
Abstract
Pitavastatin is an HMG-CoA reductase inhibitor that significantly reduces the plasma levels of total cholesterol, LDL-C and triglycerides, while also causing modest elevation of the plasma high-density cholesterol (HDL-C) level. This statin is minimally metabolized by the cytochrome P-450 (CYP) isozymes; it is glucuronized and converted to the inactive lactone form, which is also minimally metabolized by human hepatic microsomes; therefore, it is associated with a low frequency of drug interactions. Pitavastatin has also been shown to have various pleiotropic effects on platelets, monocytes/macrophages and endothelial cells. In addition, a new effect of pitavastatin of increasing the serum for adiponectin level has been reported recently. Pitavastatin has been reported to be associated with a lower frequency of adverse drug effects such as hepatic dysfunction and rhabdomyolysis, therefore, it may be judged as one of the safer among the strong statins. Several clinical trials of pitavastatin have been conducted. At present, its evaluation in actual clinical use by clinicians around the world is underway. Pitavastatin is an effective and safe drug for patients with hypercholesterolemia.
Keywords
Introduction
Atherosclerosis is a chronic inflammatory disease that is associated with disordered lipid metabolism. 1 For example, high plasma levels of cholesterol have been clearly identified as a risk factor for atherosclerosis, and high plasma levels of low-density lipoprotein cholesterol (LDL) promote the development of atherosclerotic vascular disease. 2 Because modified LDL (e.g. by oxidation) is capable of loading macrophages with cholesterol, in contrast to unmodified LDL, 3 oxidized (ox)LDL is considered to be particularly atherogenic.
Large clinical trials of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors (statins) have shown that lowering of the plasma cholesterol by statins is associated with a decrease in the incidence of cardiovascular events and delay in the progression of atherosclerosis.4,5 Pitavastatin is an HMG-CoA reductase inhibitor that significantly reduces the plasma levels of total cholesterol, LDL-C and triglycerides, while causing modest elevation of the plasma high-density cholesterol (HDL-C).6–8 This statin has also been shown to have various pleiotropic effects on platelets, monocytes/macrophages and endothelial cells.9–12 Therefore, recent recommendations emphasize considerations of pitavastatin in hyperlipidemic patients with diabetes mellitus.13,14 In this review, I shall describe the pharmacological profile of pitavastatin, and recent evidence on both its efficacy and safety.
Pharmacology
Chemistry
Pitavastatin((+)-monocalciumbis(3R,5S,6E)-7-[2-cyclopropyl-4-(4-fluorophenyl)-3-quinolyl-3,5-dihydroxy-6-heptenoate]) (C50H46CaF2N2O8), is an entirely synthetic statin with a molecular weight of 880.98, that was initially developed by Nissan Chemical Industries Ltd., Tokyo, Japan, and later by Kowa Co. Ltd., Tokyo, (Fig. 1). 15 Pitavastatin exerts its potent pharmacological actions by strongly binding to the active sites on HMG-CoA reductase. Pitavastatin is thought to form 10 hydrogen bonds with hydrophilic amino groups in the active pocket of the enzyme. 16 It has been reported that the inhibitory activity on HMG CoA reductase of a pitavastatin analogue with, an isopropyl group instead of a cyclopropyl group, was only about one-fifth of that of pitavastatin, therefore, pitavastatin may be regarded as a compound designed to fit the enzyme structure. 17 Pitavastatin calcium is a white to pale yellowish odorless powder. It is freely soluble in pyridine and tetrahydrofuran, soluble in ethylene glycol, slightly soluble in methanol, very slightly soluble in ethanol (99.5) or water, and practically insoluble in acetonitrile or diethyl ether. 18 It dissolves well in dilute hydrochloric acid. The partition coefficient (n-octanol/phosphate buffer, pH 7.0) of pitavastatin is 31.7. 19
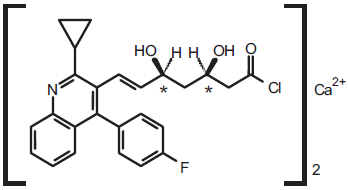
Structure of pitavastatin.
