
Abstract
Interleukin-2 (IL-2) can provide long term durable remissions for patients with advanced or metastatic renal cell carcinoma. The perceived morbidity and the difficulties in delivering this treatment hampered its widespread use in these patients. This review aims to place IL-2 in the modern milieu by reviewing the pharmacology, efficacy and toxicity of this drug. These will be contrasted and compared with the new targeted-agents. The methodology of providing high dose IL-2 treatment, follow-up care and its impact on patient quality of life will be discussed. Importantly, the ability of these agents to provide durable, complete remissions for RCC patients will be placed in context. The goal is to provide the perspective and framework for the reader to balance the important attributes of each of these drugs during the clinical decision making process.
Introduction
Interleukin-2 (IL-2) is an important drug because it gives rise to durable complete remissions at a rate that is low (5%-10%) but seen consistently across multiple studies in patients with metastatic renal cell carcinoma (mRCC). This can occur even in patients with significant disease burden, for example such as in patients with significant organ involvement (Fig. 1) or with metastatic disease involving multiple anatomic sites.1–3

Serial computerized axial tomography of a patient before and 8 weeks after the second course of high dose interleukin-2 therapy. Note the presence of multiple bilateral lung metastases as pointed out by the arrows and the complete resolution of these deposits after therapy.
The advent of novel therapeutics engineered to directly target the molecules and receptors involved in tumor angiogenesis or signal transduction have completely changed the paradigm for treating advanced or metastatic renal cell carcinoma. The appearance of these drugs has been rapid, and there are now multiple choices, where previously only IL-2 and interferon stood. The significant clinical benefit conferred by these new agents requires a reassessment of the place of immunotherapy in RCC patients.
The understanding of IL-2's role is confounded by the concentration of knowledge and expertise into “High Dose” Centers necessitated by the technical difficulties in rendering this treatment. As a result, the perception of IL-2's severe toxicity combined with a dearth of awareness of the true power of this therapy has firmly shifted oncologists away from considering it in selecting appropriate therapy for their mRCC patients.
This review aims to place IL-2 in the modern milieu by reviewing the pharmacology, efficacy and toxicity of this drug. These will be contrasted and compared with the new targeted-agents. The methodology of providing high dose IL-2 treatment, follow-up care and its impact on patient quality of life will be discussed. Importantly, the ability of these agents to provide durable, complete remissions for RCC patients will be placed in context. The goal is to provide the perspective and framework for the reader to balance the important attributes of each of these drugs during the clinical decision making process.
Pharmacology of IL-2
Recombinant IL-2 is an approximately 15 kD highly purified protein produced using DNA technology with an
IL-2 is naturally produced in the body during an immune response and is thought to be an essential factor for T cell dependent immunity.6–8 When an antigen, such as bacteria, enters the human body it is engulfed by an antigen presenting cell such as a dendritic cell. The bacterial antigens are then processed by the dendritic cells and presented to CD8+ and CD4+ T cells within the context of both MHC class I and II molecules, respectively. The presentation of the antigen to the T cell receptor (TCR) found on lymphocytes and the activation of co-stimulatory molecules, mainly CD28, results in the secretion of IL-2 and the expression of the IL-2 receptor (IL-2R).9,10 The IL-2R consists of 3 subunits; alfa (CD25), beta (CD122), and gamma c (CD132), all of which are required for formation of the IL-2R. Once IL-2 is produced it is thought to stimulate proliferation of T cells and induce the generation of cytotoxic T lymphocytes and both lymphokine-activated and natural killer cells. 11
IL-2 is predominantly produced by activated CD4+ and CD8+ T cells, although other cells are capable of producing IL-2 such as natural killer cells. 7 Approximately 1 hour after an antigen challenge, IL-2 has begun to be secreted by CD4+ cells with around 80% of cells maximally producing IL-2 4-5 hours after initial IL-2 secretion. 12 IL-2 secretion also appears to be similar in CD8+ cells when exposed to a virus. 13
IL-2 is thought to act as an anti-cancer agent by functioning as a key growth factor for T lymphocytes. IL-2 may also have the ability to activate lymphoid cells to perform cytolytic functions, may induce the antigen independent natural killer (NK) and lymphokine-activated killer cells (LAK) and may also recruit lymphocytes to sites of malignancy.
14
More recently a review has been published questioning the mechanism of action of systemic IL-2 due to the perceived apparent success of locally applied IL-2 to tumors. 23 Otter Den and colleagues hypothesize that the primary effect of IL-2 is to cause vascular leakage resulting in edema with immunity being a secondary effect. It is argued that IL-2 results in the induction of vascular leakage which then results in massive tumor necrosis and that it is the clearance of this necrosis that leads to the induction of the immune process directed against the dead tumor cells. While this hypothesis may be partially true and necessary by itself, it is not sufficient to elicit the clinical effect. The current consensus is that IL-2 functions primarily as a T cell growth and recruitment factor and that vascular leakage contributes in some part to IL-2's effectiveness.
