
Abstract
Doxycycline is a member of the tetracycline class of antibiotics and has been used clinically for more than 40 years. It is a well-tolerated drug that is bacteriostatic and acts via the inhibition of bacterial ribosomes. It is generally given at a dose of 100-mg daily or twice daily. It is well absorbed and has generally good tissue penetration. The serum half-life is 18-22 hours and dosage does not need to be adjusted in the presence of renal or hepatic impairment. Major side effects are gastro-intestinal and dermatological and it is generally contra-indicated in pregnancy or childhood because of concerns about discolouration of developing teeth and potential effects on growing bones. Drug interactions are not common although can occur with the concomitant use of methotrexate and the oral contraceptive pill, and its absorption can be reduced by the co-administration with some antacids and iron preparations. It has activity against many organisms, including Gram-positives, Gram-negatives and atypical bacteria. In addition, it appears to have some potentially clinically useful anti-inflammatory properties.
Introduction
Tetracycline antibiotics were one of the first classes developed following the introduction of penicillin G and the sulphonamides. Doxycycline (alpha-6-deoxytetracycline; see Fig. 1) was developed by Pfizer and is a semi-synthetic derivative of oxytetracycline that first became available in 1967. It has the advantage over other members of the tetracycline family of improved oral absorption and a prolonged serum half-life. Doxycycline has activity against a very broad range of Gram-positive, Gram-negative and ‘atypical’ bacteria as well as some protozoa such as malaria. It is also a useful antibiotic for prophylaxis against and treatment of several important potential biological warfare agents. As such it is widely used in many parts of the world, in particular for sexually transmitted infections, respiratory tract infections, malaria prophylaxis and for the therapy of some arthropod-borne rickettsial infections.
Chemical structure of doxycycline.
Mechanism of Action
Doxycycline inhibits bacterial protein synthesis by reversibly binding to the 30S ribosomal subunit and preventing the association of aminoacyl-tRNA with the bacterial ribosome. Further inhibition of protein synthesis occurs in mitochondria through binding to the 70S ribosomes. It is therefore a bacteriostatic drug. Doxycycline enters the cell via hydrophilic pores in the outer cell membrane and a pH-dependent active transport system in the inner cytoplasmic membrane. 1 It also inhibits apicoplast ribosomal subunits in Plasmodium falciparum, leading to impaired fatty acid synthesis and impaired heme biosynthesis late in the malarial cell cycle.2,3
In addition, it has multiple other actions including the prevention of angiogenesis and apoptosis, enhancement of gingival fibroblast attachment, and wound healing.4–6 It is known to inhibit certain matrix metalloproteases (MMPs), which are proteolytic enzymes produced by inflammatory cells. This has led to potential use in various anti-inflammatory and anti-neoplastic roles.7,8 Subantimicrobial doses of doxycycline in periodontitis inhibit collagen degradation and the action of destructive MMPs in the gingivae.9,10
Pharmacokinetics and Pharmacodynamics
Doxycycline is almost completely absorbed following oral administration in the stomach and proximal small bowel. Food or dairy products do not significantly alter absorption, unlike for tetracycline and minocycline, with serum levels only falling by 20%.11,12 It forms complexes with metal ions in food which are unstable in the acidic conditions in the stomach, and doxycycline enters the small bowel as free drug. However metal complexes formed in the duodenum are stable so a small amount of doxycycline is not absorbed. The presence of multivalent cations will impair doxycycline absorption.
