
Abstract
Objective
To evaluate the association between dyslipidaemia and Alzheimer’s disease (AD) in a cohort of postmenopausal women.
Methods
This retrospective study analysed data from postmenopausal women with early AD (group AD) and a cohort of healthy age- and sex-matched control subjects (group NC) that were considered to be within standard limits according to a neuropsychological assessment between March 2010 and March 2019. The primary endpoints were body mass index and lipid-related laboratory parameters, including leptin, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol, adiponectin, triglycerides, apolipoprotein A1, apolipoprotein B and apolipoprotein E4, which were evaluated using multivariate binary logistic analysis.
Results
The study enrolled 200 postmenopausal women with early AD (mean ± SD age 69.34 ± 6.25 years) and 180 control subjects (mean ± SD age 67.48 ± 7.42 years). Lower HDL-C and higher LDL-C were risk factors for AD. A multivariate binary logistic regression model demonstrated that lower HDL-C and higher LDL-C were the only variables associated with the development of AD (odds ratio [OR] 21.14, 95% confidence interval [CI] 2.47, 4.13; OR 36.35, 95% CI 1.24, 3.38; respectively).
Conclusion
Both low HDL-C and high LDL-C were associated with the occurrence of AD in a cohort of postmenopausal women.
Keywords
Introduction
There is increasing evidence that dyslipidaemia is a prominent contributing factor in Alzheimer’s disease (AD) pathogenesis, with it negatively regulating cerebral haemodynamics to induce a cascade of cellular and molecular upregulation that leads to cognitive deficits and ultimate progression of AD.1–3 AD has been increasingly recognized as a universal metabolic disorder, but strong evidence has not emerged to confirm this theory. 4 Research has demonstrated that a high body mass index (BMI) in postmenopausal women is a risk factor for advanced progression of AD.5,6 Furthermore, postmenopausal women with AD had a low BMI 3 years before the onset of AD-related symptoms, suggesting an association between dyslipidaemia and AD, 7 although a previous report implies a relationship between cerebrovascular changes and dyslipidaemia. 8
Dyslipidaemia mediated by the adipocyte may act to restrain energy expenditure. 9 Correspondingly, dyslipidaemia also interferes with the modulation of energetic metabolism.6,7 Extreme fat accumulation caused by dyslipidaemia leads to increased levels of leptin and aggregate effects of vascular risk factors on cerebrovascular changes. 7 Previous reports have demonstrated that the fat accumulation increases the risk of AD, as well as being associated with a quick progression of AD and with cardiocerebrovascular diseases,10,11 while depression has recently been associated with fat accumulation and low oestrogen. 12
Whether or not dyslipidaemia has an effect on AD was unclear in a cohort of postmenopausal women. 13 Even less was demonstrated for the role of low oestrogen in the occurrence of AD. 14 As a consequence, there is a crucial need to expand our knowledge of this issue given the wide-ranging deviation in the rate of cognitive decline in AD. To address these limitations and explore the relationship between dyslipidaemia and AD, this retrospective study analysed the association between dyslipidaemia and AD in a cohort of postmenopausal women.
Patients and methods
Study population
This retrospective study analysed data collected from consecutive postmenopausal women with early AD from the Department of Neurology, Affiliated Hospital of Hebei University, Baoding, Hebei Province, China between March 2010 and March 2019. Eligibility was restricted to those aged ≥60 years at diagnosis, but aged <85 years, because elderly patients with AD aged ≥85 years may be lost to follow-up as a result of short life expectancy and potential comorbidities. The diagnosis of AD was based on the recommendations of the National Institute on Aging and the Alzheimer’s Association workgroup.1,3,15 Patients with AD were studied at an early stage of the disease based on the Clinical Dementia Rating global scores.1 Only patients meeting the diagnostic criteria for early AD were included in group AD. For the control group NC, healthy adults aged ≥18 years were recruited from the Physical Examination Centre, The Affiliated Hospital of Hebei University. The healthy controls were age- and sex-matched to the patients in group AD. The main exclusion criteria for group AD included imperfect clinical data, traumatic brain injury, vascular dementia, psychiatric disorder, cancer, loss of ability to follow instructions, active infection, anticholinergic use, drug or alcohol abuse.
The study was approved by the Institutional Review Board of the Affiliated Hospital of Hebei University, Baoding, Hebei Province, China (no. 171120). Informed consent was not required due to the retrospective nature of the study.
