
Abstract
Doxycycline is one of the most commonly used antibiotics in clinical medicine. Its broad spectrum of activity along with tolerable adverse effects makes it more palatable and compliant to patients. Improved understanding of mechanisms of actions of doxycycline has provided additional potential novel uses in clinical medicine apart from just a bacteriostatic drug. Although developed drug resistance over last few decades, doxycycline is still an essential chemical agent in the present microbiological era. This short commentary outlines safety, clinical applications and efficacy of doxycycline in clinical and microbiological fields.
In the field of microbiology, following introduction of penicillines and sulphonamides, tetracyclines were next in line to be introduced in 1945 by Dr. Benjamin Duggar as the new generation of broad-spectrum antibiotics. The group of tetracyclines are classified according to their derivation into natural and semi-synthetic and also according to their duration of action into short-acting, intermediate-acting and long-acting tetracyclines. Doxycycline, one of the most widely used tetracyclines in clinical medicine, was first developed by Pfizer in 1966 as a semi-synthetic and long-acting tetracycline derived from oxytetracycline or methacycline. Its chemical structure makes it five to ten times more lipophilic and more plasma bound compared to its natural analogue tetracycline, thus providing more effective clinical use compared to tetracycline. A recently published review on safety and efficacy of doxycycline provides an in-depth knowledge based on evidences about practical use of this tetracycline drug in the clinical medicine. 1
Doxycycline, as with other tetracyclines, is bacteriostatic. It primarily inhibits the elongation step of protein synthesis by blocking the binding of aminoacyl-tRNA to the small ribosomal subunit. 2 A specific binding site for it on small subunit rRNA has been identified. Doxycycline activity in the intact cell depends on its uptake as sensitive bacteria accumulate the drug by active transport. 3 Over last few years, the anti-inflammatory activity of tetracycline family members have been well recognised including inhibition of protein kinase activity C, mammalian collagenases and other matrix metalloproteases as well as nitric oxide (NO) synthase activity.4,5
Ninety to one hundred percent of orally administrated doxycycline is absorbed from the gastrointestinal tract in the fasting state. The average peak concentrations, 1.5–2.1 μg/ml following a single 100 mg and 2.6–3.0 μg/ml following single 200 mg dose, are attained within 1.5–4 hours. These vary modestly with different preparations of doxycycline and nutritional status of the individual. 6 The gastrointestinal absorption may be reduced by 20% in the presence of food or milk. Tetracyclines in general, chelate divalent or trivalent cations such as calcium, iron, aluminium and magnesium, hence concurrent administration of antacids or other drugs containing these cations decreases gastrointestinal absorption of tetracyclines, although doxycycline is least affected. Doxycycline crosses the blood-brain barrier and placenta. The serum half-life of doxycycline is 14–17 hours and 22–24 hours following single and multiple doses respectively, which can be increased to 18–26 hours and 20–30 hours in severe renal impairment. In individuals with normal renal function, 20%–26% of doxycycline is excreted in urine and 20%–40% is excreted in feces within 48 hours as active drug.
Doxycycline is usually commenced with an initial dose of 200 mg daily, followed by maintenance dose of 100 mg once or twice depending upon the severity of infection. The duration of treatment depends on the type and causative organism of infection and its severity. Usually, doxycycline is available in calcium, hyclate and monohydrate forms. In children, it is administrated in the dose of 2.2 mg/kg once or twice a day when its advantages outweigh its side effects. Its availability in oral as well as in parenteral forms makes doxycycline more patient-friendly and more compliant. However, one needs to be aware about potential drug interactions. Figure 1 illustrates potential drug interactions of doxycycline with other drugs.
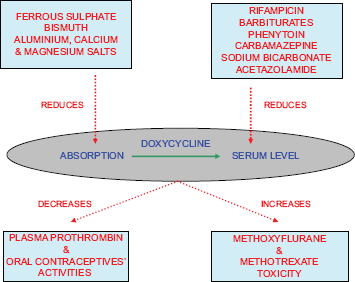
Doxycycline's interactions with other chemical agents.