Pharmacodynamics and pleiotropic effects HMG-CoA reductase-inhibitory activity
Pitavastatin produces substrate-competitive type inhibition of HMG-CoA reductase with an IC50 of 6.8 nM, which indicates that the drug is 2.4- and 6.8-fold more potent than simvastatin and pravastatin, respectively. 20
Inhibition of cholesterol synthesis
Pitavastatin inhibited cholesterol synthesis from acetic acid with an IC50 of 5.8 nM in a human liver cancer cell line (HepG2), which indicates that is 2.9 and 5.7 times as potent as simvastatin and atorvastatin, respectively. 21 When the inhibitory activity interms of the ED50 was compared with that of simvastatin, pitavastatin showed a 3-fold stronger activity in the rat and 15-fold stronger activity in a guinea pig model. 22 The inhibitory effect of pitavastatin on sterol synthesis is thought to be liver-selective. 21
Enhancement of LDL-receptor expression
In in-vitro studies in HepG2 cells, pitavastatin increased the LDL-receptor mRNA expression 21 and the amount of LDL binding to the LDL-receptor, the amount of LDL internalization into the cells 23 and the amount of degradation of apoB. 24 As compared to simvastatin and atorvastatin, pitavastatin produced more potent induction of expression of the LDL receptor mRNA. 21
Pleiotropic effects
Various in-vitro and in-vivo studies have suggested that pitavastatin also has many pleiotropic effects; it reduces the inflammatory response 25 and generation of reactive oxygen species, 26 improves endothelial function, 27 increases nitric oxide production, 12 inhibits cell adhesion, 28 attenuates smooth muscle cell contraction, 29 increases thrombomodulin expression, 30 enhances angiogenesis, 31 promotes apolipoprotein (apo) A-I production, 32 and prevents the progression of aortic atherosclerosis. 33
Recently, a new effect of pitavastatin of increasing the serum adiponectin level has been reported.34–37 Hyperlipidemic patients with type 2 diabetes exhibited a significant increase of the serum adiponectin levels after pitavastatin treatment (before vs. 3 months, 6 months, 2.81 ± 0.95 vs. 3.36 ± 0.84 μg/ml; p < 0.01, 4.61 ± 1.15 μg/ml; p < 0.001) (Fig. 2). 35 Two possibilities for the mechanism underlying elevation of the serum adiponectin levels following pitavastatin treatment have been postulated. One is blockade of the production of reactive oxygen species (ROS) that cause hypoadiponectinemia,38,39 and another is the influence of sterol regulatory element binding proteins (SREBPs) that play an important role in adipocyte production and differentiation. 40 However, further examination is required to elucidate the mechanism underlying elevation of the serum adiponectin levels pitavastatin.
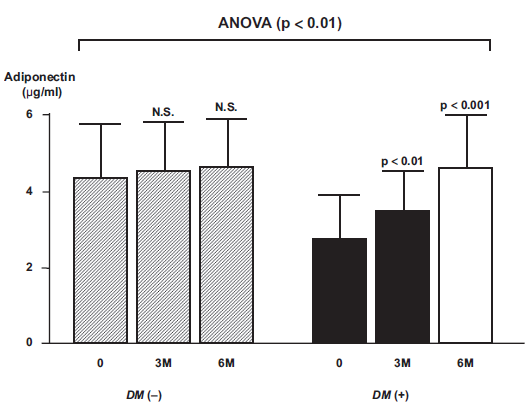
Changes in adiponectin levels before and after administration of pitavastatin to hyperlipidemic patients with and without type 2 diabetes. 35 DM (−), diabetes negative group; DM (+), diabetes positive group; 0, before; M, month (after).
