
Abstract
In recent years considerable insight has been gained in the optimal management of adult asthma. In asthma patients who have persistent symptoms despite the daily use of (a low dose) inhaled corticosteroids (ICS), adding a long-acting β2-agonist to ICS improves asthma control and decreases the number of exacerbations. Currently two different LABAs are available, ie formoterol and salmeterol. The most important difference between both LABAs is a more rapid onset of action of formoterol (2-5 minutes) when compared to salmeterol (15-30 minutes). Partly based on these pharmacological differences, two major different approaches have been put forward to asthma management. The first approach (Gaining Optimal Asthma Control) is promoted by the producers of fluticasone/salmeterol and recommends to step up ICS to the dose needed to achieve optimal asthma control in order to keep the patient symptom free and to prevent exacerbations. The second approach is promoted by the producers of budesonide/formoterol and recommends a low maintenance dose which can be adjusted up or down according to the clinical control of asthma. Initially, a treatment strategy with Adjustable Maintenance Dosing with budesonide/formoterol was introduced. At a later time, this concept was changed to the Symbicort Maintenance And Reliever Therapy (SMART) approach. The aim of this manuscript is to review the current literature on the management of asthma with ICS and LABAs and to discuss the different treatment strategies.
Introduction
Asthma is a disease characterized by airway inflammation and recurrent episodes of symptoms of wheezing and chest tightness that are associated with variable airway obstruction and bronchial hyperresponsiveness. Asthma affects 300 million people worldwide and its prevalence is still increasing. 1 International guidelines stipulate goals for optimizing asthma treatment such as preventing acute and chronic symptoms, minimizing exacerbations and emergency care, and maintaining a normal level of physical activity. Inhaled corticosteroids are the cornerstone of asthma treatment, since they suppress virtually every step of the inflammatory cascade in asthma. However, some patients with asthma require high doses of inhaled corticosteroids (ICS) to achieve an acceptable level of disease control and this may lead to both local side effects like oral candidiasis, hoarseness and skin bruising, and systemic side effects, ie suppression of the hypothalamic-pituitary-adrenal axis, osteoporosis, and (in children) growth retardation.2–4 For this reason sustained release theophylline and leukotriene modifiers have been combined with ICS as an alternative to an increase in ICS doses alone. It has been shown that both the addition of oral theophylline and the antileukotrienes montelukast and zafirlukast in patients with asthma may improve symptoms and lung function and decrease the number of exacerbations.5–8 An alternative to these additional therapies are long-acting β2-agonists (LABA). Addition of a LABA to maintenance treatment with ICS improves asthma control. 9 Importantly, the beneficial effects provided by adding a LABA to ICS are much larger than the additive effects of theophylline and antileukotrienes.10–12 Currently, two different LABAs are available, ie formoterol and salmeterol. The most important difference between both LABAs is a more rapid onset of action of formoterol (2-5 minutes) when compared to salmeterol (15-30 minutes). 13 Partially based on these pharmacological differences, two different major approaches have been put forward to asthma management. The first approach (Gaining Optimal Asthma Control) is promoted by the producers of fluticasone/salmeterol and recommends to step up ICS to the dose needed to achieve optimal asthma control in order to keep the patient symptom free and to prevent exacerbations. The second approach is promoted by the producers of budesonide/formoterol and recommends a low maintenance dose which can be adjusted up or down according to the clinical control of asthma. Initially, a treatment strategy with Adjustable Maintenance Dosing with budesonide/formoterol was introduced. At a later time, this concept was changed to the Symbicort Maintenance And Reliever Therapy (SMART). With the SMART approach, patients use a maintenance dose of budesonide/formoterol 160/4.5 μg b.i.d. or 320/9 μg b.i.d. in a single inhaler. In addition, they are allowed to use budesonide/formoterol 160/4.5 μg as needed with a maximum of extra 10 as-needed inhalations per day. The most important difference with adjustable maintenance dosing is that patients use a single inhaler with SMART (instead of one inhaler with budesonide/formoterol and a separate inhaler containing reliever medication). In addition, patients are able to more rapidly adjust their treatment up and down according to their symptoms. The aim of this manuscript is to review the current literature on the management of asthma with ICS and LABA's and to discuss the different treatment strategies.
Anti-inflammatory Effects of β2-agonists
β2-agonists not only cause bronchodilation, but also exert anti-inflammatory effects as has been shown in many in vitro studies. These effects include inhibition of the oxidative burst and release of thromboxane and leukotriene C4 from eosinophils.14–16 and inhibition of mediator release from circulating neutrophils, although relatively high concentrations are required.17,18 Furthermore, β2-agonists inhibit the release of Th2 type cytokines such as IL-5 from peripheral blood lymphocytes and the release of GM-CSF from cultured human lung fibroblasts.19,20 Finally, it has been demonstrated that the inhaled β2-agonists albuterol, terbutaline, and formoterol, when given as single dose, provide greater bronchoprotection against AMP-induced bronchoconstriction than against methacholine or histamine-induced bronchoconstriction, and this differential bronchoprotective effect has been interpreted as mast cell stabilization.21,22 In agreement with this, it has been demonstrated that β2-agonists inhibit the release of histamine from chopped human lung and dispersed human lung mast cells.23,24
Despite the abovementioned anti-inflammatory effects of β2-receptor agonists in in vitro studies, no beneficial effects were found after regular treatment with β2-agonists (without concomitant ICS) in clinical studies. In contrast, increases in both the early bronchoconstrictor and late bronchoconstrictor and inflammatory response to allergen have even been found after regular treatment with a short-acting β2-agonist (SABA).25,26 In addition, an increase in airway inflammation, as reflected by a higher percentage of sputum eosinophils, has been observed after regular monotherapy with the SABA terbutaline 1 mg q.i.d. when compared to as needed therapy with ipratropiumbromide. 27 There have also been studies investigating the anti-inflammatory effects of regular monotherapy with LABAs in asthma. No changes in cell differential or inflammatory markers in bronchoalveor lavage fluid were found after six and eight weeks monotherapy with either salmeterol (100 μg b.i.d.) or formoterol (24 μg b.i.d).28,29 Thus, although β2-agonists exert many anti-inflammatory effects in vitro, regular monotherapy with either SABA's or LABAs does not appear to have any anti-inflammatory effects in vivo. Monotherapy with β2-agonists may even enhance the asthmatic inflammatory process leading to a worsening of asthma control.