Pharmacokinetics of IL-2
There is a limited amount of data to date on the pharmacokinetics (PK) of IL-2 in humans. Following a short bolus intravenous infusion there is a high concentration of IL-2 in the plasma. 24 In 1990 Konrad and colleagues studied the PK of IL-2 in humans revealing a bimodal clearance for this drug. 24 There is a fast component representing 86.6% of the total clearance with a median half-life of 12.9 minutes and also a slow component with a half-life of 85 minutes.
Initial PK studies also revealed that the plasma clearance of IL-2 was mostly through the kidneys, with little to no active IL-2 protein excreted in the urine.24–28 Greater than 80% of the plasma IL-2, delivered to the kidney, is metabolized to amino acids. A clearance rate of 120 ml/min was obtained after a IV bolus of IL-2. 24
Two recent reports examining the PK of IL-2 in anephric patients receiving IL-2 for metastatic kidney cancer reveal that IL-2 may be cleared by other routes independent of the kidney.28,29 In both reports, the half life of IL-2 was only slightly increased in dialysis-dependent patients and they appeared to do no worse than other IL-2 patients. There is no evidence from either of these reports that IL-2 is cleared via dialysis, either via peritoneal or hemodialysis. These reports suggest that IL-2 may be cleared by alternate routes that include degradation at tumor sites and in nonrenal tissue.
Efficacy of IL-2 in mRCC
The FDA approved dose and schedule of high dose (HD) IL-2 for metastatic renal cell carcinoma is
600,000 IU/kg (0.037 mg/kg)/dose administered every 8 hours by a 15-minute IV infusion for a maximum of 14 doses. Following 9 days of rest, the schedule is repeated for another 14 doses, for a maximum of 28 doses per course, as tolerated. 30
Since its FDA approval in 1992 for mRCC, HD IL-2 has continued to be the gold standard for inducing durable complete responses despite the recent ascendancy of tyrosine kinase inhibitors such as sunitinib (Sutent®; Pfizer, New York, NY, USA) and sorafenib (Nevavar®; Bayer Oncology, Wayne, NJ, USA).31,32
Early work in the mid 1980's by Rosenberg and colleagues established IL-2's activity in tumor models and revealed its remarkable antitumor activity. 2 HD IL-2 was initially thought to be more effective when administered concomitantly with LAK cells, until Rosenberg and colleagues showed in a 1993 report that the addition of LAK cells was no more effective than HD IL-2 alone. 33 The current HD IL-2 treatment protocols stem directly from this body of work. Published studies spanning close to two decades consistently demonstrate overall objective response rates in the range of 14%-23.2% using this HD IL-2 protocol, and with 5%-9% of these cases being complete responses.32,34–39
HD IL-2 received approval for treatment of mRCC based upon a compilation of data from seven phase II trials showing an objective response rate of 14%, with 5% and 9% being complete response (CR) and partial response (PR), respectively. 35 HD IL-2 administration is fraught with significant toxicity and has a high overall cost thereby limiting its general use. This has spawned interest in the use of alternate or lower doses of IL-2 with or without the application of other agents. Along these lines, attempts at the addition of interferon and 5-FU to IL-2 have been tried without success.37,39–41 One course of high dose IL-2 has also been investigated as adjuvant therapy in high risk kidney cancer with the aim of limiting recurrences, but this unfortunately was not shown to be more effective when compared to observation alone post-operatively. 42
One of the first attempts at the use of IL-2 in conjunction with interferon-alfa was a French led randomized trial by Negrier and colleagues. 41 They compared the response rate of therapy consisting of continuous infusion of either IL-2, subcutaneous (SQ) interferon alfa-2a alone or the combination of both therapies. 425 patients were enrolled into the three treatment arms with response rates of 6.5%, 7.5% and 18.6% for the IL-2, interferon, and combination groups, respectively. There was a statistically significant difference in response rates between either of the two single therapy groups compared to the combination therapy group (P < 0.01). At one year, event free survival was 15, 12, and 20% in each of the 3 groups; statistically there was a significant advantage in the combined cytokine therapy group (P = 0.01). The advantage of the combined cytokine therapy group in terms of event free survival and response rates did not translate into a statistically significant difference in overall survival (12, 13 and 17 months respectively) and was associated with increased overall toxicity.