There is a prolonged serum half-life of 18-22 hours, and this is not altered by impaired renal function. Peak serum levels occur 2-3 hours after oral administration and within 30 minutes after intravenous administration.12,13 A single dose of oral doxycycline 200 mg achieves peak serum concentrations of approximately 3.0-5.0 μg/mL, and a single dose of intravenous doxycycline at the same dose achieves peak serum concentrations of 4-10 μg/mL.12–14
Penetration occurs in body fluids and tissues. Doxycycline is more lipid soluble than tetracycline, so high levels are detected in a range of tissues including lymphatic fluid, peritoneal fluid, colonic tissue, prostate tissue, and breast milk. Doxycycline penetrates more readily into bacterial cells compared with other tetracyclines. 15 Doxycycline also penetrates into cerebrospinal fluid with mean levels of 0.37-1.3 μg/mL or 14%-26% of serum concentration.16–18 Concentrations are highest in excretory organs including the biliary system. 19 There is poor concentration in saliva and sputum.20,21 Accumulation occurs in teeth and bones via the formation of a stable calcium complex and leads to discolouration of teeth. Doxycycline also crosses the placenta, achieving umbilical cord plasma concentrations of 54% of maternal serum concentration. 22 The topical application of doxycycline to gingivae leads to detectable levels in gingival crevicular fluid but not serum. 23 Although oral doxycycline may reduce symptoms of ocular surface diseases (for example, meibomian gland dysfunction), it is not detectable in tear fluid samples. 24
There is variable protein binding, reported up to 82%-90%.25,26 The metabolism of doxycycline and other tetracyclines has not been investigated. More than one-third of doxycycline is excreted by the kidneys via glomerular filtration,14,26,27 and a small percentage is excreted in the bile.26,27 The remainder of doxycycline is excreted in faeces. In the presence of renal impairment, more doxycycline is excreted in faeces so that the same dose of doxycycline can be given without drug accumulation.26–28 More than 90% of an oral dose of doxycycline is eliminated from the body within 72 hours of drug administration.
There are no data on the impact of sex, pregnancy, breast-feeding or hepatic impairment on pharmacokinetics and there are limited data available on doxycycline pharmacodynamics. 19 Concentration-dependent killing or area under the curve (AUC) is considered the significant parameter for doxycycline activity however there are no AUC/MIC targets. Doxycycline exerts a post-antibiotic effect (PAE) that is concentration dependent against a variety of organisms. 29 The significance of this is uncertain because adequate serum concentrations are maintained during the dosing interval if given on a daily or twice-daily regimen. 29
Drug Interactions
Absorption is impaired by ferrous sulfate, bismuth and other antacids containing aluminium, calcium and magnesium salts.13,30–34 Doxycycline should be given 2 hours prior to or 3 hours after iron supplementation. 13 It is not reduced by concomitant ranitidine. 35 Cytochrome P450 3A4 inducers such as rifampicin will reduce serum levels due to increased hepatic metabolism. 36 Barbiturates, anticonvulsants (phenytoin, carbamazepine), sodium bicarbonate, and acetazolamide will also lower plasma doxycycline levels.37,38 Tetracyclines may lower plasma prothrombin activity, so patients on anticoagulant therapy may require reduction of their anticoagulant dosage. 39 The concurrent use of tetracycline and methoxyflurane has been reported to result in fatal renal toxicity. 40 The efficacy of oral contraceptives is impaired by concurrent doxycycline, so barrier contraception must be used during doxycycline therapy and for seven days after completion of therapy.41–43 It may also lead to breakthrough inter-menstrual bleeding. Doxycycline should be used with caution in patients with chronic alcoholism as the half-life of doxycycline is reduced. 44 Doxycycline also may displace methotrexate from its binding site, leading to elevated methotrexate levels and toxicity.34,45 Synergistic or additive effects with beta-lactams have been demonstrated experimentally with Stenotrophomonas maltophilia and Chlamydophila trachomatis with uncertain clinical significance.46,47
Dosage and Administration
Doxycycline is usually commenced with a starting dose of 200-mg daily, followed by a maintenance dose of 100-mg daily (or twice-daily for severe infections). It can be administered orally or intravenously. The oral dose should be taken with sufficient fluids and the patient should remain upright for 30 minutes following administration. The maximum recommended dose is 300-mg daily. 34 In children, when doxycycline benefits outweigh the risks, a weight-adjusted dose of 2.2 mg/kg daily or twice daily is used. A higher loading dose of doxycycline, for example 200-mg twice daily for 72 hours, is recommended for optimal dose-dependent killing in serious infections. 48 Variations exist with dosing and duration for specific indications, for example, malaria prophylaxis, syphilis, and scrub typhus. Lower doses, for example 20-mg twice daily, are used for acne vulgaris and rosacea. Topical preparations are also available for periodontitis.