A possible explanation for this discrepancy may be that subsensitivity to the effect of β2-agonists develops. This β2-receptor subsensitivity can be induced by prolonged or repeated agonist binding, resulting in uncoupling of the β2-receptor from the stimulatory G-protein. This is known as desensitization and regulated by receptor phosphorylation. After this desensitization, internalization of the receptor can also be induced and this is referred to as receptor downregulation. The most important kinases involved in agonist-induced phosphorylation of the β2-receptor are protein kinase A and the β-adrenergic receptor kinases (βARK).30,31
Indeed, both β2-receptor desensitization and downregulation have been observed in vivo after regular use of β2-agonists. Wallin and colleagues showed by positron emission tomography that 2-week treatment with an inhaled β2-receptor agonist markedly reduces pulmonary β2-receptor density. 29 It has been proven surprisingly difficult to demonstrate desensitization to the bronchodilator effects of β2-agonists in asthmatic patients, suggesting resistance of airway smooth muscle to β2-receptor desensitization or a large receptor reserve.32–34 A loss of bronchoprotection to methacholine has been observed within four weeks of maintenance salmeterol treatment. 35 However, O'Connor demonstrated that regular treatment with terbutaline (500 μg four times daily) markedly reduced the bronchoprotective effect of terbutaline against AMP, much more than to methacholine. 36 These findings suggest that β2-receptors on mast cells may desensitize more rapidly than β2-receptors on airway smooth muscle cells (Fig. 1). Inflammatory cells (ie mast cells, eosinophils, neutrophils, macrophages, and lymphocytes) are more susceptible to β2-receptor desensitization than airway smooth muscle cells for several reasons. Firstly, they have a lower rate of transcription resulting in lower resynthesis of β2-receptors. 37 Secondly, inflammatory cells also have less receptor reserve resulting in an early decrease in functional response when receptors are lost or uncoupled. 38 Thirdly, the expression of βARK is lower in inflammatory cells resulting in decreased phosphorylation and uncoupling of β2-receptors. 39
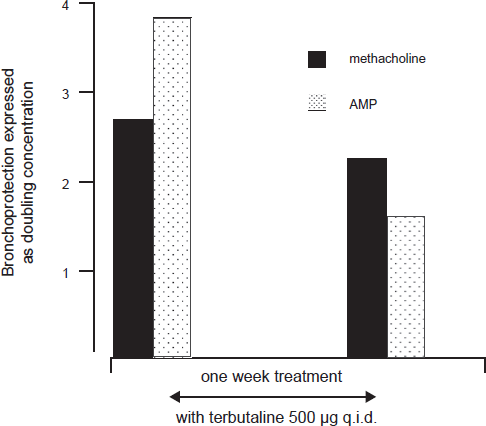
Before the seven days of treatment with terbutaline, a single dose of terbutaline reduced the PC20 methacholine by 2.7 doubling doses, but it had a greater protective effect against the PC20 AMP (3.8 doubling doses)(p, 0.001). After seven days of treatment with terbutaline (500 μg q.i.d.), the bronchoprotective effect of a single dose of terbutaline against the PC20 methacholine decreased to 2.2 doubling doses (p = 0.04). The bronchoprotective effect agains the PC20 AMP decreased even more to 1.7 doubling doses (p, 0.001). Adapted with permission from O'Connor BJ, Fuller RW, Barnes PJ. Nonbronchodilator effects of inhaled beta 2 agonists. Greater protection against adenosine monophosphate- than methacholine-induced bronchoconstriction in asthma. Am J Respir Crit Care Med. 1994;150:381-387.
Interaction between β2-agonists and ICS
Effects of corticosteroids on β2-receptors
Corticosteroids can interact with β2-agonists in a beneficial way, since they prevent desensitization at various levels including an increased β2-receptor transcription, an increased G-stimulatory protein expression, and decreased phosphorylation by reducing the level of βARK (Fig. 2).39–42 These effects occur not only in vitro, but also in humans at normally advocated doses of inhaled corticosteroids, since intranasal beclomethasone 100 μg twice daily for 3 days increases β2-receptor expression in nasal scrapings. 37 This is not necessarily very important for the bronchodilator response to β2-agonists, since airway smooth muscle cells have a large receptor reserve. However, it might be important for their anti-inflammatory effects.
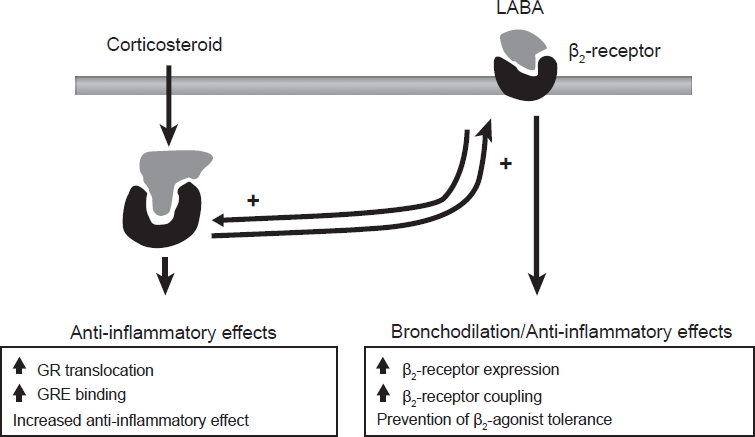
Interaction between corticosteroids and LABAs. Corticosteroids have anti-inflammatory effects but also increase the number of β2-receptors. In turn, β2-receptors induce bronchodilatation, but also enhance the anti-inflammatory effects of corticosteroids. Reproduced with permission from Barnes PJ. Scientific rationale for inhaled combination therapy with long-acting beta2-agonists and corticosteroids. Eur Respir J. 2002;19:182-191.
