
Abstract
Objective
To determine the role of anti-annexin V antibodies (a-A5) as an etiologic factor in recurrent pregnancy failure.
Study design
Prospective observational study.
Material and methods
The study included ninety first trimester pregnant women who had a history of unexplained recurrent miscarriage (group I) with ninety well-matched pregnant women with a history of normal reproductive outcome allocated as control group (GII) and another ninety nonpregnant women (GIII). Sera from all women controls were analyzed for anti-annexin antibody measured by Elisa.
Results
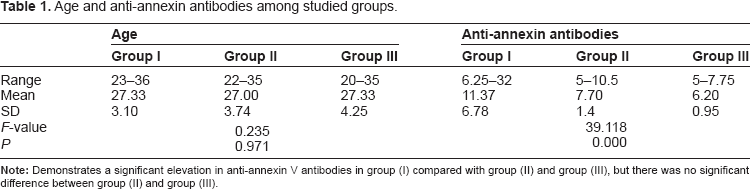
The mean value of a-A5 was 11.37 ± 6.78, 7.7 ± 1.40 and 6.20 ± 0.95 ng/ml in groups I, II and III respectively. There was a significant increase in the mean value a-A5 among women with a history of recurrent miscarriage, compared with controls. The mean value was 13.92 ± 2.42 ng/ml among patients with unfavourable outcome, compared with a corresponding value of 6.95 V 0.58 ng/ml among women with favourable outcome. The receiver operator characteristic curve revealed that the cutoff value of a-A5 was 8.61 ng/ml.
Conclusion
This study emphasizes the relationship between anti-annexin V antibodies and recurrent miscarriage.
Keywords
Introduction
Recurrent pregnancy loss (RPL) is the loss of 3 or more spontaneous consecutive pregnancies. 1 The antiphospholipid antibody syndrome is an autoimmune condition in which venous or arterial thrombosis and recurrent pregnancy losses occur in patients having serologic evidence of antibodies against anionic phospholipid protein complexes. The pathophysiologic mechanisms of this syndrome have not yet been established. 2
Annexin-V is an anionic phospholipid-binding protein with potent anticoagulant activity. It inhibits prothrombin activation and is able to prevent thrombus formation under normal venous and arterial blood flow conditions. 3
Annexins are important in various cellular and physiological processes such as providing a membrane scaffold, which is relevant to changes in the cell's shape. Also, annexins have been shown to be involved in trafficking and organization of vesicles, exocytosis, endocytosis and also calcium ion channel formation. 4 Annexins have also been found outside the cell in the extracellular space and have been linked to fibrinolysis, coagulation, inflammation and apoptosis. 5
It was shown that cells undergoing apoptosis break up the phospholipid asymmetry of their plasma membrane and expose phospholipid-like phosphatidylserine (PS) which is translocated to the outer layer of the membrane. This occurs in the early phases of apoptotic cell death during which the cell membrane remains intact. This PS exposure may represent a hallmark in detecting dying cells. 6 A number of studies suggest that displacement of annexin-V shield from the syncitiotrohpblastic surface by anti-annexin V antibodies is causative in the generation of thrombogenic environment and consequent fetal loss. 7
The diagnostic significance of anti-annexin antibodies has been studied by many authors. Yet, the results of these studies remain controversial. Some authors focus their efforts on animal models and investigate fundamental issues concerning the role of annexin antibodies in the process of thrombogenesis. 8
The aim of this work was to evaluate the prevalence of annexin V antibodies in women with early recurrent miscarriage.
Subjects and Methods
This study was carried out on 270 women recruited from the outpatient clinic of the department of Obstetrics and Gynecology of Tanta University Hospitals, during the period from January 2008 to December 2009. Cases were classified into three groups; each group includes 90 multiparous women. The first group included 90 first trimester pregnant women with history of repeated abortion, otherwise was normal and followed up till 28 weeks (age of medicolegal viability in Egypt). The second group (controls) included 90 normal first trimester pregnant women with no history of repeated abortion and followed up till 28 weeks. The third group included 90 healthy nonpregnant women with history of repeated abortion.
All women were subjected to history taking, clinical and ultrasonographic examination and routine laboratory investigations. Estimation of anti-annexin V antibodies was done by ELISA technique. 9
An informed consent was taken from each case, after proper counseling. Analysis of the results was done using the mean, standard deviation, unpaired t-test, linear correlation according to the methods described by Petrie and Sabin 10 using SPSS software statistical computer package version 12.
Results
The results of the current investigation are summarized and depicted in three tables and one figure. As regards age, there was no significant difference between the three studied groups. Concerning gravidity, in group I all cases were ≥4 gravidas; in group II 26.67% were 3rd gravida and 73.33 were ≥4 gravidas; in group III 32.22% were primigravidas, 31.11% were 2nd gravidas, 30.00% were 3rd gravidas and 6.67 & were ≥4 gravidas.
