
Abstract
The relationship between miscarriage and fertility is complex. While most healthcare settings treat miscarriage as a problem of subfertility in assisted reproduction units, others believe that miscarriage occurs in super-fertile women. Infertile women undergoing assisted reproduction are at a greater risk of having a miscarriage especially at an advanced age compared with women conceiving naturally. Aberrant expression of immunological factors and chromosomal abnormalities underlie both infertility and miscarriage. Common risk factors include increased maternal age, obesity, smoking, alcohol, pre-existing medical conditions and anatomical abnormalities of the reproductive system. Management pathways of both conditions may be similar with pre-implantation genetic testing and assisted reproductive technology used in both conditions. This paper discusses the synergies and differences between the two conditions in terms of their epidemiology, etiopathogenesis, risk factors and management strategies. The two conditions are related as degrees of severity of reproductive failure with common pathways in manifestation and management.
Keywords
Infertility and miscarriage are often treated in clinical practice as two separate phenomena with distinct etiopathologies and clinical management [1]. Infertility and miscarriage are common events of human reproductive failure, with infertility affecting one in six couples of reproductive age and miscarriage occurring in 15–20% [2] of all pregnancies, but whether there is a causal relationship between the two conditions remains unclear.
Human reproduction is an inefficient process with nearly 30% of embryos being lost at the implantation stage. At post-implantation, but before the first missed menses, 30% of biochemical pregnancies are lost and can only be diagnosed by falling human chorionic gonadotropin levels. After the first missed menses, 10% of embryos are lost and are termed clinical miscarriage [3].
Research has shown that women who experience miscarriage are often labeled as subfertile [4] and infertile women have a greater risk of miscarriage [5]. On the other hand, some researchers believe that women who suffer recurrent miscarriage are actually superfertile, and the miscarriage is nature's way of controlling the number of pregnancies in these women. Furthermore, miscarriage is common after undergoing infertility treatments. These findings support the theory that infertility and miscarriage share common etiopathogenic pathways and are in fact in a continuum of human reproductive failure, with total infertility and live birth at the two extreme ends of the spectrum [6].
Human reproductive failure ranges from an inability to conceive through the incapacity to maintain pregnancy, or pregnancy loss after successful conception.

Follow-up of 1000 reproductive cycles.
If pregnancy is defined as commencing at the time of implantation, pregnancy wastage can occur at any time after the blastocyst implants in the uterus. This paper describes the synergy between the two conditions of reproductive failure – infertility and miscarriage in terms of their epidemiology, etiopathogenesis, diagnosis and management. We also highlight the differences in these aspects of the two conditions and hypothesize that these differences are of degree rather than absolute [7].
Epidemiology of infertility & miscarriage
Definition & classification
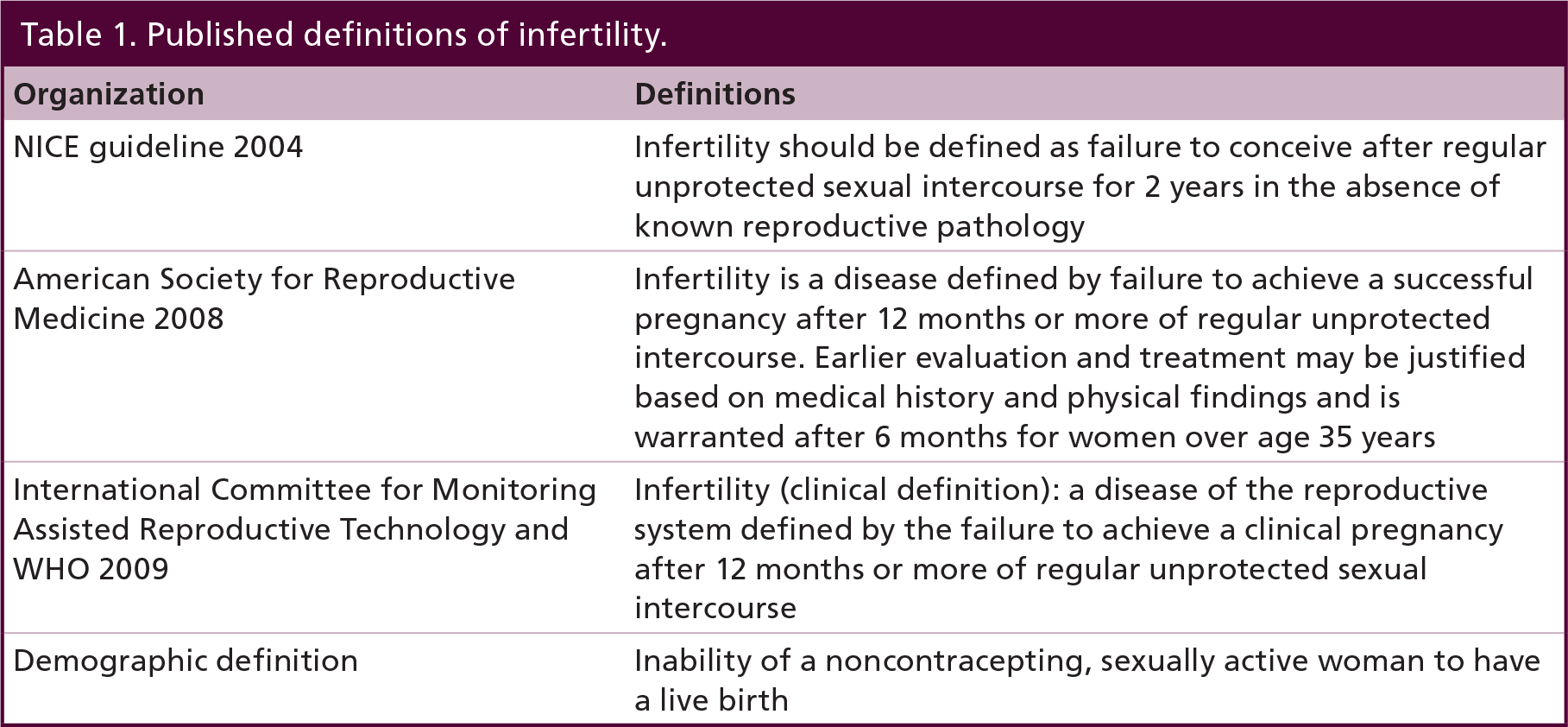
The definitions used to classify aspects of human reproductive failure lack standardization and are complicated by nomenclatures used by some authors and not by others, making comparability between studies difficult. The medical literature differentiates between a clinical/epidemiological versus a demographical definition of infertility (
The World Health Organization and the International Committee for Monitoring Assisted Reproductive Technology defines infertility as ‘a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse’ [8]. This definition stems from the biological observation that 85–90% of noncontracepting couples of normal reproductive health will achieve conception within a year [9,10]. The epidemiological definition of infertility lengthens the 12-month period to 24 months or more, while the demographic approach extends this even further to 5 years [11]. Other definitions however shorten this to 6 months [12]. Demographers define infertility as the inability to remain pregnant or achieve a live birth. This definition is closer to the public viewpoint as live birth rather than conception is the desired outcome.