Mechanism of action of corticosteroids
Corticosteroids bind to glucocorticoid receptors (GR's) which are present in the cytoplasm of every cell (Fig. 3). Upon binding, the activated GR translocates to the nucleus of the cell. Once in the nucleus, the activated GR is able to exert its anti-inflammatory effects via two mechanisms. The first mechanism is called transrepression and involves the inhibition of the key pro-inflammatory transcription factors, nuclear factor -Ab (NF-κB) and activator protein-1 (AP-1).43,44 The second mechanism is called transactivation and involves the activation of anti-inflammatory genes via binding to the glucocortoid responsive elements (GRE's).45,46 GRE's are specific DNA sequences found in the promotor region of target genes. Binding of the activated GR to GRE's stimulates the production of anti-inflammatory cytokines and proteins. In this way, corticosteroids for instance upregulate mitogen activated protein (MAP) kinase phosphatase-1 (MKP-1).47–49 MKP-1 suppresses the production of many pro-inflammatory genes by dephosphorylation (and thus inactivation) of the MAP kinases, ie p38 MAP kinase, extracellular signal-regulated kinase-1 (ERK-1), ERK-2, and c-Jun-N-terminal-kinase.50–53 Other examples of anti-inflammatory mediators that are upregulated by corticosteroids are the glucocorticoid leucine zipper gene (GILZ), secretory leuko-proteinase inhibitor (SLPI), and also the β2-receptor.54–57
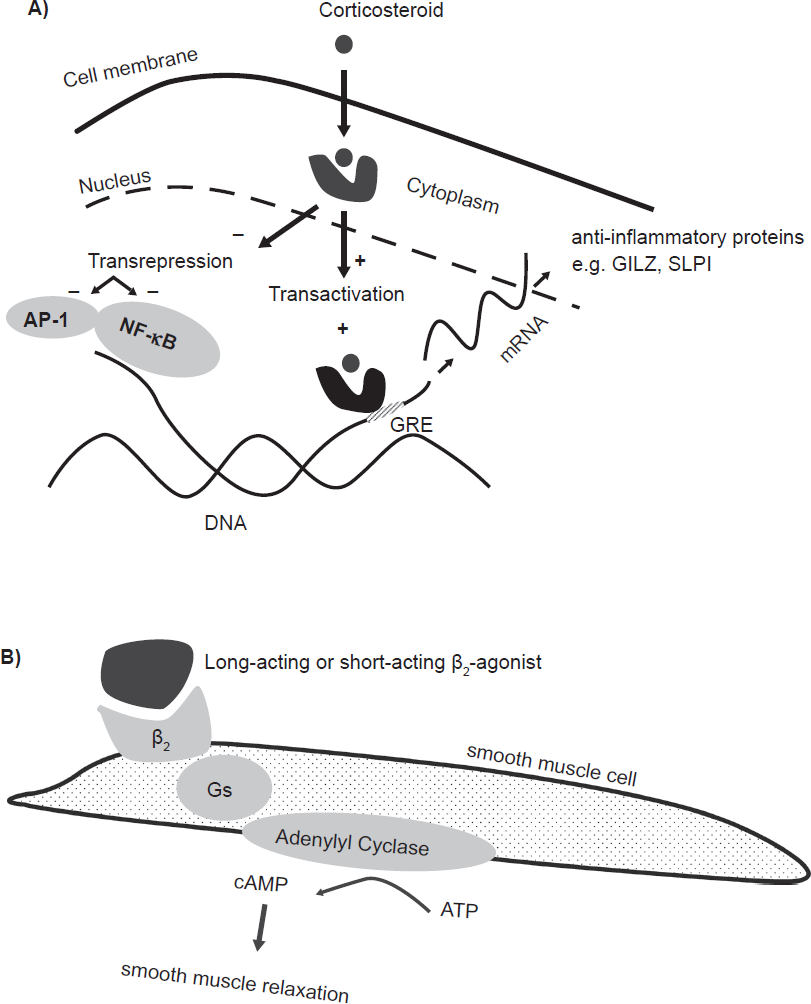
Mechanism of action of corticosteroids and long-acting β2-agonists. A) Corticosteroids bind to the glucocorticoid receptor (GR) in the cytoplasm. Upon binding, the activated GR translocates to the nucleus to exert its effects. The activated GR can bind with glucocorticoid responsive elements (GRE) in the promoter region of anti-inflammatory genes to induce the formation of anti-inflammatory mediators (transactivation). In addition, the activated GR inhibits the transcription factors AP-1 and NF-κB, which results in a decreased production of pro-inflammatory mediators (transrepression). 120 B) β2-agonists bind to β2-receptors on airway smooth muscle and cause an increase in cyclic AMP and this results in airway smooth muscle relaxation. In addition, β2-receptors exert anti-inflammatory effects (see also Fig. 2). Adapted with permission from Barnes PJ. How corticosteroids control inflammation: Quintiles Prize Lecture 2005. Br J Pharmacol. 2006;148:245-254.
