
Abstract
The development of nelarabine as a therapeutic agent to treat various forms of hematologic malignancies spans more than 40 years. From the bench top to the bedside, basic scientists and clinical scientists in the pharmaceutical industry and academia collaborated with regulatory agencies to bring this drug to the market. Studies have demonstrated efficacy in treating T-cell leukemia and lymphoma and further work is ongoing as new dosing schedules of nelarabine and combinations with other chemotherapeutic agents are explored. This work is aimed at maximizing the therapeutic outcome while minimizing the potential neurotoxicity that has been identified with nelarabine. This brief review provides some of the “milestones” of development and presents a summary of the efforts of the pharmaceutical industry, academia, and government. Nelarabine, synthesized in the late 1970's as a prodrug of 9-β-D-arabinofuranosylguanine (ara-G), is still undergoing rigorous clinical evaluations in an effort to identify its optimal use.
Introduction
The pertinent review entitled “Nelarabine in the treatment of T-cell lymphoblastic leukemia/lymphoma” by Hernandez-Ilizaliturri and Czuczman was recently published in Clinical Medicine: Therapeutics. 1 This review discusses the use of this purine analog in the treatment of patients with T-cell leukemia or lymphoma. The development of nelarabine was made possible through the efforts of many individuals who recognized its potential as a therapeutic agent. Here, a concise review of the development of nelarabine is presented in the positive context of collaboration between individual researchers, the pharmaceutical industry and government regulatory agencies.
Nelarabine (506U78; Arranon®; Atriance®) is the 6-methoxy derivative, pro-drug, of 9-β-D-arabinofuranosylguanine (ara-G). In vivo, nelarabine is efficiently demethoxylated by adenosine deaminase to form ara-G. The compound is indicated for the treatment of patients who have failed to respond to or have experienced relapse in the face of T-cell acute lymphoblastic leukemia or T-cell lymphoblastic lymphoma after receiving two or more chemotherapy regimens. 2
Development of Nelarabine
The development of Nelarabine was born out of the work of Gertrude Elion, who worked in the laboratory of Dr. George Hitchings at Burroughs Wellcome Company (now GlaxoSmithKline), in Tuckahoe New York, USA and later in Research Triangle Park North Carolina, USA. As Hitchings surmised that analogs of endogenous nucleosides could work to interrupt cell reproduction, he and Elion worked to make and test various nucleoside analogs. 3 By the early 1950's, Elion's research group had synthesized more than 100 purine analogs. 6-mercaptopurine (6-MP) was one of the early analogs found to be active in treating leukemia. 4 Over the years, its use in combination with other compounds for remission induction, consolidation and maintenance has resulted in a cure rate of childhood leukemia of approximately 80%.3,5 6-MP was a model compound which encouraged the search for other therapeutically active purine analogs.
In 1964 Reist and Goodman synthesized 9-β-D-arabinofuranosyl guanine (ara-G) and while over time in-vitro activity against leukemic T-cells was documented, its use in the clinic was confounded by inadequate solubility.6,7 The use of ara-G was predicated on the observation that patients with purine nucleoside phosphorylase (PNP) deficiency were observed to have severe T-cell lymphopenia while maintaining adequate B cell counts. 8 The T-cell deficiency was due to increased deoxyguanosine triphosphate as patients with PNP deficiency are unable to degrade deoxyguanosine. 8 These observations lead to further work at Burroughs Wellcome. In the mid 1970s, a new enzymatic synthesis of purine-D-arabinosylnucleosides was developed. 9 This approach set the stage for the synthesis of 506u78, nelarabine, a compound with ten times the solubility of ara-G. 10 As stated earlier, nelarabine was shown to be converted in man, via adenosine deaminase, to ara-G. It was now time for nelarabine to be evaluated in the clinical setting.
As needed before clinical development could ensue, further in vitro work and pre-clinical toxicology, pharmacology and pharmacokinetic studies were performed by the scientists at Wellcome's laboratories. With the sufficient work performed and documented, Drs. Joanne Kurtzberg and Beverly Mitchell submitted an investigator driven Investigational New Drug (IND) application proposing the initial (Phase I) study of nelarabine in patients with refractory hematologic malignancies. In April 1994, 30 years after the synthesis of ara-G, and more than 40 years after the work of Elion was initiated, nelarabine entered clinical studies. 11 The initial study was started at Duke University and at the University of North Carolina and was supported by Burroughs Wellcome. Later, the study was expanded to include patients at the Boston University Medical Center and at the M.D. Anderson Cancer Center in Houston. 11
In the mid 1990's Burroughs Wellcome was acquired by Glaxo Inc. and at this time the future of the development of nelarabine was in question. Work continued in the clinic and initial responses to the compound in the refractory patient population were encouraging. With this information and the guidance of Drs. Elion, Kurtzberg, Mitchell and others, GlaxoWellcome, the newly combined company, made the commitment to formally sponsor the development of nelarabine. This decision was based on a clear therapeutic need of the subset of leukemia patients with T-cell disease.