Pharmacokinetics and metabolism
In pharmacokinetic studies, pitavastatin has been shown to have high bioavailability, exceeding 80% in rats, 41 and it is selectively distributed to its target organ, the liver. 42 Pitavastatin is minimally influenced by CYP metabolism in spite of its lipid solubility; it is glucuronized and rapidly converted through the elimination reaction to the inactive lactone form, which is also minimally metabolized by human hepatic microsomes.43,44 In addition, none of pitavastatin and its lactone form has major influence on CYP2C9- and CYP3A4-mediated metabolism of model substrates. 43 Thus, as compared with other statins which are mainly metabolized by CYP, pitavastatin has a unique metabolic pathway, so that the frequency of CYP-mediated drug interactions is minimized, which might contribute significantly to the clinical usefulness of pitavastatin. In an in-vitro study in human liver microsomes, the metabolic clearance rate of pitavastatin was 2.5 μL/min/mg, about 1/10th that of other statins, and inhibition of the metabolic reaction by itraconazole and grapefruit juice, which inhibits CYP3A4, was observed for atorvastatin, which is metabolized by CYP3A4, but not for pitavastatin. 44 It has been reported that the organic anion transporter 2 (OATP2/OATP1B1) plays a role in the incorporation of pitavastatin, like that of the other statins, into the liver, so that co-administration of cyclosporine is associated with a 4.6-fold increase of its blood concentration (AUC0-24) owing to inhibition of incorporation of the drug into the liver.46,47 Similarly, the blood concentrations of simvastatin, atorvastatin, rosuvastatin, lovastatin, and pravastatin were reported to increase 3 to 8-fold, 6 to 9-fold, 7-fold, 5 to 20-fold, and 5 to 12-fold. 48 However, P-glycoprotein, which shares its substrates with CYP3A4, is not involved in the pharmacokinetics of pitavastatin. 49
Clinical Studies
Phase I studies
The safety and pharmacokinetics of pitavastatin were evaluated in some studies conducted in healthy male subjects. 8 Based on the results, it was determined that pitavastatin doses of 1 mg, 2 mg and 4 mg were safe for further clinical evaluation in hyperlipidemia patients.
Phase II studies
The efficacy and safety of pitavastatin have been evaluated in three small studies of hyperlipidemic patients. 8 Pitavastatin was administered at 4 mg/day for 8 weeks in 34 hyperlipidemic patients. The results revealed a significant decrease of the serum LDL-C by 46% and of the serum TG by 42% (pre-administration TG level ≥ 150 mg/dL), and a statistically significant increase of the serum HDL-C by 4 mg/dL. Adverse drug reactions occurred in 10.0%. As compared with the levels in the placebo population, the serum TG levels decreased significantly (by 20%) in patients receiving pitavastatin in a doubleblind cross-over study.
To investigate the efficacy and safety as well as the dose response relationship, pitavastatin was administered at 1 mg, 2 mg or 4 mg once a day for 12 weeks by a double-blind method to 273 hyperlipidemic patients. 50 Significant decrease of the serum LDL-C by 34%, 42% and 47% was observed at the doses of 1 mg, 2 mg and 4 mg, respectively, indicating a dose-response relationship. A significant decrease of the serum TG and significant increase of the serum HDL-C were also observed at all doses (Fig. 3), although there was no dose-response correlation in the drug effect on these latter parameters. Pitavastatin at 2 and 4 mg doses appeared to be as efficacious as 10 and 20 mg atorvastatin. Based on the these results, pitavastatin was judged to be effective for the treatment of hyperlipidemia at the recommended dose of 2 mg or 4 mg.