Effects of β2-receptor agonist on corticosteroids
β2-agonists are capable of potentiating the anti-inflammatory actions of corticosteroids. Firstly, β2-agonists increase the expression of GR's, which is mediated by cAMP-induced stabilization of GR mRNA.58,59 Secondly, β2-agonists enhance the translocation of the GR from the cytoplasm to the nucleus.60–62 For example, in a study by Usmani and colleagues, using sputum samples of patients with asthma, inhalation of both fluticasone (500 μg) and salmeterol (50 μg) induced translocation of the GR from the cytoplasm to the nucleus in both bronchial epithelial cells and macrophages. 63 Interestingly, the combination of low dose fluticasone (100 μg) with salmeterol (50 μg) was equivalent in this respect to the higher dose of fluticasone (500 μg). In addition, it was shown in human bronchial epithelial cells (BEAS-2B) that the combination of fluticasone and salmeterol significantly increased the production of anti-inflammatory proteins such as MKP-1 and SLPI compared to fluticasone alone. 63 When combining ICS and LABA in vitro, Spoelstra and colleagues showed that salmeterol and formoterol enhanced the inhibitory effects of fluticasone and budesonide on tumor necrosis factor (TNF)-α-induced expression of intercellular adhesion molecule-1 and vascular adhesion molecule-1 on human lung fibroblasts. 20 Furthermore, salmeterol and fluticasone have been shown to inhibit the rhinovirus-induced release of IL-8 and RANTES from human bronchial epithelial cells (BEAS-2B) in an additive manner.64,65 Finally, Roth and colleagues demonstrated that the addition of formoterol increases the effect of budesonide to inhibit proliferation of human airway smooth muscle cells through activation of the cell-cycle control protein p21. 61 The latter observation may have implications for patients with more severe chronic asthma in whom smooth muscle hypertrophy and hyperplasia is thought to play a considerable role in airway remodeling and clinical instability. Taken together, there is now considerable evidence from in vitro studies that corticosteroids and β2-agonists interact in a beneficial way and this could account for the favorable effects of combination therapy with ICS and LABA in asthma.
Combination of ICS and LABA in the Treatment of Asthma Patients
The LABAs salmeterol and formoterol have been introduced into the treatment of asthma in the nineties. The introduction of these LABAs initially raised concerns, because of the negative findings with regular monotherapy with short-acting β2-agonists as explained above.25,26 However, some concerns were taken away by Greening and colleagues who carried out the first double-blind study of 6-month duration in 426 patients with asthma. 66 They showed that patients with uncontrolled asthma despite a low dose ICS (200 μg b.i.d.) had little improvement in symptoms and morning peak expiratory flow rate (PEF) when the ICS dose was increased to 500 μg b.i.d. but much greater improvements if salmeterol (50 μg b.i.d.) was added to the same dose of beclomethasone. These findings were confirmed in the landmark FACET study. This study showed in 852 patients with moderately severe asthma that the addition of formoterol (12 μg b.i.d.) to budesonide (100 μg b.i.d.) more effectively controls symptoms and lung function than a fourfold increase in the dose of budesonide (ie 400 μg b.i.d.), and this benefit persisted during the 12 months of the study. 9 Moreover, the addition of formoterol (12 μg b.i.d.) significantly reduced the number of mild and severe exacerbations when added to both a low (100 μg b.i.d.) and a high (400 μg b.i.d.) dose of budesonide. The efficacy of ICS/LABA combination therapy in patients with asthma has been confirmed subsequently in many studies using different combinations of ICS and LABAs, ie beclomethasone/salmeterol, fluticasone/salmeterol, budesonide/formoterol, and beclomethasone/formoterol.67–70 Several new combinations are currently under investigation, ie mometasone/formoterol and ciclesonide/formoterol.(www.clinicaltrials.gov) Although it is likely that these new combinations will have similar beneficial effects, this has yet to be formally demonstrated.
Combination Therapy with ICS/LABA in a Single Inhaler versus Concurrent Therapy with Two Separate Inhalers
Patient compliance
Treatment with single inhaler containing both an ICS and LABA has the advantage that it simplifies the management of asthma patients and this is likely to increase patient compliance.71,72 In agreement with this, Rosenhall and colleagues found a lower number of withdrawals during their 12-month study after treatment with budesonide/formoterol in a single inhaler compared to treatment with budesonide and formoterol administered via separate inhalers (9% versus 19%, p = 0.008). 73 In addition, two retrospective observational cohort studies using pharmacy data have shown that patient compliance increases when combination therapy (fluticasone/salmeterol or budesonide/formoterol) is administered in a single inhaler when compared to treatment with both separate inhalers.74,75 However, patient compliance may still be low even with single inhaler combination therapy, It has been reported that the adherence (ie% of days that medication is supplied) and persistence (ie percentage of patients who continued their treatment for one year) is 22% and 9% for patients using fluticasone./salmeterol. 76
Efficacy
Several studies have directly compared the efficacy of fluticasone/salmeterol to fluticasone and salmeterol in separate inhalers. Although these individual studies did not show any differences, a meta-analysis performed by Nelson and colleagues showed a small but statistically significant improvement in morning PEF with fluticasone/salmeterol administered in a single device.77–81 In addition, Zetterstrom and colleagues investigated the efficacy in morning PEF with budesonide/formoterol in a single inhaler when compared to budesonide and formoterol in separate inhalers. 82 No significant differences were found for improvement in symptoms and morning and evening peakflow, though a trend was seen during the first month. Taken together, these data might suggest a small benefit for treatment with ICS and LABA in a single inhaler, which may be due to a better lung deposition, improved ICS and LABA interactions at receptor or post-receptor levels, or improved compliance.