Study endpoints
The primary endpoints were laboratory values collected including serum leptin, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), adiponectin, triglycerides (TG), apolipoprotein A1 (Apo-A1), apolipoprotein B (Apo-B) and apolipoprotein E4 (Apo-E4). Measurements of serum lipid concentrations were analysed using routine automated techniques (Covance, Indianapolis, IN, USA) at the Central Laboratory of The Affiliated Hospital of Hebei University. The severity of AD was assessed using the Mini-Mental Status Exam. 16 Dyslipidaemia was defined according to the 2004 update of the National Cholesterol Education Program guidelines: LDL-C ≥8.9 mmol/l, HDL-C ≤2.2 mmol/l, TG ≥8.3 mmol/l (at least one abnormal value), or patients that were on long-term lipid-lowering medication. 17
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). Data are presented as mean ± SD or n of patients (%). Categorical data were assessed using Mann–Whitney U-test or χ2-test as appropriate. Non-parametric analyses were performed for serum leptin, HDL-C, TC, TG and adiponectin. Normality analysis of the two-group variables was also performed. Between-group comparisons of continuous variables were undertaken using the non-parametric Mann–Whitney U-test. Multivariate binary logistic analysis was carried out to further clarify which variables were better at predicting disease status. Given that TC consists of HDL-C, LDL-C and TG, its value was not considered as a factor. Missing data were not included in the study. A two-sided P-value of < 0.05 was considered statistically significant.
Results
This retrospective analysis identified 267 consecutive postmenopausal women with early AD. Based on the inclusion and exclusion criteria, a total of 67 women were excluded and 200 women formed group AD for these analyses (Figure 1). The control group (group NC) consisted of 180 healthy individuals that were considered to be within standard limits according to the neuropsychological assessment. The mean ± SD age of group AD was 69.34 ± 6.25 years (range, 63–75 years) and for group NC was 67.48 ± 7.42 years (range, 60–74 years) (P = 0.021). Baseline demographic and clinical data for the two groups are shown in Table 1.

Flow diagram demonstrating the identification, exclusion and recruitment of a cohort of postmenopausal women with early Alzheimer’s disease (AD) in a study that aimed to evaluate the association between dyslipidaemia and AD. Group NC, healthy control subjects.
Baseline clinical and demographic characteristics of a cohort of postmenopausal women with early Alzheimer’s disease (group AD) and healthy control subjects (group NC) that were enrolled in a study to evaluate the association between dyslipidaemia and AD.

Data presented as mean ± SD or n of patients (%).
aCategorical data were assessed using Mann–Whitney U-test or χ2-test as appropriate. Non-parametric analyses were performed for serum leptin, HDL-C, TC, TG and adiponectin. Between-group comparisons of continuous variables were undertaken using the non-parametric Mann–Whitney U-test.
BMI, body mass index; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglycerides; Apo-A1, apolipoprotein A1; Apo-B, apolipoprotein B; Apo-E4, apolipoprotein E4; NS, no significant between-group difference (P ≥ 0.05).
The potential predictive factors for AD (group AD versus group NC) according to logistic regression models are presented in Table 2. Age and education were included because they are acknowledged to be independent predictive factors for AD. BMI, TG, Apo-A1, Apo-B, Apo-E4 carrier and Apo-E genotype were not predictors of AD. There was no association between leptin or adiponectin and AD. A multivariate binary logistic regression model demonstrated that lower HDL-C and higher LDL-C were the only variables associated with the development of AD (odds ratio [OR] 21.14, 95% confidence interval [CI] 2.47, 4.13, P < 0.001; OR 36.35, 95% CI 1.24, 3.38, P < 0.001; respectively).
Multivariate binary logistic analysis of the factors associated with Alzheimer’s disease (AD) in a cohort of postmenopausal women with early AD.
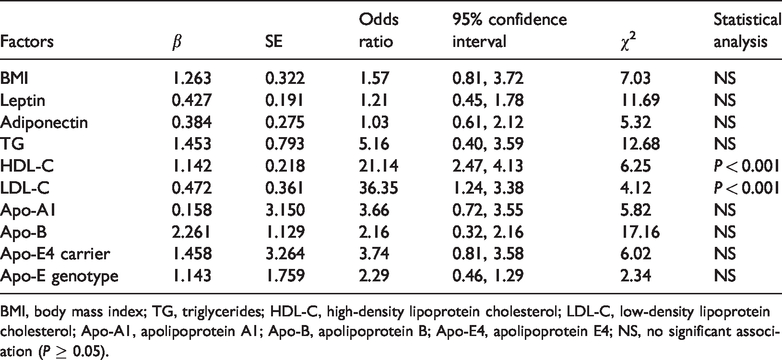
BMI, body mass index; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; Apo-A1, apolipoprotein A1; Apo-B, apolipoprotein B; Apo-E4, apolipoprotein E4; NS, no significant association (P ≥ 0.05).