Yang and colleagues initiated a randomized phase III trial in 1991 to compare high dose versus low dose IL-2 in patients with metastatic kidney cancer. 39 Patients were randomized from 1991-1993 to either 720,000 IU/kg (high dose) or 72,000 IU/kg (low dose) of IL-2, both given every 8 hours for 14 doses. In order to reflect current practice at that time, a 3rd arm was added to the trial in 1993. In this new arm, daily subcutaneous IL-2 was given 5 days per week Monday thru Friday with 250,000 IU/kg/dose given during the first week followed by 125,000 IU/kg/dose for the next five weeks. Analysis of the 1991-1993 data set comparing high versus low dose IL-2 revealed a statistically significant difference in response rates (21 versus 13%; P = 0.48), with 11 patients (7%) and 6 patients (4%) having complete responses. There was no survival difference between the two groups. In the three arm comparison group, response rates were 21, 11, and 10% with 6, 1 and 2 complete responses in the high dose, low dose and subcutaneous groups respectively. Eight of the eleven complete responses in the high dose IL-2 arm remained disease free at a median of 9.3 years. The survival of patients completely responding to high dose therapy was significantly better than complete responders treated with low dose IL-2 (P = 0.04). The results reveal that low dose intravenous IL-2 appears equivalent to subcutaneous IL-2, with significantly more overall responses and durable complete responses with high dose intravenous therapy. High dose IL-2 remained the treatment of choice for treating mRCC patients with curative intent.
A phase III randomized trial comparing subcutaneous IL-2 and subcutaneous interferon alfa-2b with high dose IL-2 in metastatic kidney cancer was initiated by the Cytokine Working Group in the late 1990's. 37 Subcutaneous IL-2 was given as 5 MIU/m2 × 3 doses on day 1, then daily 5 times a week for 4 weeks and subcutaneous interferon-alfa 2b 5 MIU/m2 three times per week for 4 weeks, both given every 6 weeks. High dose IL-2 was given at a standard dose of 600,000 IU/kg every 8 hours for 14 doses on days 1-5 and 15-19 every 12 weeks. Overall response rates were statistically better in the high dose group versus the outpatient regimen (23.2 vs. 9.9%; P = 0.018). There were also more than double the complete responses in the high dose group (8 vs. 3), but no difference in median survival (17 vs. 13 months; P = 0.211) at the time of the publication.
There are now four randomized trials that examine the relative efficacy of low dose and high dose cytokine therapies. The sum of the data point to the superiority in terms of response rate of high-dose IV bolus IL-2 and suggest that the durability of response is better when compared to regimens that involve either low-dose IL-2 and interferon-alpha, intermediate- or low-dose IL-2 alone, or low-dose interferon-alpha alone. Thus, HD IL-2 has emerged as the standard of care for the treatment of RCC in which long term remission is desired.
In 2008, the Surgery Branch at the National Cancer Institute published a retrospective analysis of response and survival in patients treated with high dose IL-2 for metastatic kidney cancer between 1986 and 2006, to reflect their 20 year experience. 36 259 patients were treated during this 20 year experience and a total of 23 patients (8.9%) experienced a complete response with an overall objective response rate of 20%. There were 2 treatment related deaths during the earliest time period when little was known about IL-2 toxicities. More relevantly however, no deaths have occurred at the NCI in the past 20 years, reflecting the current outcomes at High Dose Centers such as those in the Cytokine Working Group or at the Roswell Park Cancer Institute. The median survival has not been reached for the complete response group to date, but for the partial responders survival was more than doubled when compared to non-responders. (39.1 vs. 15.1 months).
Safety and Tolerability of IL-2
The administration of HD IL-2 results in vasodilation and capillary leak syndrome. 43 This affects every organ and so is associated with a wide array of different side effects. Every patient experiences some degree of this and these side effects tend to get worse and more pronounced as the number of cycles and doses of IL-2 increases. It is important to note that while some patients receiving HD IL-2 will experience very few side effects, others may experience life threatening side effects that require close monitoring (discussed in detail below). IL-2 effects are particularly difficult on the cardio-respiratory system; therefore, the crux of safe administration resides on careful patient selection. Patients go through a full medical history and physical examination before undergoing a battery of pre-IL-2 screening tests. Those patients who are ECOG 0 or 1, pass the screening exams and appear able to tolerate a full 5 day course of HD IL-2, are deemed suitable candidates regardless of age. In general however, we assess every patient over the age of 60 on a case-by-case basis and weight physiologic performance over chronologic age.
Pre-testing, Screening and Counseling Prior to Administration of IL-2
All patients should possess adequate cardiac, hepatic and CNS function prior to the start of treatment because of the possibility for severe side effects to these organ systems. A full laboratory assessment should be performed to assure adequate kidney and liver function prior to IL-2 treatment because of the stress placed on these organs during treatment. Although a majority of RCC patients have undergone nephrectomy in the course of treatment prior to consideration for IL-2, the criteria commonly used in clinical trials and also in our own practice is a serum creatinine <1.5 mg/dl or Cr clearance >60 ml/min. An MRI should be performed to rule out untreated brain metastases, as these have the potential to exacerbate cerebral capillary leak and are at risk of hemorrhage during treatment. Also prior to treatment our patients go through a cardiac stress test as well as pulmonary function tests to confirm lung reserve, especially important if there is a smoking history. If patients are still concurrently smoking we advise them to try and quit or at the least stop smoking for at least 2 weeks prior to admission. 44 Screening should also be performed to ensure that patients do not have a history of severe immunologic disorders such as Cohn's disease, rheumatoid arthritis, etc. as there is the potential for IL-2 to exacerbate pre-existing disorders or unmask underlying latent disorders.