Clinical Evidence of Additional Anti-inflammatory Effects of LABA when Added to ICS
Several clinical studies have directly investigated the anti-inflammatory effects of LABAs when added to ICS. For example, it has been shown by Li and colleagues that the addition of salmeterol (50 μg b.i.d.), but not fluticasone (100 μg b.i.d) to maintenance treatment with ICS (100 μg-500 μg beclomethasone or budesonide) significantly reduced the number of eosinophils in bronchial biopsies compared to placebo. 83 In addition, Koopmans and colleagues compared the effect of a single dose of the combination fluticasone/salmeterol (100/50 μg) to a single dose of fluticasone alone (100 μg), when given immediately prior to allergen challenge. 84 No differences in sputum inflammatory markers were found 24 hours after allergen challenge (cell differential, ECP, MPO, and IL-8). However, adding salmeterol to fluticasone reduced the allergen-induced increase in peripheral blood eosinophils and IL-5 to a greater extent than fluticasone alone. Finally, Green and colleagues showed a decrease in the percentage of sputum eosinophils when formoterol (12 μg b.i.d.) was added to budesonide (100 μg b.i.d.). 85 Thus, it has been shown both in vitro and in clinical studies that adding a LABA to maintenance treatment with ICS has additional clinically relevant anti-inflammatory effects.
Safety of LABAs
Similar to SABA's, LABAs are associated with systemic side effects such as an increased heart rate, systolic blood pressure and tremor.86,87 The level and duration of these side effects have been shown to be similar for salmeterol and formoterol at equi-effective doses. 87 Importantly, Lötvall and colleagues have shown that the systemic effects of formoterol, despite its longer duration of action, are of a similarly short duration as salbutamol. 88 Regular treatment with higher doses of β2-agonists may pose a greater risk of cardiac adverse events in patients with myocardial disease, since one study in patients with chronic obstructive pulmonary disease (COPD) showed a greater incidence of supraventricular or ventricular premature beats after a single dose of formoterol 24 μg compared to formoterol 12 μg or salmeterol 50 μg. Recently, Nelson and colleagues have performed a large safety study on the use of salmeterol in 26,335 patients with asthma. 89 They found the regular use of salmeterol (50 μg b.i.d.) to be associated with a higher risk of the primary endpoint, “combined respiratory-related death or life-threatening experience.” Subgroup analyses revealed that patients who did not concomitantly use ICS and patients of African origin were predominantly at risk. Africans are more likely to express the arg/arg genetic variation in the β2-receptor than Caucasians (25% versus 15%), a genotype that is associated with an impaired response to β2-agonists and therefore have a higher chance of worsening asthma control when on regular β2-receptor agonist treatment. 90 Therefore, it has been suggested that the increased risk in the African population might reflect a genetic predisposition. 91 On the other hand, the recent findings of Bleecker and colleagues may argue against this. They showed that patients with the arg/arg genotype have a similar outcome when treated with combination ICS + LABA therapy compared with the other genotypes (ie similar reduction in the number of exacerbations and improvement in symptoms and lung function). Another explanation for the findings of a higher mortality in African Americans with salmeterol could be a more severe asthma at the start of the study or patient behaviour such as a delay in seeking care when asthma deteriorates. The findings of Nelson and colleagues have several implications. Most importantly, LABA treatment should always be combined with ICS. Further, in African patients whose asthma is not adequately controlled with low dose ICS alone, it might be considered to first increase the dose of ICS and/or to prescribe alternative medication to improve asthma control (ie a leukotriene antagonist, low dose theophylline, or an anticholinergic agent), but consensus on this has not been reached.
Pharmacology of LABAs: Differences between Formoterol and Salmeterol
Both salmeterol and formoterol are highly potent and selective β2-agonists. Both drugs are more lipophilic than SABA's and this property accounts for their longer duration of action. 92 This can be explained as follows. After inhalation, both formoterol and salmeterol will first contact the epithelium. Since both drugs are lipophilic, a proportion will diffuse through the epithelial cell membrane with a subsequent release of small amounts that can activate β2-receptor. However, formoterol is less lipophilic than salmeterol and therefore a larger proportion will rapidly diffuse through the airway wall to exert a relaxation effect on airway smooth muscle cells. This property of formoterol accounts for its more rapid onset of action which is similar to that of salbutamol. 13 In addition, formoterol has a higher pharmacological efficacy than salmeterol. For example, Palmqvist and colleagues showed that inhalation of a high dose of formoterol (120 μg) one hour prior to methacholine challenge provides a significantly greater protection than a high dose of salmeterol (500 μg), with a shift in the PD20 methacholine of 4.6 and 2.8 doubling doses respectively (Fig. 4). 93 In addition, the effects of formoterol were dose-dependent, in contrast to salmeterol which did not show a clear additional effect at doses higher than 50 μg (Fig. 4). Although the higher efficacy of formoterol is paralleled with more pronounced systemic side effects, cumulative doses up to 90 μg over a 3-hour period are well tolerated. 94 Taken together, formoterol has a more rapid onset of action than salmeterol and a higher efficacy with a dose-dependent bronchoprotective effect. These properties, in combination with its favorable safety profile, make formoterol more suitable for use as both maintenance and reliever medication than salmeterol.
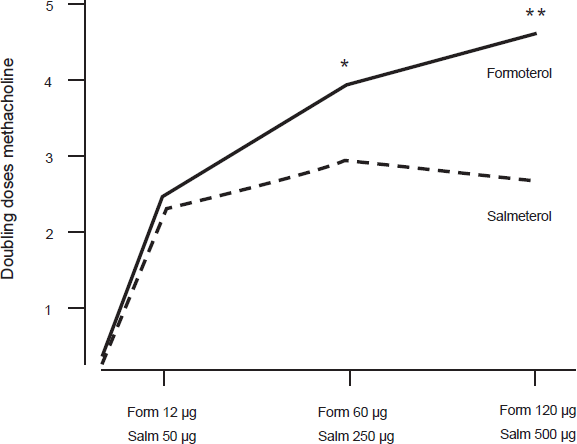
Shift in PD20 methacholine after increasing doses of formoterol and salmeterol. There was no significant difference at the lowest doses of each drug (p = 0.7). However, after both of the higher doses formoterol caused a significantly higher shift in the PD20 methacholine compared with salmeterol (p = 0.0021 and p = 0.0001). Reproduced with permission from Palmqvist M, Ibsen T, Mellen A, Lotvall J. Comparison of the relative efficacy of formoterol and salmeterol in asthmatic patients. Am J Respir Crit Care Med. 1999;160:244-249.