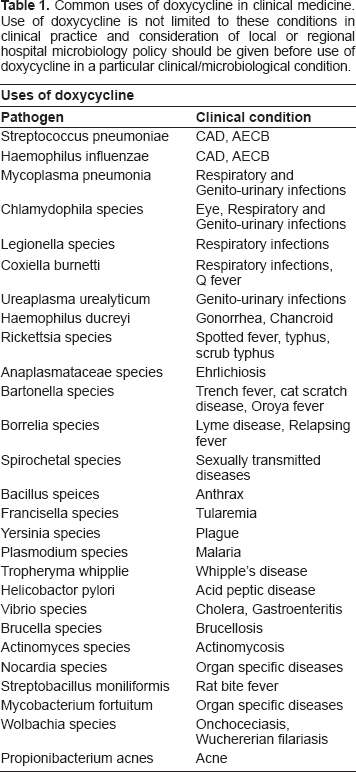
The broad-spectrum activity of doxycycline includes activity against Gram-positive, Gram-negative, atypical bacteria, Chlamydia, rickettsiae and protozoa. Apart from these, doxycycline has been shown to be effective in other conditions such as rheumatoid arthritis, abdominal aortic aneurysm, malignant pleural effusion and mesenteric ischemia. In recent years, it has been reported to have cytotoxic, anti-proliferative and anti-invasive properties in various cancer cell lines such as prostate cancer,7,8 melanoma, 5 osetosarcoma, 9 breast cancer,10,11 leukemia 12 and colorectal cancer.13,14 More general uses of doxycycline in various clinical conditions and against different organisms are detailed in Table 1. However, one needs to refer to the local or regional hospital policies and microbiology guidelines along with these before considering the use of doxycycline in particular clinical conditions as differences in geographies and populations may affect the choice and sensitivity of doxycycline in a particular condition. Other non-infectious conditions in which doxycycline may be of use include periodontitis, rosacea, bullous dematoses, neutrophilic diseases, pyoderma gangrenosum, sarcoidosis and multiple sclerosis.
Common uses of doxycycline in clinical medicine. Use of doxycycline is not limited to these conditions in clinical practice and consideration of local or regional hospital microbiology policy should be given before use of doxycycline in a particular clinical/microbiological condition.
Doxycycline is absolutely contraindicated in pediatric age group and lactating mothers, while it is not recommended in pregnancy. It should be avoided in liver diseases. The most frequent complications are abdominal pain with cramps, central nervous system toxicity, dental discoloration, diarrhea, nausea, skin photosensitivity and vomiting. Dyschromia, genital organ pruritus, glossitis, mouth irritation, oral candidiasis, pruritus ani, stomatitis and tongue discoloration may occur less frequently. Acute pancreatitis, benign intracranial hypertension and drug toxin-related hepatitis are rare side effects. As with other antibiotics, there has been the emergence of resistance against the antibiotic activity of doxycycline. Thus, initially considered as one of the strongest antibiotics in the 1960s, it has become less potent against various infections over a period of time. The main mechanisms of developing resistance include i) active efflux of drug by plasmid-encoded enzyme,15–17 and ii) ribosomal protection either by limiting the access to ribosomes or altering the ribosomes.18–20 Efflux genes and ribosomal protection genes have been found both on plasmids and chromosomes. Among these, tet and otr genes are considered responsible for the doxycycline resistance. 21 Horizontal transfer of resistance genes between normal microflora and pathogens may be responsible for the persistence of resistance against doxycycline. 20
Thus, from patient's perspectives, doxycycline is inexpensive and easily available worldwide with convenience of oral as well as parenteral administration along with less adverse and tolerable side effects. However, careful knowledge of possible drug interactions and adverse effects of doxycycline should be an essential component in clinician's medical armamentarium.
Disclosure
The author reports no conflicts of interest.