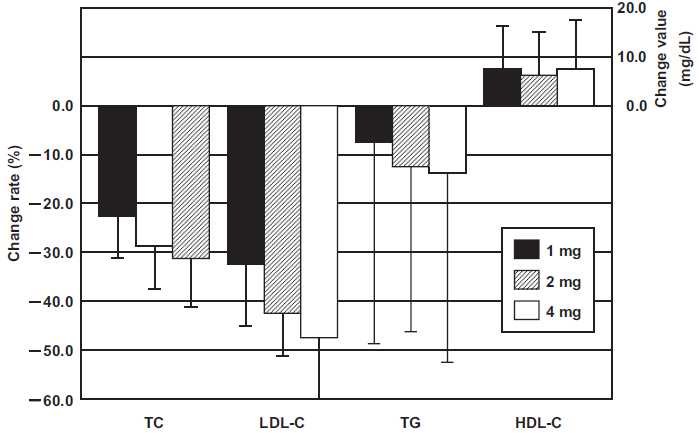
Mean percent changes (TC, LDL-C and TG) and mean changes (HDL-C) from baseline values after 12 week with various doses of pitavastatin in Japanese patients with hyperlipidemia. 50
Phase III studies
Comparative study with pravastatin
The percent reductions of the serum LDL-C by pitavastatin 2 mg/kg/day and pravastatin 10 mg/kg/day were 38% and 18% respectively, indicating a significant difference between the effects of the two drugs. 51 The percent reductions of the serum TG by pitavastatin and pravastatin were 23% and 20% respectively, and signicant elevation of the serum HDL-C of 4 mg/dL and 5 mg/dL, respectively, was also noted. About 124 patients in the pitavastatin group and 109 patients in the pravastatin group were included in the safety analysis. There were no serious adverse events, and most of the events were mild to moderate clinical laboratory abnormalities. These results suggest that serum LDL reduction by pitavastatin is more pronounced than that by pravastatin at comparable doses, and that there is no substantial difference in the safety between the two drugs.
Study in patients with familial hypercholesterolemia
The clinical efficacy of pitavastatin 2-4 mg/day was assessed in 30 patients with heterozygous familial hypercholesterolemia (FH). 52 At 2 mg/day, significant reduction of the serum LDL-C by 40% was observed, which increased further to 48% following the drug administration at 4 mg/day. There were no adverse events. 6 The percent reduction of the serum LDL-C level in patients with FH was compared among the statins that are currently available in Japan. 53 The results provided a new therapeutic choice for the treatment of patients with heterozygous FH.
Study in patients with type 2 diabetes
To investigate the influence of pitavastatin on glucose metabolism and the safety of the drug in patients with type 2 diabetes, pitavastatin was administered to 34 patients with type II diabetes mellitus associated hyperlipidemia at the dose of 2 mg/day for 8 weeks in a phase III study. 54 No significant changes were noted in the fasting blood glucose, suggesting that the influence of pitavastatin on the glycemic status was negligible. The efficacy was similar to that observed in phase II and comparable phase III studies. In addition, improvement of the serum levels of remnant-like lipoprotein and small dense LDL was also suggested.
Enhancement of serum HDL-C
Pitavastatin appears to increase the serum levels of functional HDL-C through increasing the levels of apo A1. It has also been reported that pitavastatin increased the serum HDL-C by 22.5% in a group with low baseline HDL-C (<40 mg/dL) levels. 55 Increase of the serum HDL-C by pitavastatin is very important clinically, because low serum levels of HDL-C are major risk factor for coronary heart disease. 56
A clinical study by Yokote et al 57 yielded interesting and suggestive results. They conducted a 12-week, prospective, open-label trial to compare the efficacy and safety of pitavastatin 2 mg/day versus atorvastatin 10 mg/day in 204 hypercholesterolemic patients. Both pitavastatin and atrovastatin significantly reduced the serum LDL-C by 42.6% and 44.1%, and serum TG by 17.3% and 10.7%, respectively, after 12 weeks’ treatment with no significant intergroup differences (Fig. 4). Significant increase of the serum HDL-C was observed after 12 weeks of pitavastatin treatment (3.2%, p = 0.033 vs. baseline), but not after 12 weeks of atorvastatin treatment (1.7%, p = 0.221 vs. baseline) (Fig. 4). The waist circumference, body weight and BMI were significantly correlated with the percent reduction of the serum non-HDL-C in the atorvastatin group, whereas consistent reduction of the serum non-HDL-C was observed in the pitavastatin group, regardless of the body size.