Two Different Approaches to Asthma Management: Fixed Dosing versus Variable Dosing
Two different approaches to asthma management have been put forward in the current literature, which are largely driven by the pharmacological differences between salmeterol and formoterol. The first approach (Gaining Optimal Asthma Control) is promoted by the producers of fluticasone/salmeterol and recommends to step up ICS to the dose needed to achieve optimal asthma control in order to keep the patient symptom free and to prevent exacerbations. The second approach is promoted by the producers of budesonide/formoterol and recommends a low maintenance dose which can be adjusted up or down according to the clinical control of asthma. Initially, a treatment strategy with Adjustable Maintenance Dosing with budesonide/formoterol was introduced. At a later time, this concept was changed to the Symbicort Maintenance And Reliever Therapy (SMART) approach as explained below.
The gaining optimal asthma control study
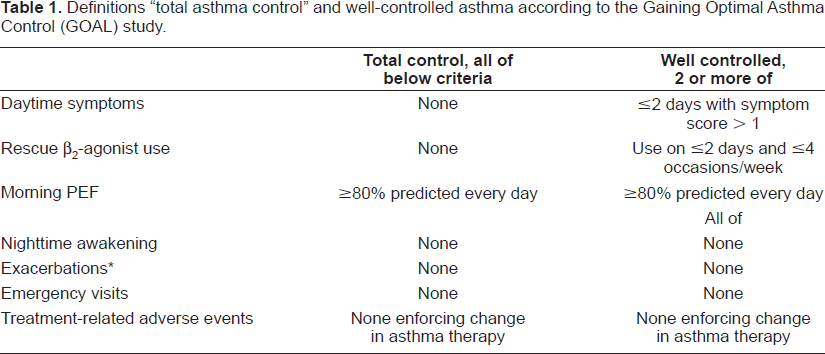
In the Gaining Optimal Asthma Control (GOAL) study, Bateman and colleagues have assessed how frequently total asthma control or well controlled asthma control can be achieved according to the criteria presented in Table 1. 95 Three groups were included: steroid-naïve, low-dose and moderate-dose ICS use at study entry, and all groups were not well controlled. The study population was randomly allocated to either increasing doses of fluticasone alone or similar doses together with salmeterol for 1 year. The study consisted of two phases. In phase 1, the dose was stepped up every 12 weeks until total asthma control was achieved or until the maximum dose was reached (fluticasone 500 μg b.i.d. or fluticasone/salmeterol 500/50 μg b.i.d.). During phase 2, patients remained on the dose necessary to achieve total asthma control (or the maximum dose) for 1 year. The percentages of patients with total asthma control and well controlled asthma at the end of phase 1 and phase 2 are presented in Figure 5. The combination of fluticasone/salmeterol was always significantly better than fluticasone alone. As shown in Figure 5, the percentage of patients achieving total asthma control and well controlled asthma further increased during sustained treatment in phase 2, and this was associated with improvements in FEV1, exacerbation rates and quality of life. This is in line with previous studies showing that long-term treatment with ICS is needed to reach maximal improvements in airway inflammation, bronchial hyperresponsiveness and airway remodeling.96–98 The findings of the GOAL study are important, since the AIRE survey in 2803 patients with asthma previously demonstrated that a large proportion of asthma patients remain symptomatic. 99 For example, 50% of the patients experienced daytime symptoms at least once a week and 30% had nocturnal awakenings at least once a week. Only 5% of the population surveyed met the goals of the GINA guidelines. Another important finding of the AIRE survey was that a large proportion of asthma patients tended to underestimate the severity of their asthma accepting a higher rate of symptoms than recommended by the guidelines. The GOAL study elegantly showed that achievement of well controlled or total asthma control is a realistic goal that can be reached in a considerable proportion of asthma patients. However, there may also be a risk for overtreatment, since the majority of patients participating in this study ended with the highest dose of inhaled corticosteroids, ie 1000 μg daily (68% with salmeterol/fluticasone and 76% with fluticasone). In contrast to the recommendations in the current GINA guideline, and according to the design of the study treatment reduction did not take place in the GOAL study when patients reached total asthma control or well controlled asthma for a certain period of time. Currently, it remains unknown which patients can step down safely and after which period of treatment and this clearly has to be sorted out in future studies.
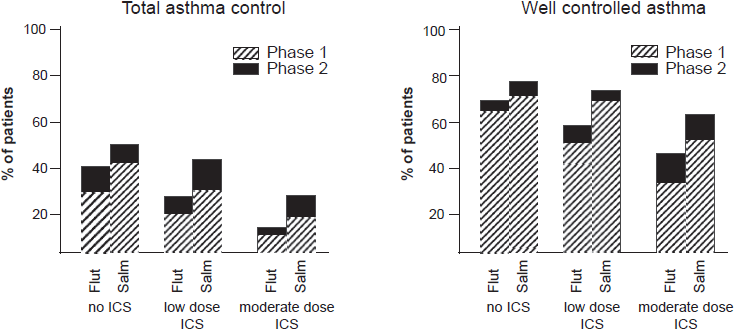
% of patients reaching the criteria for total asthma control and well controlled asthma in the GOAL study. Adapted with permission from Bateman ED, Boushey HA, Bousquet J. Can guideline-defined asthma control be achieved? The Gaining Optimal Asthma ControL study. Am J Respir Crit Care Med. 2004;170:836-844.
Definitions “total asthma control” and well-controlled asthma according to the Gaining Optimal Asthma Control (GOAL) study.