Clinical Uses
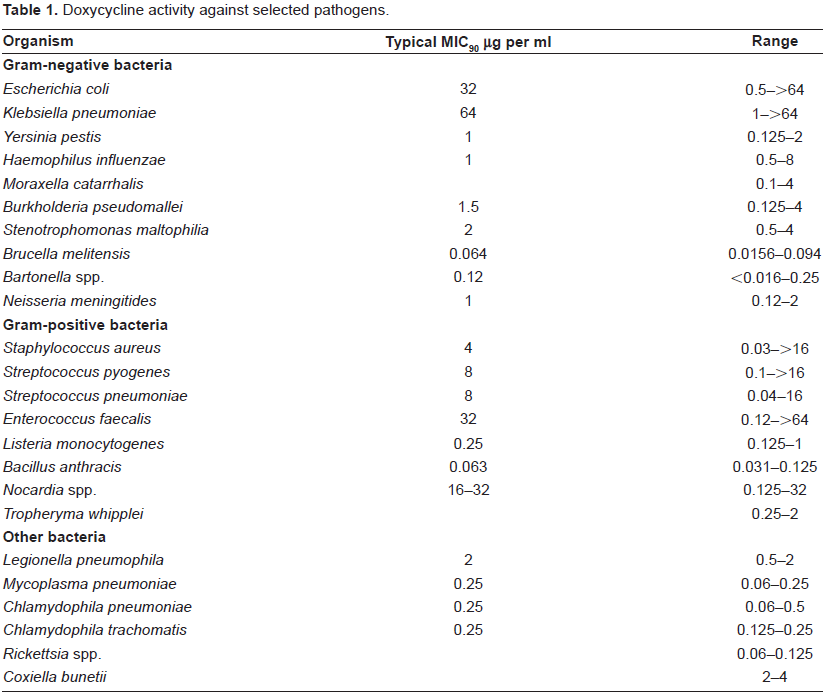
Doxycycline has a broad-spectrum of activity against many Gram-positive, Gram-negative and ‘atypical’ bacteria, as seen in Table 1. As a result, it has many potential uses.
Doxycycline activity against selected pathogens.
Respiratory infections
Doxycycline is frequently used in some parts of the world to treat respiratory tract infections such as community-acquired pneumonia (CAP) and acute exacerbations of chronic bronchitis (AECB). Its activity against ‘atypical’ bacteria such as Mycoplasma pneumoniae, Chlamydophila spp., Legionella spp. and Coxiella burnetii is reliable although resistance rates for ‘typical’ bacteria such as Streptococcus pneumoniae and Haemophilus influenzae are variable. Pneumococcal resistance rates for doxycycline range from 5%-25%.49–51 Thus, in areas where resistance rates are either high or unknown, doxycycline should be combined with another agent that has more reliable anti-pneumococcal activity, such as a beta-lactam. In Australian patients with CAP treated with doxycycline combined with either benzylpenicillin, amoxycillin or ceftriaxone, very good outcomes were obtained, 52 and outcomes have been good even for confirmed cases of legionellosis. 53 Recent randomized studies comparing doxycycline with other agents are not available. In the CAP guidelines from the Infectious Diseases Society of America/American Thoracic Society, doxycycline is listed as one of the options for treating ambulatory patients with CAP who have no risk factors for drug-resistant pneumococcal infections. 54
Doxycycline is generally listed as one of the first-line treatment options for AECB. Recent data for this is limited but in one study, it was superior to cefaclor and equivalent to amoxicillin, cephalexin and enoxacin. 55 Another small study compared it to roxithromycin and found slightly lower rates of mortality and adverse events in the roxithromycin group. 56
Genitourinary infections
For many years, seven-day courses of doxycycline were the treatment of choice for non-gonococcal urethritis (NGU) because of its reliable activity against Chlamydophila spp. With the availability of azithromycin, which can be given as a single oral dose to improve adherence, doxycycline use has decreased for this indication. Both drugs achieve similar high rates of successful outcomes of at least 97% for NGU due to Chlamydophila trachomatis. 57 Activity of doxycycline against Ureaplasma urealyticum is also good although occasional resistant strains are seen. 58 These same organisms can cause chronic prostatitis or epididymo-orchitis and four-week courses of doxycycline achieve equivalent responses to weekly doses of azithromycin for four weeks.59,60
In the guidelines for the treatment of PID from the Centers for Disease Control and Prevention, doxycycline combined with either ceftriaxone (+/- metronidazole), cefoxitin or cefotetan is recommended. 61 Because of concerns about poorer activity against M. genitalium, as well as greater ease of use with azithromycin, doxycycline is being used less commonly now in some locations.62–64 In a comparison of the treatment of PID using ceftriaxone combined with either three doses of azithromycin over two weeks or two weeks of doxycycline, better results were obtained in the azithromycin group. 65