Paramount to the safety and efficacy of HD IL-2 in the pre-screening stage is a complete medication history and assessment. This assessment takes into account several issues; (i) the therapeutic intention is immunoactivation, (ii) the acute and temporary impairment of hepatic and renal function as result of IL-2 administration and most importantly (iii) the potentially life-threatening changes in cardiorespiratory function as a result of capillary leak syndrome and hypotension.
Along these lines, patients should not be on any corticosteroids when considering IL-2 treatment because of their immunosuppressant nature and potential to decrease anti-tumor effectiveness. 45 We therefore require that patients receiving steroids be completely weaned off of them for at least 4 weeks prior to IL-2. This infers that any pre-existing condition that required steroids in the first place have been definitively addressed (i.e. brain metastases treated surgically or with stereotactic radiosurgery). Assessment of other immunosuppressive medications such as methotrexate should also be performed and discontinued if possible based upon patients’ individual circumstances. Inhaled and topical steroids are also discontinued prior to IL-2 and avoided throughout treatment. Both cytotoxic chemotherapy and radiation therapy cause immunosuppression and a 4-6 week recovery and washout period is standard prior to IL-2. Blood counts have to normalize during this interim.
The normal reaction to IL-2 induced hypotension requires the ability to mount an appropriate physiologic response. Anti-hypertensive medications should be stopped or tapered (if beta blocker, to avoid rebound tachycardia) prior to admission because of the potential for severe, refractory hypotension as a result of vasodilation and capillary leakage syndrome. 45 This is particularly important for beta-blockers since their negative inotropic effects can severely compromise the patient's ability to cope with any degree of hypotension and the drop in blood pressure can be sudden and profound during therapy. As a general rule we instruct the patient to hold all anti-hypertensives 72 hours prior to admission but this can vary slightly based upon the medication or patients requirements.
Since drug metabolism is bound to be altered during therapy, a full medication review also requires an understanding of the metabolism and clearance of any other prescribed outpatient medication. Other concomitant medications that have the potential to cause bleeding, such as aspirin, or have other known potential serious side effects on organ systems (i.e. statins, etc.) are also discontinued prior to admission.
The Role of Cytoreductive Nephrectomy Prior to HD IL-2 Therapy
There is evidence that surgical removal of the diseased kidney prior to immunotherapy may be beneficial. Several clinical series reports and small nonrandomized studies suggested that patients who had undergone nephrectomy before systemic therapy seemed to exhibit a higher rate of response and longer survival.46–48 This led to the study by Flanigan and colleagues that enrolled patients into a prospective comparison study of radical nephrectomy followed by interferon versus treatment with interferon alone. They found that the combination treatment resulted in significantly improved survival over that of treatment with interferon alone (median survival 11.1 to 8.1 months). Mickisch and coworkers studied 83 patients randomly assigned to either immunotherapy alone or in combination with nephrectomy. They found that radical nephrectomy before interferon-based immunotherapy substantially delayed time to progression and improved survival of patients with metastatic renal cell carcinoma who present with good performance status (overall survival: 17 months vs. 7 months; HR, 0.54; 95% confidence interval, 0.31-0.94). 49
There are no studies that directly compare nephrectomy and IL-2 to IL-2 alone. A case-controlled study by Figlin and colleagues examined 203 consecutive IL-2 patients for factors predictive of response.50,51 From this analysis the following two factors emerged as important predictors of survival in this patient population; (i) having undergone a prior nephrectomy and (ii) the time from nephrectomy to relapse. There is general consensus that in patients who can tolerate the procedure, radical nephrectomy should be carried out prior to immunotherapy with either interferon or IL-2. 52
Using Histologic and Molecular Markers to Select for IL-2 Responders
The low response rates for RCC patients receiving high dose IL-2 is one of the major issues limiting its use and thus represents a conspicuous unmet need in this field. The search for tumor features or markers that can help identify patients that might benefit from HD IL-2 has lead to a search of histologic and molecular attributes that are found predominantly in IL-2 responders.
As an example of the former strategy, Upton and co-workers analyzed 231 patient specimens to develop a predictive model based on histologic and pathologic tumor features. 53 This model was then validated on a separate independent sample of 68 metastatic RCC specimens. They found that patients with clear cell tumors possessing more than 50% alveolar features and absent of granular or papillary features have a potential IL-2 response rate of 39%. They conclude that the most favorable group consist of clear cell carcinomas possessing alveolar features and lacking papillary and granular features.