Adjustable maintenance dosing
Since worsening of asthma and exacerbations are associated with both increased airway inflammation and bronchoconstriction, studies have been initiated to evaluate the clinical value of adjusting the dose of budesonide/formoterol compared with a fixed daily dose.100–107 The principle of adjustable maintenance dosing was that patients were first stabilized on a fixed dose budesonide/formoterol (two inhalations b.i.d. of 160/4.5 μg or 80/4.5 μg). Patients randomized to fixed dosing continued with the same dose throughout the study period (3-12 months). Patients randomized to adjustable maintenance dosing reduced the dose to 1 inhalation b.i.d. if their asthma was adequately controlled (ie no reliever medication required on ≤2 days in the previous week and no nocturnal symptoms). Patients who where not adequately controlled (reliever medication required ≥3 times per day or asthma-related nocturnal awakening) increased their dose to 4 inhalations b.i.d. for 7 to 14 days. Generally, it was found that the dose of ICS was lower with the adjustable maintenance dosing strategy with a similar level of asthma control (as expressed by the number of exacerbations, symptoms and lung function). Three studies have directly compared the adjustable maintenance dosing strategy with budesonide/formoterol to a fixed dose fluticasone/salmeterol. In the CONCEPT study, Fitzgerald and colleagues found a lower number of exacerbations and less symptoms in patients using fixed dose fluticasone/salmeterol 250/50 μg b.i.d. compared to budesonide/formoterol adjustable maintenance dosing. 108 However, the CONCEPT study used a different adjustable maintenance dosing scheme with a step down dose of budesonide/formoterol that was lower than that used in all other studies with adjustable maintenance dosing (budesonide/formoterol 160/4.5 μg once daily versus b.i.d.), which may well explain the favourable results with the fixed dosing regimen.100–108 Indeed, two subsequent studies using the advocated step down dose showed no differences in asthma control between fluticasone/salmeterol 250/50 μg b.i.d. and budesonide/formoterol adjustable maintenance dosing.103,109
Symbicort Maintenance and Reliever Therapy (SMART)
Residual symptoms in asthma can be treated by increasing the maintenance dose of the ICS/LABA combination as explained above. Another option is to simply use the fixed ICS/LABA combination both for maintenance and relief, the Symbicort Maintenance And Reliever Therapy (SMART) approach. With the SMART approach, patients use a maintenance dose of budesonide/formoterol 160/4.5 μg b.i.d. or 320/9 μg b.i.d. in a single inhaler. In addition, they are allowed to use budesonide/formoterol 160/4.5 μg as needed with a maximum of extra 10 as-needed inhalations per day. The most important difference with adjustable maintenance dosing is that patients use a single inhaler with SMART (instead of one inhaler with budesonide/formoterol and a separate inhaler containing reliever medication). In addition, patients are able to more rapidly adjust their treatment up and down according to their symptoms. There are currently eight published studies investigating the SMART approach (summarized in Table 2). The first three studies compared SMART to a higher maintenance dose of budesonide.110–112 These studies showed a decrease in the number of exacerbations as well as improvement in FEV1 and symptoms with the SMART approach. However, these results could be expected, since the FACET study already showed that combination therapy is superior to treatment with ICS alone. 9 In further studies, SMART was compared with a fixed dose budesonide/formoterol (160/4.5 μg b.i.d.). 111,113,114 These studies again showed a significant reduction in the number of asthma exacerbations and improved symptoms and lung function with the SMART regimen. However, by design, higher doses of budesonide/formoterol were used with SMART and this could well explain the results. For this reason, a next randomized double-blind study was carried out to compare the SMART approach to a higher fixed dose of budesonide/formoterol 320/9 μg b.i.d.) or fluticasone/salmeterol (250/50 μg b.i.d.). 115 Although patients used lower total doses of ICS and LABA in the SMART treatment group than in the fixed dose treatment groups, similar improvements in symptoms and lung function were seen. In addition, the number of exacerbations was significantly lower with SMART. Thus, this study elegantly confirms that SMART is an effective approach to treat patients with asthma. One concern with SMART was that some patients might use the combination inhaler too frequently and could end up receiving unacceptably high doses of budesonide and formoterol. However, this was not the case in the abovementioned studies since the additional as-needed doses of budesonide/formoterol used with SMART were low (the mean number was only one extra as-needed dose per day) and very few patients required high doses. Finally, two more studies have compared the SMART approach to fixed dosing with fluticasone/salmeterol. One study compared the SMART approach using a maintenance dose of budesonide/formoterol 320/9 μg b.i.d. with additional doses of budesonide/formoterol 160/4.5 μg as needed to fixed dosing with fluticasone/salmeterol 500/50 μg b.i.d. 116 In that study, the SMART approach had a better outcome for number of exacerbations without a difference in lung function. In addition, the mean dose of ICS was lower with SMART (792 μg budesonide versus 1000 μg fluticasone). Finally, an open label study was carried out by Vogelmeier and colleagues. 117 They compared SMART to fixed dosing with fluticasone/salmeterol. With the SMART approach, the budesonide/formoterol maintenance dose could be titrated in accordance to normal clinical practice to either 160/4.5 μg b.i.d. or 320/9 μg b.i.d. In addition, patients were allowed to use budesonide/formoterol 160/4.5 μg as needed. With fluticasone/salmeterol, the dose could also be titrated to 100/50 μg b.i.d., 250/50 μg b.i.d., and 500/50 μg b.i.d. This study again showed a reduced exacerbation rate in favour of the SMART approach, while the doses of ICS used were similar (mean 653 μg budesonide per day versus 583 μg fluticasone per day. All abovementioned studies have been carried out in patients with asthma who were still symptomatic despite the use of a low dose ICS. In these patients, it has now been demonstrated that the SMART approach effectively reduces the number of asthma exacerbations. Thus far, no studies have been performed to investigate the effects of the SMART approach on direct measures of airway inflammation. This may be important, since asthma exacerbations are (amongst others) defined by an increase in symptoms and a decrease in lung function (ie FEV1 and/or morning PEF) and these parameters are more difficult to interpret when patients use a LABA. In addition, it has previously been demonstrated that airway inflammation is often not effectively suppressed during regular treatment with ICS, even when clinical symptoms are adequately controlled.118,119 Thus, there might be a risk for undertreatment with the SMART approach and this may pose a risk for asthma patients on the long-term, since uncontrolled inflammation may lead to airway remodelling and a more rapid decline in FEV1.