Three-week courses of doxycycline can be used in the therapy of lymphogranuloma venereum and granuloma inguinale (donovanosis).66,67 Due to high rates of resistance, doxycycline is no longer recommended for the treatment of gonorrhoea or chancroid (Haemophilus ducreyi) without confirming susceptibility first.67,68
Cell wall deficient bacteria such as Rickettsia
Worldwide, an increasing number of species of Rickettsia are being recognised that cause human disease. These are divided based on their clinical characteristics into the spotted fever group, the typhus group and the scrub typhus group. Doxycycline is the treatment of choice for these rickettsial infections, generally given as 100-mg twice daily for 5-7 days. It is also the treatment of choice in infections caused by Ehrlichia spp. and Anaplasma phagocytophilum. 69 In most cases, response is rapid, although there have been recent reports about delayed response or reduced susceptibility in cases of scrub typhus and murine typhus. 70
Q fever infections can be self-limiting but if treatment is used in acute cases, doxycycline for 14 days is preferred. In cases of Q fever endocarditis, prolonged therapy is required, generally for 18 months and combined with another agent such as hydroxychloroquine. 71
Bartonella
Bartonella spp. can cause a variety of manifestations, including trench fever, endocarditis, pyrexia of unknown origin, cat scratch disease, bacillary angiomatosis, peliosis hepatis and splenitis, Oroya fever, verruga peruana, retinitis and pericarditis. Doxycycline has activity against Bartonella spp. and is recommended as first-line therapy for many of these conditions, either alone, or in the more serious illnesses, combined with other agents such as gentamicin or rifampicin. It is generally given for prolonged periods. 72
Spirochetal infections
In patients with early Lyme disease, treatment with doxycycline for 10-21 days is as effective as other agents such as amoxycillin or cefuroxime.73,74 One potential benefit of choosing doxycycline is that it will also have activity against Ehrlichia or Anaplasma infections that may be also be transmitted by ticks. If dissemination has occurred, with either neurologic or cardiac complications, it can still be used and should be given for 21 days, with results equivalent to intravenous penicillin G or ceftriaxone.75–77 In late cases of Lyme disease that are associated with arthritis, a month of doxycycline is effective in the majority. 78 Other Borrelia infections such as relapsing fever can also be treated with doxycycline, although there is greater experience using tetracycline and penicillins.
14-28 days of doxycycline is an alternative for treating primary or secondary syphilis in the penicillin-allergic patient. 79 It is also likely that this will be adequate treatment of endemic treponematoses such as yaws, although clinical studies about this are lacking.
Doxycycline is effective therapy for leptospirosis and is equivalent to both penicillin and cefotaxime. 80 As rickettsial infections may be prevalent in some areas with leptospirosis and the two infections may occur together or be difficult to distinguish, doxycycline is the preferred option in such locations.