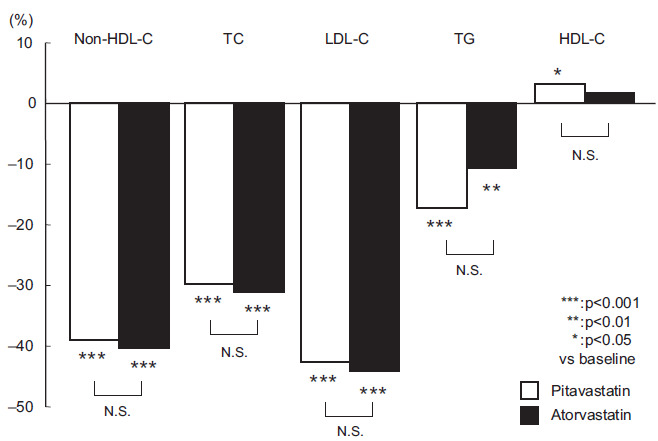
Percent change from baseline in lipid levels in all patients. Data are presented as mean ± S.D; PTv, pitavastatin (n = 93); ATv, atorvastatin (n = 98).
Another study conducted on patients with hypercholesterolemia who were under treatment with atorvastatin has been reported. Patients were divided into groups who continued to receive atorvastatin or were switched to pitavastatin. 58 After 3 months, no significant difference of the serum HDL-C was observed in the group continued on atorvastatin, while significant increase of the serum HDL-C as compared with the baseline level was observed in the group switched to pitavastatin. Thus, pitavastatin may have a more pronounced effect on the serum HDL-C.
Comparative study with simvastatin in Korea
An 8-week, multicenter, prospective, randomized, open-label, clinical trial was conducted, to compare the efficacy and safety of pitavastatin 2 mg/day versus simvastatin 20 mg/day in Korean patients with hypercholesterolemia. 59
The percent change of the serum LDL-C was −38.2% in the pitavastatin group and −39.4% in the simvastatin group, with no significant difference between the two groups. The percent change of the serum TG among patients with baseline TG values higher than 150 mg/dL was −29.8% in the pitavastatin group and −17.4%, in the simvastatin group. The percent change of the serum HDL-C was 8.3% and 3.6% in the pitavastatin and simvastatin groups, respectively, with no significant difference between the two groups.
Adverse reactions occurred in 15.4% of the patients in the pitavastatin group and 37.3% of the patients in the simvastatin group, the difference between the two groups being significant. Serious adverse reactions were not noted in either group.
Comparative study with atorvastatin in India, Denmark, Russia and Spainsimvastatin in Korea
A 12-week, multicenter, prospective, randomized, double-blind clinical trial was carried out to compare the efficacy and safety of pitavastatin 2 to 4 mg/day and atorvastatin 10 to 20 mg/day in patients with hypercholesterolemia or combined dyslipidemia in India, Denmark, Russia, and Spain. 60
Pitavastatin 2 to 4 mg/day demonstrated the percent change of the serum LDL-C by −37.9% and −44.6%, respectively, which was comparable to that of atorvastatin 10 to 20 mg/day by −37.8% and −43.5%, respectively. In any other lipid parameters no statistically significant differences were observed.
Safety and Tolerability
Clinical trials
Pitavastatin at doses of 1, 2 and 4 mg has been well-tolerated, with a safety profile comparable to that of other statins. The results of 8 clinical trials in Japan are summarized below. 8 Subjective symptoms and objective findings assessed as adverse drug reactions were noted in 5.6% (50/886 subjects), but none of the events individually occurred at a rate higher than 1%. Abnormal laboratory parameters assessed as adverse drug reactions by the attending physician were noted in 18.8% of the subjects (167/886 subjects). The major changes were increased serum γ-GTP in 5.3%, increased serum CK in 4.6%, increased serum GPT in 3.6%, and increased serum GOT in 3.2% of the cases. These adverse reactions were similar to those observed to the statins already available in the market. Severe adverse drug reactions occurred in 0.9%, and the administration needed to be discontinued on account of adverse drug reactions in only 2.8% of the patients.