Overview of clinical trials investigating the SMART approach.
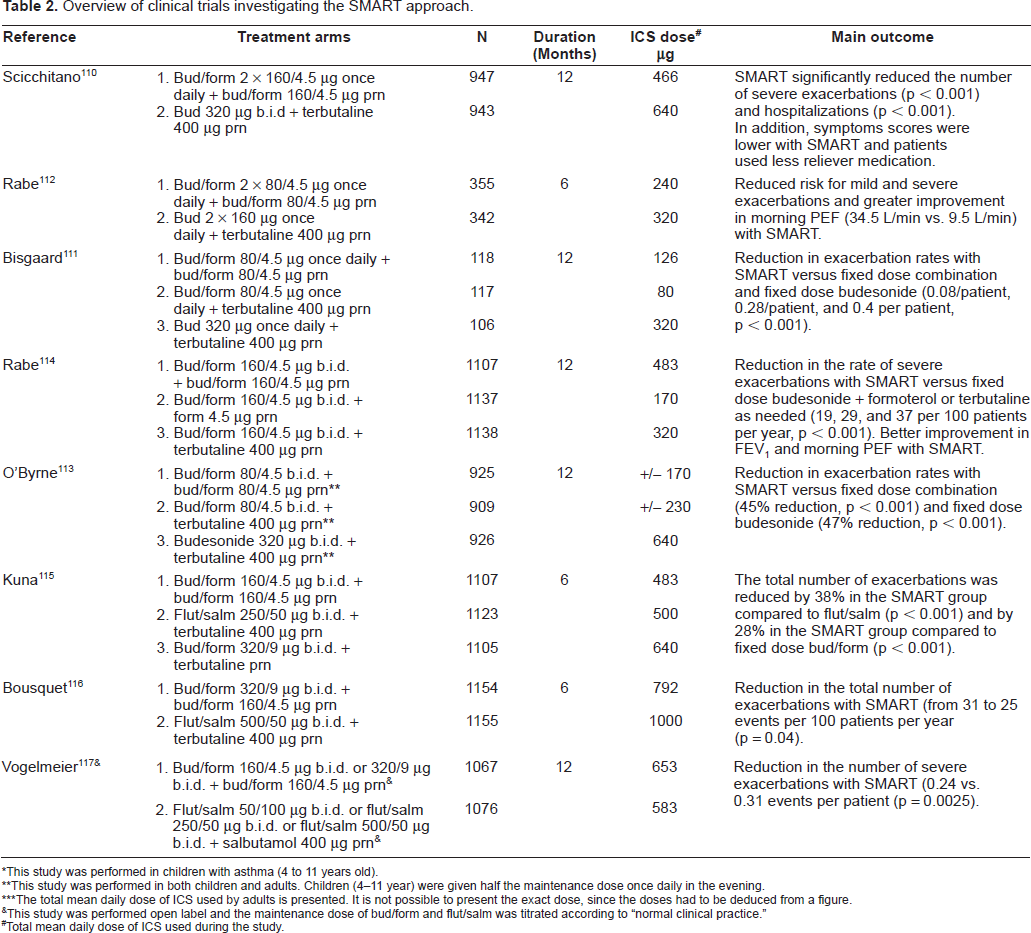
This study was performed in children with asthma (4 to 11 years old).
This study was performed in both children and adults. Children (4-11 year) were given half the maintenance dose once daily in the evening.
The total mean daily dose of ICS used by adults is presented. It is not possible to present the exact dose, since the doses had to be deduced from a figure.
This study was performed open label and the maintenance dose of bud/form and flut/salm was titrated according to “normal clinical practice.”
Total mean daily dose of ICS used during the study.
Conclusions
In recent years considerable evidence has been gained in the optimal management of adult asthma. Many patients with mild asthma are well controlled with a low dose of ICS and adding a LABA to ICS is not necessary. In patients with more severe asthma who are not well controlled with ICS alone, combination therapy with ICS/LABA is both safe and effective. There is now a considerable amount of evidence that combination therapy improves symptoms and lung function. In addition, it is associated with a significant reduction in the number of asthma exacerbations. These beneficial effects of combination therapy may, at least partly, be explained by additional anti-inflammatory effects of LABAs when added to maintenance treatment with ICS. There are important pharmacological differences between the two LABAs currently available to treat asthma, ie salmeterol and formoterol. Formoterol has a more rapid onset of action and a higher efficacy than salmeterol (which is also associated with more side effects). For this reason, the combination of budesonide/formoterol (in contrast to the combination fluticasone/salmeterol) is more suitable for use as both maintenance and reliever therapy. Currently, two different major approaches to asthma management have been put forward. The first approach is fixed dosing aimed to achieve “well controlled asthma” or “total asthma control” according to the GOAL study. With this approach, there may be a risk for overtreatment, since the majority of patients ended the study on the highest treatment dose. In the GOAL study, treatment reduction did not take place when patients reached asthma control. Future studies are needed to investigate which patients can step down safely, after which period of treatment, and according to what algorithm. The second approach is to adjust the dose according to symptoms experienced by the patient, ie the Symbicort Maintenance And Reliever Therapy (SMART) approach. With this approach, there may be a risk for undertreatment, since airway inflammation may not be effectively suppressed with asthma therapy, particularly in subjects with poor perception of asthma control. For this reason, it now becomes important to investigate the effects of the SMART approach on direct measures of airway inflammation and/or remodelling. Nevertheless, both treatment strategies have been shown to be effective, both in improving symptoms and lung function and in reducing the number of asthma exacerbations.
Disclosures
The authors have no conflicts of interest to disclose.