Potential agents of bioterrorism
Both naturally occurring anthrax and that due to bioterrorism can be treated with doxycycline. Naturally occurring cutaneous anthrax is treated for 5-7 days while both treatment and post-exposure prophylaxis in the event of bioterrorism require 60 days of therapy. Inhalational anthrax is generally more severe and combination therapy is preferred.81,82
Tularaemia is another potential bioterrorism agent. Recommended therapy is generally streptomycin or gentamicin, although doxycycline is a suitable alternative, especially if the patient is not seriously ill. 83 Similar recommendations are made for infections due to Yersinia pestis, with 7-10 days therapy suggested and high response rates seen. 84
Malaria
For chemoprophylaxis against malaria in areas with chloroquine resistance, one of the most commonly used agents is doxycycline 100-mg daily taken from two days before entering until four weeks after leaving the malarial area. This offers protection of over 93% and is equivalent to mefloquine although the tolerability of and compliance with weekly mefloquine may be better.85–87 At lower doses, or when taken for only two weeks after travel, breakthrough cases of malaria, particularly Plasmodium vivax, are not uncommon. In general, for travel to malaria-endemic areas with chloroquine resistance, options for prophylaxis are doxycycline, mefloquine and atovaquone-proguanil. The choice is based on cost, patient preference and ability to adhere, co-morbid illnesses, history of side effects, and presence of widespread resistance to any of these agents in the travel destinations. It is important to seek up to date advice on the rates of drug-resistant malaria in the countries that will be visited.
For treatment of malaria, particularly that caused by P. falciparum, doxycycline also has a role as adjunctive therapy. It can be combined with quinine (or quinidine), mefloquine, artesunate or artemether to improve rates of cure.
Miscellaneous uses
Doxycycline can be used as a second-line treatment option combined with other agents to treat Helicobacter pylori, particularly when clarithromycin resistance is present.88,89 There is, however, greater experience with tetracycline for this indication. Ocular trachoma infections can also be treated with doxycycline although generally either oral azithromycin or topical tetracycline are preferred. 90 Following induction therapy for Whipple's disease with ceftriaxone or penicillin, doxycycline combined with hydroxychloroquine for one year can be used as maintenance therapy in patients unable to take co-trimoxazole. 91
In patients with cholera, antibiotics are an adjunct to adequate fluid and electrolyte replacement but may have a role in reducing Vibrio excretion as well as volume of diarrhoea. Doxycycline (or tetracycline) has been the treatment of choice although resistance to this class is seen.92,93 Infections due to non-cholera Vibrio spp. and Aeromonas spp., which generally involve the skin or gastro-intestinal tract but may cause septicaemic illnesses, can also be treated with doxycycline.91,92
In treating adults with brucellosis, doxycycline for 45 days combined with initial streptomycin is frequently given as first-line treatment. Substitution of gentamicin for the streptomycin leads to equivalent outcomes. 94 Alternatively, 45 days of doxycycline plus rifampicin is sometimes used and is superior to doxycycline plus a fluoroquinolone. 95 In patients with osteoarticular brucellosis, aminoglycoside-doxycycline therapy is preferred. 96 Triple antibiotic combination with doxycycline, rifampicin and an aminoglycoside appears to reduce the relapse rate. 95
Actinomycosis is another infection that can be treated with doxycycline, although penicillins are usually first-line therapy. 97 For infections due to Nocardia spp., minocycline is preferred although doxycycline maintenance therapy may be used in patients who are intolerant of this and co-trimoxazole. Melioidosis is treated initially with IV carbapenems or ceftazidime but this is then followed up with at least three months of oral therapy, generally using co-trimoxazole plus doxycycline, for which the MICs are generally low.98,99
Rat bite fever due to infection with Streptobacillus moniliformis is generally treated with penicillins although doxycycline can be substituted in the allergic patient. Occasional isolates of rapid growing mycobacteria such as M. fortuitum are susceptible to doxycycline although this is rarely used clinically. 100 Prolonged courses of doxycycline over three to six months are sometimes used to treat patients with tropical sprue. 101