There is recent excitement surrounding the hypothesis that the cell surface molecule, carbonic anhydrase IX (CAIX), maybe a useful pretreatment marker to identify those patients that are destined to respond to IL-2. CAIX is a transmembrane protein found on up to 94% of the clear cell variant of RCC. 54 Low expression of this marker within the tumor tissue is associated with a worse outcome. In nonmetastatic patients at high risk for progression, low CAIX predicts for an outcome similar to patients with metastatic disease (P = 0.058). 54 A retrospective analysis of CAIX levels in 66 RCC patients who had previously received IL-2 therapy found that 21 of 27 (78%) responding patients had high CAIX expressing tumors compared with 20 of 39 (51%) nonresponders. This corresponds to an odds ratio of 3.3 and a P value of 0.04. Importantly, patients with high CAIX expressing tumors possessed a longer median survival (P = 0.04) and it was this patient population who survived >5 years. 55 Confirmation of these promising but preliminary results is currently ongoing in the SELECT trial, headed by the Cytokine Working Group. This prospective study will carry out histopathologic and molecular analysis, including CAIX, on patients receiving high dose bolus IL-2 for advanced RCC.
It is interesting to note that the studies discussed above show that properly guided selection of patients can give rise to response rates at or near those shown for TKIs such as sunitinib. The hope is that these studies will identify and characterize a panel of specific markers that can select for those patients capable of obtaining a curative response to IL-2.
Side Effects Emerging during Treatment with IL-2
The potential for a number of serious side effects occurring in patients during treatment weeks necessitates close observation of patients with a highly specialized team so that rapid treatment decisions can be made as a result of the wide variation in toxicities seen in individuals. There are over 40 adverse effects listed in the package insert as occurring in greater than 10% of patients and greater than 25 life-threatening Grade IV adverse events possible in greater than or equal to 1% of patients. 30 There are a number of appropriate pre-medications listed in Table 1 that are given to help diminish the side effects that will be discussed throughout this section. During treatment, attempts should be made to avoid concomitant nephrotoxic and hepatotoxic medications where appropriate.
Roswell Park Cancer Institute's IL-2 program-concurrently used medication to counteract adverse effects.
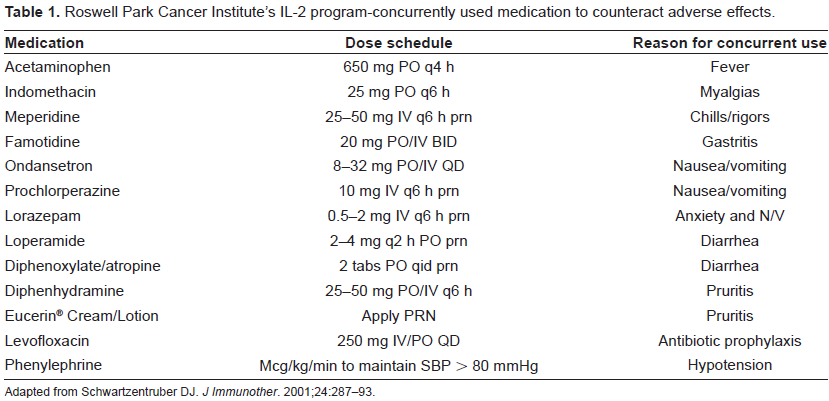
Adapted from Schwartzentruber DJ.
The most frequent and serious syndrome occurring early and throughout therapy is capillary leak syndrome. Capillary leak syndrome (CLS) is the result of extravasation of proteins and fluids into the 3rd space leading to hypotension and a resultant tachycardia. To prevent severe hypotension early on, fluid boluses should be given to maintain systolic blood pressure greater than 80-90 mmHg. 44 Crystalloid fluids are generally preferred over colloids because of equal effectiveness and decreased cost. 56 When blood pressure cannot be maintained with fluids alone, alpha agonists, such as phenylephrine are added on a mcg/kg/min basis at the lowest effective dose to maintain systolic blood pressure greater than 80-90 mmHg. Oliguria and kidney function may progressively worsen which should be monitored closely and weight heavily on the decision to hold doses when appropriate. Urine output of greater than 20-30 ml/hr is the working threshold above which additional IL-2 doses can be administered safely. CLS can also result in weight gain, progressive pulmonary edema requiring withholding of therapy, and total body edema. The latter which usually resolves post-treatment by normal physiologic mechanisms or through pharmacologic means with diuretics. 57
Fever, chills and rigors can occur anywhere from one to six hours after a dose of IL-2. To help combat fever and chills, acetaminophen and indomethacin are used around the clock with careful attention paid daily to liver function tests and serum creatinine. To help with IL-2 induced rigors, patients are usually prescribed as needed meperidine, at doses ranging from 25-50 mg every 6 hours, with careful attention paid to neurologic function during doses.