During this time, the Cancer Therapy Evaluation Program (CTEP) of the Division of Cancer Treatment and Diagnosis at the United States National Cancer Institute partnered with GlaxoWellcome to further support the clinical development and distribution of nelarabine. This collaboration continued through the merger of GlaxoWellcome and SmithKline Beecham to form GlaxoSmithKline in 2000. In December 2003 nelarabine was granted “Fast Track” status, which is given to compounds in development that have the potential to meet an unmet medical need for a serious or life-threatening condition. Further collaboration between investigators, GlaxoSmithKline, and CTEP led to further studies (phase II) which provided more information to the FDA and the European regulatory authorities and resulted in nelarabine being given Orphan Drug Status, as a product being developed for a rare disease affecting less than 200,000 people annually in the United States (August. 10, 2004). On June 16, 2005, the European Commission approved orphan drug designation for nelarabine. In October 2005, the Food and Drug Administration (FDA; USA) granted accelerated approval for nelarabine, with the trade name Arranon® (nelarabine injection) product being made available. Finally, Atriance® (nelarabine injection) was approved for marketing throughout the European Union on August 22, 2007.
Current Information
Clinical studies have documented nelarabine's activity in the setting of refractory T-cell leukemia/lymphoma, with complete remissions and partial remissions noted by a number of investigators.11–14 It appears that nelarabine is less active in non-T-cell disease and in indolent cutaneous T-cell and peripheral T-cell lymphoma. 1 However, Kurtzberg points out, varying dosing schedules need to be evaluated in these settings. 16
Neurotoxicity has been dose limiting in several studies with nelarabine.11–14 It has been speculated that ara-G reaches higher concentrations in neurons, however, the true mechanism of nelarabine neurotoxicity or other purine nucleoside analogs has not been delineated. 15
Many questions remain with respect to selecting nelarabine for use and identifying optimal dosing schedules. It is clear that nelarabine has an important role to play in the treatment of certain T-cell malignancies and collaboration with respect to the study of nelarabine continues. Table 1, below, lists the status of various studies investigating the compound to date.
Current active studies further investigating the use of nelarabine. a
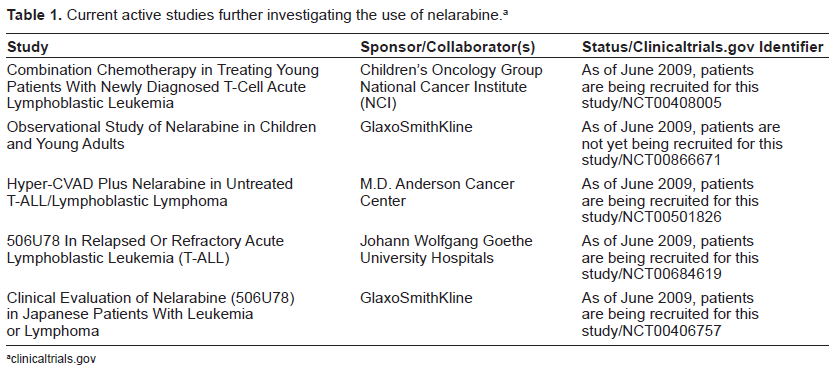
clinicaltrials.gov
Currently there have been more than 60 publications that describe various aspects of nelarabine, including preclinical and clinical studies and reviews of the individual compound, such as that found recently in Clinical Medicine: Therapeutics and reviews of the class of compounds known as purine antimetabolites. As further work on nelarabine continues, we will look to the literature to help us learn more about its potential.
Summary
Nelarabine represents the final compound developed that had the direct input of Dr. Elion. Her work was born out of a rational approach to drug development, which resulted in marketed therapeutic agents that have benefited untold numbers of individuals and saved countless lives. In early February 1999, this author received a note from Dr. Elion regarding her upcoming visit to Ohio Northern University (April 1999), where she was to present the annual Merck Lecture. She put forth the idea of discussing her role in drug discovery and development and thought she may discuss the purine analog story. Unfortunately Dr. Elion passed away later that February and our students did not get to hear this important story. Now, some ten years after her death, it is up to those who Dr. Elion has mentored and their colleagues to collaborate and continue writing the story of nelarabine, with the goal of identifying its optimal use.
This brief commentary/review is dedicated to Dr. Gertrude Elion on the tenth year anniversary of her passing. (January 23, 1918-February 21, 1999).
Disclosure
The author reports no conflicts of interest.