An interesting newer use of doxycycline has been for Wolbachia endosymbiont infection in filarial infections such as onchocerciasis and Wuchererian filariasis. It is used for 6 weeks and by killing the symbiotic bacteria that assist in the life cycle of the filaria, interrupts embryogenesis in the adult worms for prolonged periods.102–105
Non-infectious conditions that can be treated with doxycycline
Doxycycline has also been used in a variety of non-infectious conditions. Most commonly, it can be used for severe acne, although part of its effect may be due to anti-bacterial activity against Propionibacterium acnes. Other examples of its use are in periodontitis, rosacea, bullous dermatoses, neutrophilic diseases, pyoderma gangrenosum, sarcoidosis, multiple sclerosis, the medical therapy of aortic aneurysms, autoimmune disorders such as rheumatoid arthritis and scleroderma, and as a sclerosant in pleurodesis procedures and for lymphatic or vascular malformations.106–115
An interesting potential use for doxycycline is its use in treating or preventing certain cancer metastases. This particularly relates to bone metastases from breast or prostate primaries, possibly due to the inhibition of certain MMPs that are mediators in the formation of this complication. 116 However, in vitro activity against a range of cancers has been demonstrated with members of the tetracycline family, including the recently developed molecule, Col-3.7,116
Safety
Doxycycline is generally well tolerated, especially compared with older tetracyclines and minocycline.34,117
Gastrointestinal
Common symptoms include nausea, vomiting, diarrhoea and epigastric burning. More severe reactions include oesophagitis, oesophageal ulceration, and mediastinitis. The risk of oesophageal ulceration can be reduced with the use of enteric-coated preparations, and with the monohydrate (rather than hydrochloride) formulation. Patients should take doxycycline with sufficient fluids and remain upright for 30 minutes after administration to reduce symptoms. Doxycycline should be avoided in patients with oesophageal compression or obstruction. Other gastrointestinal effects include Clostridium difficile-associated diarrhoea, although this occurs less frequently than with other antibiotics such as clindamycin. 118 Tetracycline-induced hepatotoxicity is increased in the presence of hepatic impairment, however the risk with doxycycline is lower or minimal compared with other tetracyclines. 119
Dermatological and hypersensitivity
Doxycycline may cause photosensitivity and photo-onycholysis. 120 A wide variety of skin eruptions may occur, including erythematous, maculopapular and pustular rashes, pruritus, urticaria and fixed drug eruptions. Rarely hypersensitivity and serum sickness reactions, 121 Stevens-Johnson syndrome and toxic epidermal necrolysis may occur. The Jarisch-Herxheimer reaction may occur when doxycycline is used for treatment of spirochetal infections. Anaphylaxis has also been reported.
Bones and teeth
The accumulation of doxycycline in teeth and bones leads to discolouration of teeth and is more common in deciduous rather than permanent teeth. However if they are given to children whilst permanent teeth are still in development, this may lead to lifelong discolouration. Discolouration may also occur in permanent teeth, especially with concomitant poor dental hygiene and increased sunlight exposure. 122 It may also cause enamel dysplasia and bone deformities and impairment in bone growth. 123 Premature infants administered doxycycline demonstrated a 40% reduction in fibular bone growth that was reversible upon drug cessation. 124
Neurological
Doxycycline has also been associated with benign intracranial hypertension. Symptoms usually improve upon cessation of doxycycline and concomitant administration of acetazolamide, however permanent visual acuity or visual field loss has occurred in a percentage of patients, necessitating optic nerve fenestration or CSF shunting.125,126
Other
Oropharyngeal and vaginal candidiasis from fungal overgrowth is common. Rare side effects include taste perversion, rhinitis, hiccups, and blood dyscrasias.34,117,127 Drug-induced lupus is associated with minocycline but not doxycycline, however doxycycline may exacerbate systemic lupus erythematosus. 121 There are fewer side effects when doxycycline is used in lower doses without an increase in resistance of microorganisms. 34
Pregnancy, lactation and children