Neuropsychiatric problems and mental status changes such as irritability, confusion, depression and rarely coma have occurred with the use of IL-2. 58 Patients should be monitored closely for severe neuropsychiatric effects, with a bias for withholding doses or discontinuing therapy in these cases. Polypharmacy leading to confusion and mental status change can frequently be a problem in IL-2 patients because of a large number of medications such as anti-histamines, benzodiazepines, and opioids that are used to combat other side effects. It can often be difficult to distinguish between side effects from medications and true neuropsychiatric side effects from the IL-2, so practitioners should err on the side of caution when deciding on continued dosing of IL-2. Focal neurologic signs and symptoms are not normal during IL-2 therapy, and thus any suggestion of focality requires consideration of a space occupying lesion such as cerebral hemorrhage or the development of metastatic disease. Although the latter would expectedly be unusual given that all patients undergo brain imaging during pre-IL-2 screening, we have several instances where the metastatic deposit develops in the interim or only became evident when CLS occurred in the central nervous system.
The gastrointestinal side effects of IL-2 include nausea, vomiting, dyspepsia, diarrhea and potentially gastritis in severe cases. Anti-diarrheals such as loperamide, diphenoxylate/atropine, and in severe cases opium tincture or codeine sulfate should be made available to patients on an as needed basis. Doses are rarely held for severe diarrhea unless metabolic and electrolyte abnormalities became severe or if hematochezia developed. HD IL-2 is a moderately emetogenic regimen. 59 The National Comprehensive Cancer Network (NCCN) practice guidelines define this as a regimen with a 30%-90% potential risk of emesis on therapy. 59 Previous reports on HD-IL-2 nausea/vomiting/anorexia has been reported in 69, 77, 85% and 87% of cycles of HD IL-2.3,33,60,61 In actual practice, we have found that while some patients suffer very little emesis on HD IL-2, this can be a dose-limiting toxicity in a small number of patients. Ondansetron was equivalent to droperidol in controlling nausea and vomiting in one clinical study. 62 We recommend a 5HT-3 antagonist according to institutional formularies with an as needed agent such as prochlorperazine for breakthrough nausea and vomiting. Because steroids are prohibited with IL-2, they cannot be given as recommended according to NCCN guidelines for moderately emetogenic chemotherapy. Alternative anti-emetics should be added and considered in cases where nausea or vomiting is a significant problem.
Infections have been associated with the use of IL-2 and are often difficult to diagnose because of the overlap of symptoms with IL-2 and sepsis.63–66 Infectious complications are bacterial in origin, with the majority arising from gram positive bacteria. Insertion of central lines along with an IL-2 induced neutrophil dysfunction and leucopenia has placed IL-2 inpatients at this elevated risk.44,57 With the use of appropriate antibiotic prophylaxis the risk and incidence of infections in this patient population has decreased.63–66 Our current standard is to use oral levofloxacin for a total of nine days (throughout the week of IL-2 and for 4 days thereafter) or cephalexin for those unable to use levofloxacin.
Pruritis and rash can occur in approximately 42 and 24% of patients receiving HD IL-2. 30 For this reason around the clock antihistamines such as diphenhydramine or hydoxyzine are often used in patients to try and limit dermatologic complications. Along with oral anti-histamines the use of moisturizers and/or oatmeal powders should be readily available for topical use. 44
Laboratory abnormalities that most often occur during treatment include increased serum creatinine, total bilirubin, decreased platelet levels, leucopenia, and a number of electrolyte abnormalities that require standard electrolyte replacement. Serum creatinine elevation is usually the result of decreased perfusion to the kidney (pre-renal) from hypotension and decreased intravascular volume and extremely rarely is a consequence of direct damage to the kidneys. Increased bilirubin is usually a result of cholestasis and rarely does the thrombycytopenia caused by IL-2 result in the need for transfusion.67,68 Doses of IL-2 based upon lab parameters are usually held in our practice for a SCr ≥ 3 mg/dL, platelets less than 50,000/mm3, or a total bilirubin >4 mg/dL.
The onset of these toxicities can occur within hours, and their resolution can likewise follow a similarly rapid course. We measure serum troponin daily, beginning from Day 1 in order to detect the development of myocarditis (for those patients returning for week 2 of an IL-2 course) or impending cardiac toxicity (myocardial ischemia or overwork) from ongoing HD IL-2 during the week of therapy. Any cardiac conduction abnormalities, EKG changes, persistent sinus tachycardia, or elevated serum troponins (and other cardiac enzymes) will result in either withholding of doses or discontinuation of IL-2.