Discussion
This current retrospective analysis provides evidence that both low HDL-C and high LDL-C are associated with the occurrence of AD in a cohort of postmenopausal women. To the best of our knowledge, this is the largest retrospective study that has investigated the association between dyslipidaemia and AD in a cohort of postmenopausal women.
A growing but still extremely limited body of literature has evaluated the role of dyslipidaemia in AD. For example, a previous study showed that hydroxy methylglutaryl coenzyme A reductase inhibitor significantly reduced the mortality of elderly women with AD. 18 To date, the available reports on the association between dyslipidaemia and AD in a cohort of postmenopausal women remain limited. A previous review described the role of diabetes mellitus in AD and revealed that diabetes and obesity are among the modifiable risk factors for AD, and hyperlipidaemia mediated by chronic hyperglycaemia provides a critical link between dyslipidaemia and AD. 11 Widespread attention has been focused on whether dyslipidaemia has a positive correlation with sex in AD. For example, a previous study reported a positive correlation between dyslipidaemia and AD in a cohort of elderly female patients. 19 Other research has demonstrated that low HDL-C and high LDL-C appeared to result in the development of AD and that the onset of the disease was significantly correlated with time and degree of dyslipidaemia.20,21
Postmenopausal women with AD are recognized as having low BMIs during illness. 22 Given leptin is produced in proportion to fat, the levels of leptin tend to be associated with BMI.5,11 This dependence on BMI could explain the lack of a role for leptin in the current regression model. 10 Leptin resistance is recognized to increase with BMI and factors that regulate resistance increase with age, which could contribute to the studied results.3,20 Although the role of adiponectin in cognitive decline is currently debated, 13 an inverse relationship between adiponectin and BMI has been demonstrated previously. 19
Along with reports related to cholesterol metabolism, higher HDL-C seems to be an indication of a lower incidence of AD, while high LDL-C appears to be a risk factor.21,23 In addition, patients with AD frequently suffer from higher levels of TC, but not TG.11,20 After controlling for other baseline variables, LDL-C was shown to be a risk factor for AD in postmenopausal women in this current study, which could result in discussions about risk variables for AD.2,21 Specifically, statins could be suitable for women and there is interest in the use of niacin to increase HDL-C.11,17
In the current study, BMI was significantly lower in the patients with AD by over 2 kg/m2 compared with the healthy control subjects. BMI appears to be a predictor of AD in postmenopausal women. 24 Although it has been reported that central obesity in female populations can predict AD,6,24 the data reflecting BMI was incomplete in this study, which may simulate the low BMI after the onset of AD to a certain extent. 21 Supplementary lipid regulators may activate dormant genes associated with AD. 22 LDL receptors contribute to amyloid-β protein precursor catabolism and amyloid-β cell transport at the gene level.21,25
This current study had a number of limitations that need to be considered. The retrospective nature of the study and the exclusion criteria used for the study participants may have limited the conclusions. In addition, the timing of the lipid test was not fixed for a certain period of time, which may lead to differences in the test values. Furthermore, there were no uniform diagnostic criteria for potential comorbidities in the patients participating in the study. Coupled with the patient’s personal habits, such as smoking and drinking, this information was obtained verbally from the patient, which may have resulted in bias. The findings of this current study are not generalizable as the study was restricted to postmenopausal women. In addition, although the study followed the general guidelines, the blood lipid results may have been constrained by the examination equipment, because the patients were from two different wards in the hospital. Although the examination equipment was the same, there were differences in personnel between the two wards.
In conclusion, the results reported in this current study supplement a growing body of evidence that suggests that both low HDL-C and high LDL-C are associated with the occurrence of AD in postmenopausal women. Although a number of issues remain to be addressed, these findings provide a starting point for clarifying the risk factors for AD, which in turn could help with the early detection of AD, strategies to prevent or delay AD in the early stages before the onset of dementia and mortality reductions in the later stages of the disease. Prospective studies are needed to determine whether these risk factors can serve as an early warning of AD.