Doxycycline can be given during the first 18 weeks of pregnancy but is contraindicated after this time due to potential discolouration and malformation of fetal teeth. It is potentially teratogenic in animal studies. There was a minor increase in fetal abnormalities (odds ratio 1.6, 95% confidence interval 1.1-2.3) in a large survey of over 18,000 pregnancies, however another study of 1795 doxycycline-exposed pregnancies demonstrated no increased risk of fetal abnormalities.128,129 High doses of doxycycline have been associated with fatty necrosis of the liver in pregnant women, especially those with pyelonephritis. A short course of doxycycline for 7 to 10 days is considered safe during breast-feeding if there are no other alternatives available. Otherwise they should be used with caution as doxycycline is present in breast milk and may also lead to abnormalities in tooth development in the baby. Doxycycline is contraindicated in children younger than 8 years of age due to discolouration of teeth, enamel dysplasia and possible bone deformities. In rare situations doxycycline may be administered to children with a dose of 2.2 mg/kg twice daily where benefits of doxycycline outweigh the risks, such as infections with rickettsiae, Yersinia pestis, and Burkholderia pseudomallei. 130
Efficacy
Resistance to doxycycline occurs due to acquisition of genes such as the tet and otr genes. 131 Generally they are acquired through conjugation from transposons, plasmids and integrons. The majority of these genes encode for efflux proteins that export tetracycline from the cell via an energy-dependent process. Some genes encode ribosomal protection proteins that result in ribosomal conformational changes, preventing doxycycline from binding to the ribosome. Shigella dysenteriae was the first tetracycline-resistant organism isolated. Since 1953 there has been a significant increase in doxycycline resistance in Gram-negative organisms including Enterobacteriaceae, Pseudomonodaceae, Neisseria, Haemophilus, Mannheimia, Treponema, Vibrio spp., and fastidious nonfermentative organisms such as Kingella, Eikenella and Actinobacillus spp. 1 Multi-drug resistance now occurs as tet genes are carried on integrons and plasmids with other genes encoding resistance to other antibiotics. Gram-positiveorganisms such as Staphyloccocus aureus, Streptococcus agalactiae, Enteroccocus faecalis, and Streptococcus pneumoniae have also developed doxycycline resistance and multi-drug resistance. Other organisms that may acquire tet and otr genes include Mycoplasma, Ureaplasma, Actinomyces, Nocardia and rapidly growing Mycobacterium species.
There are 2 newly discovered genes that encode tetracycline-inactivating enzymes in Bacteroides species.132,133 Doxycycline resistance rarely occurs through chromosomal mutation where permeability of outer membrane pores affects diffusion of tetracycline into the cell. Clinically important chromosomal mutations occur in H. pylori, M. avium complex and N. gonorrhoeae. As yet there is no tetracycline resistance amongst obligate intracellular pathogens and protozoa. 134 Tetracycline-resistant Chlamydophila suis has been detected in pigs, so there is potential for doxycycline resistance in chlamydophilae. 135
The increasing prevalence of doxycycline resistance in various geographic locations has limited its use as treatment for many organisms including Enterobacteriaceae, S. aureus, S. pneumoniae (including penicillin-resistant pneumococci) and Bacteroides. 136 Fortunately doxycycline remains active against a wide range of other infections where its use is now first line, for example, Coxiella burnetii, Brucella melitensis, Borrelia burgdorferi, and in penicillin-allergic patients with early syphilis.
Patient Preference
Doxycycline is inexpensive and available worldwide, and can be conveniently administered via oral or parenteral routes. This makes it practical for use in community and hospital settings. Excellent absorption and tissue distribution make it particularly useful for the severely ill patient compared with other antibiotics. Common adverse reactions such as gastrointestinal upset or oesophagitis can be prevented with careful attention to correct administration. Enteric-coated pellets have fewer gastrointestinal side effects. 34 Photosensitivity can be prevented or ameliorated with adequate attention to sun protection. It is important to remind women that the efficacy of the contraceptive pill is reduced and that barrier methods of contraception are required during and after doxycycline therapy.
Conclusions
Given its broad spectrum of activity and the wide array of clinical uses, including against some more obscure and difficult to diagnose conditions, doxycycline is sometimes referred to as the “secret weapon of the infectious diseases physician.” Although the long acting macrolide azithromycin has taken on many of its uses, it retains a very important place in the antibiotic armamentarium. It is generally well tolerated and has excellent clinical activity in many sexually transmitted infections, rickettsial and related infections, Lyme disease, brucellosis, anthrax, Q fever and atypical respiratory pathogens as well as the prevention of malaria.
Disclosure
The authors report no conflicts of interest.