Post IL-2 Treatment Considerations
There are a number of considerations after infusions of HD IL-2 have been completed. First, in the immediate 24 hours, patients should continue to be monitored closely for the side effects listed above while at the same time continuing around the clock acetaminophen, indomethacin, and antihistamines. 44 Prophylactic antibiotics are also usually continued post hospital discharge for approximately 72-120 hours as an outpatient to decrease the infectious complications of IL-2, as discussed above. After, and possibly occurring during HD IL-2 therapy, a large number of patients can develop clinically significant hypothyroidism requiring medical management. 69 Screening patients that have symptoms at follow up visits and routine lab tests for hypothyroidism allow for diagnosis, with patients exhibiting clinical hypothyroidism receiving treatment with levothyroxine.
Another potential significant problem after treatment with IL-2 is delayed reactions to iodinated contract media. 70 A majority of reactions were within 4 weeks post IL-2 treatment, but some occurred months after IL-2 administration. 30 For this reason it is recommended that patients exposed to HD IL-2 who are undergoing radiologic imaging using iodinated contrast media should receive a prophylactic pharmacologic regimen containing a steroid and antihistamine. We prefer dexamethasone 8 mg 12 and 2 hours before contrast media concurrently with 50 mg of oral diphenhydramine one hour prior to contrast media.
Quality of Life (QOL) and Patient Satisfaction/acceptability on HD IL-2
The need to hospitalize patients undergoing high dose IL-2 can impact overall acceptability of this therapy. This is particularly true with the advent of new oral tyrosine kinase inhibitors (TKIs) for mRCC in which therapy takes place entirely as an outpatient. A balanced assessment about the relative merits of either of these approaches must take into account the fact that long term complete remissions have not been consistently documented with TKIs (discussed in detail below). Thus, it currently appears that TKI therapy and its associated toxicity may be life-long since patients need to be maintained on drug. In stark contrast, almost the entire morbidity of HD IL-2 is during active treatment. For those that respond, no further therapy is required to maintain this response. There are no comparative studies between these two modalities of treatment and so direct comparison can not be made between these two different approaches.
What is the QOL for patients receiving IL-2? There are very few studies that directly address this issue. A study of advanced mRCC patients undergoing nephrectomy and adjuvant tumor infiltrating lymphocytes plus IL-2 therapy for advanced renal cell carcinoma examines their QOL as compared to other malignancies (such as prostate and breast cancer) and to other severe chronic disease. 71 The survey shows that these patients report better health related quality of life than those with other malignancies and better physical function than patients with congestive heart failure. However, health related quality of life is worse than in the general population and similar or worse than in patients with hypertension or type II diabetes. It is important to realize that the investigators are studying a highly selected population of IL-2 patients who have responded to therapy or in whom the disease may have taken a more indolent course. Nevertheless, this study informs us that the QOL for patients on IL-2 can translate into tangible benefits for patients.
The Role of IL-2 in the Era of Molecular Targeting Agents
Kidney cancer is arguably one of the most active areas in oncology drug development. The FDA approval of sorafenib in December of 2005, followed a month later by sunitinib's approval was the beginning of the era of targeted therapy in RCC. The American Society of Clinical Oncology's 2007 annual meeting was an auspicious time for RCC therapy. The mTOR inhibitor, temsirolimus received its FDA approval just as the meeting began, and the meeting itself firmly consolidated the VEGF antibody, bevacizumab, as an active agent in this disease. Thus, four new agents have come to the forefront for the treatment of RCC within the past 3 years. With the excitement and optimism surrounding these new drugs, the field has firmly shifted away from the use high dose IL-2 as a result of the perceived benefits and ease in the use of TKIs.
An example of the prototype of the new TKI drugs is sunitinib (Sutent®; Pfizer, New York, NY, USA). 72 This is a small molecule inhibitor of multiple receptor tyrosine kinases, with a high degree of affinity for the vascular endothelial growth factor receptor (VEGFR) and platelet derived growth factor receptor (PDGFR). Because these receptors are critical in the angiogenesis pathway, use of these drugs in a highly angiogenic tumor such as RCC became an area of intense study.
There are no trials that directly compare any of these new drugs to HD IL-2 and the closest approximation to immunotherapy comes from several head to head comparison trials to interferon alpha 2B (Intron A®; Schering-Plough, Kenilworth, NJ, USA). In a multicenter phase 3 study, 750 patients with previously untreated, metastatic RCC were randomized to receive either repeated 6-week cycles of sunitinib (at a dose of 50 mg given orally once daily for 4 weeks, followed by 2 weeks without treatment) or interferon alfa (at a dose of 9 MU given subcutaneously three times weekly). 32 The median progression-free survival was 11 months in the sunitinib group and only 5 months in the interferon alfa group. This corresponds to a hazard ratio of 0.42 (95% confidence interval, 0.32 to 0.54; P < 0.001), and signifies a true advantage for the use of single agent sunitinib in this treatment naive population. The Global ARCC Trial tested the mTOR inhibitor temsirolimus against interferon in a 3 arm clinical trial design. 73 In this study, those patients who received temsirolimus (Torisel®; Wyeth, Madision, NJ, USA) alone had longer overall survival (hazard ratio for death, 0.73; 95% confidence interval [CI], 0.58 to 0.92; P = 0.008) and progression-free survival (P < 0.001) than did patients who received interferon alone. In both these trials, the investigators either report a better quality of life or significantly fewer severe side effects on the non-interferon arm. In light of these studies the use of interferon has waned considerably.