Post-marketing surveillance
A large-scale, long-term, prospective post-marketing surveillance study of pitavastatin, the Livalo Effectiveness and Safety (LIVES) Study, was conducted to evaluate the safety and efficacy of pitavastatin in the clinical setting in Japan. 61 Of the 20,279 patients recruited, 19,925 patients were included in the analysis of drug safety, and 18,031 patients were included in the efficacy evaluation. Adverse drug reaction were observed in 2,069 of the 19,925 patients (10.4%), and most of the adverse drug reactions were classified as mild. Common adverse drug reactions were blood CPK increased (2.74%), ALT increased (1.79%), AST increased (1.50%), myalgia (1.08%) and γ-GTP increased (1.00%).
Treatment with this drug resulted in a significant reduction of the serum LDL-C (29.1%). The peak serum lipid level reduction occurred within 4 weeks of treatment initiation, and then plateaued. In patients with abnormal baseline levels of serum TG and serum HDL-C, pitavastatin decreased the serum TG (22.7%), and increased the serum HDL-C (19.9%) as compared with the values at baseline (Fig. 5). Based on the criteria established by the Japan Atherosclerosis Society (JAS) guideline for the diagnosis and prevention of atherosclerotic cardiovascular diseases for Japanese, goal serum LDL-C levels were achieved in 88.2% of the primary prevention, low-risk patients, 82.7% of the primary prevention intermediate-risk patients, 66.5% of the primary prevention high-risk patients and 50.3% of the secondary prevention patients. No significant safety or efficacy issues were observed.
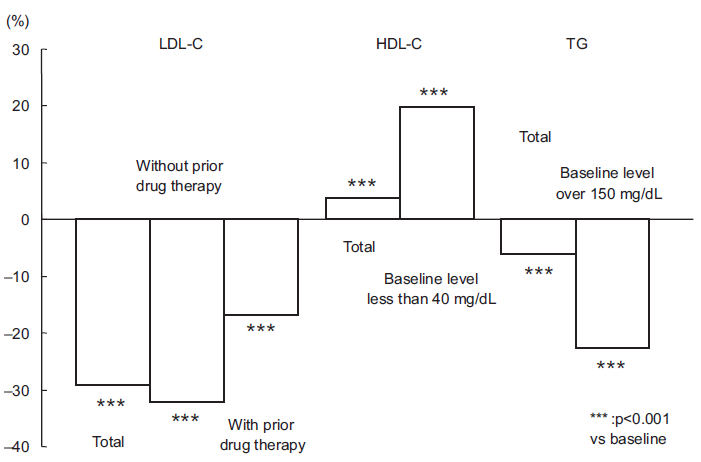
Time-course of changes in the serum LDL-C, HDL-C and TG.
Drug-drug interactions with co-administered drugs
In general, patients requiring statin therapy frequently have concomitant diseases such as hypertension, diabetes mellitus and/or coronary artery disease. In the treatment of such patients, multiple drugs frequently need to be co-administered with the statins, which gives rise to the possiblility of drug interactions and elevation of the blood concentrations of the concomitantly administered drugs or the statin, and consequently, a higher risk of higher of adverse drug reactions. However, pitavastatin is minimally metabolized by CYP isozymes, and therefore associated with a minimal incidence of drug interactions. In the LIVES study, the incidence of adverse reactions for each concomitantly administered medication was studied, and no increase in the incidence of adverse reactions was observed with any of the concomitantly administered drugs. These data support the absence of any clinically significant drug interactions with pitavastatin.