In contrast, there was a statistical significant rise in serum levels of anti-annexin antibodies among first trimester pregnant women with history of repeated abortions in comparison with the controls (Table 1). Similarly, there was a significant elevation in anti-annexin V antibodies in patients with unfavorable outcome versus controls (Table 2). The Receiver Operator Characteristic curve shows that the cutoff value of anti-annexin V antibodies was 8.61 ng/ml. The Sensitivity was 81.67%. Specificity, positive predictive value and negative predictive value were (80.83%, 81.67% and 60.0%) respectively.
Age and anti-annexin antibodies among studied groups.
Anti-annexin V antibodies concentrations (ng/ml) in relation to outcome of pregnancy among patients of group I.


Comparison of anti-annexin V antibodies (ng/ml) concentration in relation to outcome of pregnancy among patients of group I.
Discussion
Annexin V is also known as placental anticoagulant protein I, is located on the apical surface of the placental syncytiotrophoblast and, with the development of the placenta during pregnancy, a massive exposition of A5 to the circulating immune cells could occur. 8
Anti-annexin V antibodies (a-A5) have been detected for the first time 10 years ago in patients with systemic lupus erythematosus (SLE). Since then, these antibodies have been associated with the occurrence of thrombotic events and/or recurrent abortions in patients with SLE and anti-phospholipid syndrome (APLS) as well as digital ischemia in patients with systemic sclerosis (SSc). Although the mechanisms leading to the occurrence of a-A5 have not been completely elucidated, it has been proposed that in the context of increased apoptosis, extracellular/ membrane annexin V might constitute an antigenic stimulus for specific antibody production. Moreover, it is suspected that a-A5 may interfere with annexin V function(s) and exert a detrimental role leading to thrombosis and/or vascular occlusion. 11
Antibodies against annexin-V were controversially reported to be associated with recurrent abortions or failures of in-vitro-fertilization attempts.12,13 Recognition by anti-annexin V antibody of adhered annexin V on trophoblast cell structures might represent a potential pathologic mechanism by which these antibodies can cause defective placentation. 14
The current investigation demonstrated the presence of a significant elevation in anti-annexin V antibodies in the serum of first trimester pregnant women having a history of repeated abortion when compared with nonpregnant and first trimester pregnant women having no history of repeated abortion.
The association between increased levels of anti-annexin V in cases of fetal loss during pregnancy can be explained by the fact that antibodies against annexin A-V destroy its 2-dimensional crystal structure and uncover the phospholipids in the membrane, making them available for contribution to various coagulation mechanisms.15,16 Rand et al 7 and Wang et al 17 showed that the infusion of a-A5 decreases the binding of anti-annexin V to the apical surfaces of syncytiotrophoblasts in the placenta and leads to placental thrombosis, necrosis and fetal loss.
As regards the relation of anti-annexin V antibodies concentration to outcome of pregnancy (Table 3) among first trimester pregnant women having a history of repeated abortion, the present study depicted increased significant values of anti-annexin antibodies in patients with unfavorable outcome more than those with favorable outcome.
Evaluation of results of anti-annexin V antibody test for detection of abortion among studied pregnant women (group I and group II).

Bizzaro et al 18 found positive a-A5 in 17% of women with recurrent miscarriages. An important finding in this study is that 19% of the anti-cardiolipin antibodies -negative patients were a-A5 positive. Moreover, 50% of the patients with one positive antiphospholipid (APL) had positive a-A5. The latter strongly correlated with the presence of recurrent miscarriages.
In 2006, Zammiti et al 19 found that positive a-A5 and anti-b2GPI antibodies are independent risk factors for recurrent pregnancy loss.
Rand proposed that thrombosis and pregnancy loss in the antiphospholipid syndrome may be caused by disruption of this Annexin-V shield by antiphospholipid (and cofactor) antibodies, thereby increasing the net quantity of thrombogenic phospholipids exposed to the circulating blood. 2 Nojima et al found annexin V antibodies in 64% of patients with intrauterine fetal loss. 20
Arnold et al 21 found positive a-A5 in 35% of the ACL positive and in 29% of the anti-cardiolipin antibodies -negative female patients with fetal loss but suggested that a-A5 is not a risk factor for a fetal loss.
In a cohort of female patients with recurrent pregnancy loss, Ulcova-Gallova et al 22 found positive a-A5 in 13.5% of the cases.
Lastly, we conclude the presence of a relationship between anti-annexin V antibodies and recurrent miscarriage.
Publish with Libertas Academica and every scientist working in your field can read your article
“I would like to say that this is the most author-friendly editing process I have experienced in over 150 publications. Thank you most sincerely.”
“The communication between your staff and me has been terrific. Whenever progress is made with the manuscript, I receive notice. Quite honestly, I've never had such complete communication with a journal.”
“LA is different, and hopefully represents a kind of scientific publication machinery that removes the hurdles from free flow of scientific thought.”
Available to your entire community free of charge
Fairly and quickly peer reviewed
Yours! You retain copyright
Footnotes
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.