How does IL-2 fit within the current treatment paradigm for mRCC? One of the most important points is that
In distinct contrast, long term analysis extending close to 20 years on the 255 patients from the original seven phase II clinical trials used for the registration of IL-2, confirm a complete response rate of 7% and a partial response rate of 8%.1,30 The median response duration for all objective responders remains unchanged over several serial analyses at 54 months. Even partial responses are clinically significant since the average duration of such responses is 20 months and can last over 126 months. 30 IL-2 can result in long term durable remissions for a subset of patients with metastatic disease.
The relative toxicities for each type of treatment balances the acute severe toxicity of IL-2 against the chronic side effects of long term TKI therapy. Low grade toxicities with TKIs that can occur with regularity include fatigue (74%), diarrhea (55%), and skin toxicity (38%) for sunitinib. 75 Grade 3 or 4 myocardial infarction, congestive heart failure and bleeding are less common. Recurrence is a risk upon discontinuation and so any TKI drug holiday is short lived. The core of the decision making process for these patients is to balance the low grade but long term toxicity of TKI against HD IL-2's acute, high grade toxicity albeit with a chance of cure.
When Should HD IL-2 be Used?
The relative ease of using TKIs, their ready availability and clinical data showing efficacy in treatment naïve patients firmly planted their place in front line use for mRCC. The current National Cancer Center Network (NCCN) guidelines place TKIs and IL-2 together as front line therapy for metastatic RCC. There is an implicit notion that TKI failures can be subsequently salvaged using HD IL-2. There is now data to challenge this assumption since it appears that this particular sequence of treatments may be neither safe nor efficacious.
Cho et al report on their experience in this setting, showing a striking increase in the incidence of severe cardiac toxicities in patients who previously received sunitinib or sorafenib. 76 The toxicity risk in these patients was 40% and included sudden fatal cardiac arrest, myocarditis, atrial fibrillation with hypotension and bowel ischemia, severe angina and cardiomyopathy. The ability to adequately deliver IL-2 in these patients was likewise compromised since 26% of these patients could not receive their second week of IL-2 therapy, compared to 8.5% in historical controls. In Cho's report, only 1 of 23 patients proceeded to receive a second cycle of IL-2 and not a single patient achieved a partial or complete response to therapy. Our own experience parallels theirs; with the appearance of sudden, unpredictable life-threatening cardiac events in previous TKI treated patients. These are small patient series whose major contribution may be to point out where further investigation is warranted. The mechanism of these phenomena is currently unknown. The fact that none of the previously bevacizumab-treated patients missed their week 2 of treatment gives rise to the speculation that this effect may be linked to VEGFR inhibition however effects at other tyrosine kinases can not be ruled out.
In this context, it is important to point out that the safety and efficacy of sequencing treatment first with IL-2 followed then by TKI is well known. The initial FDA registration clinical trials for sorafenib and sunitinib mandated patients who had failed or were intolerant to cytokine therapy such as interferon or IL-2.31,32 For example, in the case of sunitinib, the major cardiac issue is hypertension (Grade 3/4, 8%) in this situation, and significant cardiac toxicities (i.e. Grade 3 decrease in LV ejection fraction; 2%, Grade 4; 0%) occur at a very low rate. 32
The capacity of IL-2 to trigger a therapeutic response depends on the patient's ability to activate and trigger an anti-tumor response. Therefore, it is not surprising that in almost every study of HD IL-2, patient performance status emerges as one of the major determinants of response.34,35 Patients with ECOG 0 or 1 respond best to HD IL-2. Thus, putting IL-2 eligible patients through non-curative therapy with TKIs may compromise their chance for a durable complete remission since their performance may slip below the optimum at the time of TKI treatment failure. The converse is not true since TKIs remain active in those patients with an ECOG score greater than 0. 77 Indeed, subgroup analyses of the temsirolimus Phase III trial show that this drug may be particularly efficacious in high risk, poorer performance status patients. 73
Conclusion
The dominant use of targeted therapies in RCC stem from the recognition that the response rates were higher, the side effects were more tolerable, and that these might be more efficacious agents than immunotherapy agents. A more measured assessment challenges all these assumptions and makes a compelling case to consider high dose IL-2
Disclosure
Dr. Wong has served either on the Speaker's Bureau or on Advisory Board for; Pfizer, Wyeth, Bayer/Onyx, and Novartis.