Musculoskeletal adverse events
The rate of muscle related adverse events associated with pitavastatin is lower than that with other statins. For example, atorvastatin was found to be associated with a higher risk of musculoskeletal adverse events, including elevation of the serum CK, as compared with pitavastatin in routine clinical practice in Japan (atorvastatin 144/4805, pitavastatin 154/7930; risk ratio 1.54, confidence interval 1.23 to 1.93; P = 0.0001 by the Mann-Whitney U test), 58 and in the comparative study with simvastatin conducted in Korea, 59 greater than 2-fold elevations over the upper limit of normal of the serum CK were observed in 3.8% (2/52) of pitavastatin-treated patients and 9.8% (5/51) of simvastatin-treated patients, although the difference between the two groups was not ststistically significantre.
Glycemic control
Absence of influence of pitavastatin on the glycemic status in diabetic subjects has been reported by numerous clinical trials, and the incidence of increased plasma glucose and HbA1c as adverse reactions were only 0.01% and 0.02% respectively. 8 Glucose uptake by differentiated 3T3-L1 cells was reported to be unaffected by pitavastatin, but to be reduced by other statins. 63 In one study, pitavastatin did not affect glycemic control in 78 patients with type 2 diabetes. 64 Sasaki et al 13 compared the effects of pitavastatin and atorvastatin on the serum HDL-C and other lipids and also on the glucose metabolism in Japanese patients with elevated serum LDL-C levels and glucose intolerance. Two hundred seven patients were enrolled in the study, and 173 patients (88 pitavastatin, 85 atorvastatin) were included in the efficacy evaluation (Fig. 6). The primary endpoint of percent change in the serum HDL-C levels was significantly greater in the pitavastatin group than in the atorvastatin group (8.2 vs. 2.9, respectively; p = 0.031), as was the percent change in the serum levels of apolipoprotein A-I (5.1 vs. 0.6; p = 0.019). Similarly, 52 weeks of treatment with pitavastatin 2 mg/day was associated with significantly greater increases of the serum HDL-C and apolipoprotein A-I levels than atorvastatin 10 mg/day during the study period. There were no significant differences between the treatment groups with respect to the parameters of glucose metabolism.
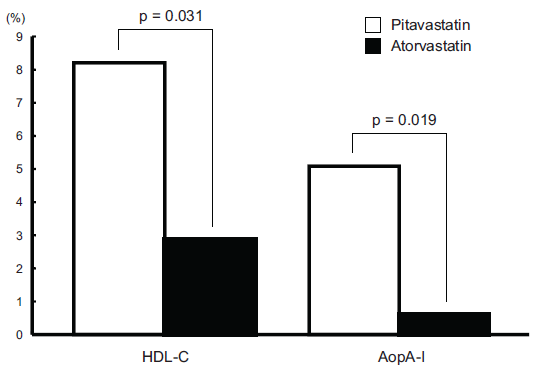
Percent change in lipid measures after 12 months of treatment.*
On the other hand, Yokote et al 57 demonstrated an increase of the serum level of glycoalbumin in diabetic patients receiving atorvastatin, but not in those receiving pitavastatin; also, in patients with the metabolic syndrome, pitavastatin was more effective than atorvastatin in lowering the serum LDL-C. Taken together, the results suggest that pitavastatin is useful for lowering the serum LDL-C in patients with diabetes mellitus or the metabolic syndrome.
