treated with either ceftobiprole (500 mg every 8 hours, infused over 120 min), or ceftazidime (2000 mg every 8 hours, infused over 120 min) with linezolid (600 mg every 12 hours, infused over 60 min), for 7 to 14 days. The cure rates were 69.3% for those treated with ceftobiprole, and 71.6% for those treated with ceftazidime plus linezolid. The cure rates for pneumonia that did not include VAPs were 77.4% for those treated with ceftobiprole, and 76.3% for those treated with ceftazidime plus linezolid.48,49
A second phase III randomized, double-blind study assessed the efficacy of using ceftobiprole compared with ceftriaxone with or without linezolid for patients who had been hospitalized with community-acquired pneumonia (CAP). A total of 666 patients were treated with either ceftobiprole (500 mg every 8 hours, infused over 120 min) with or without a placebo (every 12 hours, infused over 60 min), or ceftriaxone (2000 mg once daily, infused over 30 minutes) with or without linezolid (600 mg every 12 hours, infused over 60 min). The cure rates were 86.7% for those treated with ceftobiprole, and 87.6% for those treated with ceftriaxone (with or without linezolid).48,50
Safety
Ceftobiprole was well tolerated in the single-dose and multiple-dose studies performed using healthy volunteers. Less than 25% of the participants experienced one or more mild to moderate adverse event (AE). The most commonly reported were a mild taste disturbance (a caramel-like taste during the infusion period), nausea and/or vomiting, and transient headache. None of these AEs required any treatment.19,24
In the phase III clinical trials using patients with cSSSIs, approximately half of the participants reported experiencing an AE. There was no significant difference in total AEs between those treated with ceftobiprole and those treated with vancomycin with or without ceftazidime. The most commonly reported were nausea, headache, vomiting, and diarrhea. Most of these were mild to moderate in severity. There were 7 deaths among the participants (4 receiving ceftobiprole and 3 receiving vancomycin), none of which were related to the study drugs. During these trials, the participants showed no difference in mean laboratory test results that included values for white blood cell count and differential, hemoglobin, red blood cell count, platelet count, serum electrolytes, glucose, blood urea nitrogen, creatinine, bilirubin, uric acid, alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyltransferase (GGT), and normal urinalysis.46,47
Ceftobiprole has not been found to have any drug interactions, but there is insufficient information available on this issue. In addition, patients and providers should be aware that ceftobiprole could cause the same type of hypersensitivity reaction seen in people who are allergic to β-lactam drugs. While there is no data available on ceftobiprole cross-reactivity with penicillin allergy, studies on cross-reactivity of third generation cephalosporins have shown very low risk. Ceftazidime had a cross-reactivity of 0.06% in patients with a known history of penicillin/amoxicillin allergy. 51
Place in Therapy
Ceftobiprole has a broad-spectrum of antimicrobial activity which makes it an excellent choice for early option monotherapy in complicated infections, especially where MRSA is suspected to be a causative agent. The clinical trials using patients with cSSSIs have shown it to be extremely effective on those types of infections. There is also promising data for use on pneumonia infections. It has good activity against most Gram-positive cocci, especially against MRSA and penicillin-resistant S. pneumoniae. In addition, it shows good activity against many Gram-negative bacteria (not ESBL strains), and some anaerobes. In instances where it might not be the best choice for monotherapy (eg, E. faecium, ESBL strains, ceftazidime-resistant P. aeruginosa infections), it could still be valuable in combination with another drug such as vancomycin. The synergism studies show promise that ceftobiprole may have a synergistic effect when used in combination with some of the aminoglycoside or fluoroquinolone drugs.
Conclusions
The most common cause of cSSSIs is S. aureus, and most often a MRSA strain. The steady increase in the number of MRSA cases worldwide has made a top priority of finding a way to treat these infections. Ceftobiprole has been shown to have excellent activity against MRSA strains, with a relatively low potential for development of resistance. At this current moment that makes ceftobiprole an important weapon in the fight against MRSA. In addition, cSSSIs and other complicated infections may be polymicrobial, so a broad-spectrum drug is usually the best choice for initial therapy. Other types of complicated infections may be caused by other Gram-positive cocci, Gram-negative bacteria, or anaerobes. Since ceftobiprole has a such a broad-spectrum of antimicrobial activity, it can be a very versatile option for all types of complicated infections. There is encouraging data on treatment of community-acquired, nosocomial, and ventilation-acquired pneumonia infections. More data is needed to assess its potential for use in septicemia and other serious infections such as complicated intra-abdominal infections. The possibilities for use of ceftobiprole in combination with other drugs is very promising, especially if synergistic effects can be achieved. Ceftobiprole has been shown to have relatively low levels of mild adverse effects during treatment, and a has a low potential for interaction with other types of medication, which makes it a patient friendly drug.
Disclosures
This manuscript has been read and approved by the author. This paper is unique and not under consideration by any other publication and has not been published elsewhere. The author and peer reviewers report no conflicts of interest. The author confirms that they have permission to reproduce any copyrighted material.