Patient-Focused Perspectives
The Japan Assessment of Pitavastatin and Atorvastatin in Acute Coronary Syndrome (JAPAN-ACS) study was a prospective, randomized open-label parallel group study with blind endopoint evaluation conducted with the participation of 33 centers in Japan.65,66 A total of 307 patients with ACS undergoing IVUS-guided percutaeous coronary intervention were randomized and 252 patients had evaluable IVUS examinations at baseline as well as at the 8-12 months’ follow-up. The study was conducted to compare the effect of pitavastatin 4 mg/day and atorvastatin 20 mg/day on the coronary plaque volume (PV) in patients with acute coronary syndrome using IVUS imaging. The mean percentage change of the PV was −16.9% ± 13.9% and −18.1% ± 14.2% (p = 0.5) in the pitavastatin and atorvastatin group, respectively, which was associated with negative vessel remodeling. The upper limit of the 95% confidence interval (CI) of the mean difference in the percent change of the PV between the two groups (1.11%, 95% CI: −2.27 to 4.48) did not exceed the pre-defined non-inferiority margin of 5%. This study emphasizes the significance of intensive lipid-lowering therapy in patients with ACS in Japan.
Furthermore, two large clinical trials, namely, the Japan Prevention Trial of Diabetes by Pitavastatin in Patients With Impaired Glucose Tolerance (J-PREDICT) and the pitavastatin heart failure study (PEARL Study) are on-going. The results are being expected with great anticipation.
Place in Therapy
The benefit of aggressive lipid-lowering therapy in high-risk patients has been established. However, it has been hypothesized that strong inhibition of cholesterol synthesis by statins may increase the risk of serious adverse reactions such as hepatic dysfunction and rhabdomyolysis. Thus, statins are required to not only show potent LDL-C lowering activity, but also to exhibit a high degree of safety.
Pitavastatin has been shown to potently reduce the serum LDL-C and serum TG, and also increase the serum HDL-C. The finding that pitavastatin induced the expression of the LDL receptor more strongly than other statins suggested that pitavastatin may have high safety as compared with that of the other statins, although there are few clinical trials comparing pitavastatin with other statins. The data also suggest that pitavastatin may be associated with a reduced incidence of drug interactions, since it is minimally metabolized by the CYP enzymes. The efficacy and safety of pitavastatin are supported by clinical trials and the LIVES study, a large-scale prospective postmarketing surveillance study, and pitavastatin represents a new therapeutic drug for preventing CHD in high-risk patients.
Many recent and ongoing pitavastatin trials are expected to clarify the anti-atherosclerotic and favorable pleiotropic effects of pitavastatin in patients at high risk for CHD.
Conclusion
Pitavastatin is a novel fully synthetic 3-hydroxy-3-methyl-glutaryl coenzyme A (HMG-CoA) reductase inhibitor. This drug exerts its potent pharmacological actions by strongly binding to the active sites on HMG-CoA reductase, and is one of the more potent statins along with atorvastatin and rosuvastatin. One unique characteristic of this statin is that it is minimally metabolized by the CYP isozymes, and is therefore associated with a reduced incidence of any drug interactions. Pitavastatin has been reported to be associated with a lower frequency of adverse effects such as hepatic dysfunction and rhabdomyolysis, and therefore may be judged as one of the safer drugs among strong statins. It is expected that drug-drug interactions, which is another factor related to safety, may be avoided with the use of pitavastatin, which is not metabolized by the cytochrome P-450 class of enzymes.67,68 Finally, pitavastatin may be an effective agent for the treatment of metabolic syndrome, because of its clearly beneficial effect on the serum HDL-C level. Various in-vitro and in-vivo studies have suggested that pitavastatin also has many pleiotropic effects.12,25–37,69 Several clinical trials of pitavastatin have been conducted. At present, its evaluation in actual clinical use by the clinicians around the world is ongoing. Differences in the efficacy and safety of various drugs among races (Oriental, Anglo-Saxon, Black etc.) are well known. Especially, the difference in the BMI between the Western and Orientals populations is significant. Therefore, it is possible that the beneficial effect of pitavastatin, as compared with other strong statins, on the glucose metabolism, observed in the Japanese study, might be masked in western countries.
Conflict of Interests
The author has no conflict of interests to report.
Footnotes
Acknowledgements
This review article on pitavastatin was invited by the Editor-in-Chief of Clinical Medicine: Therapeutics.