Infertility is further classified as primary or secondary and by the etiology subtype. According to WHO, primary infertility occurs when a woman fails to achieve conception. Secondary infertility, however, arises after the achievement of a pregnancy and the failure to subsequently conceive [13].
Couples who are unable to conceive but have absence of abnormalities after an evaluation of their fertility profile are said to have unexplained or idiopathic infertility [12].
Miscarriage on the other hand, is defined by WHO as pregnancy loss due to expulsion or death of the fetus or embryo weighing <500 g, and before 20–24 weeks' gestational age [11]. Miscarriage is classified as first trimester ≥12 weeks' gestation (early) or late, which ranges from 12–24 weeks' gestation. In addition to these commonly used definitions, there are various terms in use to classify infertility and miscarriage [12].
Published definitions of infertility.
Terms used to describe miscarriage include ‘abortion’ or ‘spontaneous abortion’, however, the social stigma associated with these terms has made them less popular, and moreover may be confused with therapeutic termination of pregnancy. ‘Early fetal demise’ or ‘early pregnancy loss’ are acceptable terminology for miscarriage and are further classified depending on ultrasound or clinical parameters [3]. Depending on the timing and stage of development of conceptus, miscarriage may be termed as implantation failure or embryonic demise.
Recurrent miscarriage is defined as three or more consecutive pregnancy losses prior to 24 weeks' gestation and occurs in 1–3% of reproductive age women [14]. There is a wide debate regarding the definition of recurrent miscarriage, with some Early Pregnancy Units defining the condition as two or more miscarriages if the losses occur in women above the age of 35 or in the second trimester.
Prevalence
For both infertility and miscarriage, the prevalence within and between different geographical locations is difficult to determine, this is due to heterogeneity in terms of the definitions, nature of the sampled population, the denominator used in its calculation, exposure and outcomes [12]. For instance, according to Biovin et al., it is estimated that approximately 72.4 million women in a consensual relationship, aged 20–44 years, are infertile [16]. However, this is in contrast to the 2004 Demographic and Health Survey report by WHO on fecundity and infertility which stated that 186 million married women in developing countries aged 15–49 years were infertile due to primary or secondary infertility.
A universally quoted figure for sporadic miscarriage is one in five for clinically recognized pregnancies [17]. A miscarriage rate of 31% was found in an observational study of 200 women within 3 months of conception. A biochemical pregnancy rather than an ultrasound recognizable pregnancy was found in 41% of these women [18]. A similar study reported a miscarriage rate of 11% for clinical pregnancy and 26.9% for biochemical pregnancy. A 12% pregnancy loss was reported before 8 weeks' gestation in 630 women [19].
Thus in terms of definitions, both infertility and miscarriage are similar in that both conditions result in childlessness. Both conditions however, are defined variously in the literature and the population prevalence of the conditions are dependent on the definitions used, making a case for standardization of definitions.
Ethiopathogenesis of infertility & miscarriage
Immunological factors
The presence of paternally inherited genes in the implanted blastocyst makes it a foreign graft, which would consequently be rejected if certain factors in the maternal–fetal interface did not prevent it. Thus abnormalities in the maternal immune tolerance to a semi-allogeneic allograft may cause a miscarriage. Various immunological factors influence reproduction and lack of expression of these factors could contribute to human reproductive failure. Thus, the achievement of fertilization and pregnancy maintenance depends on the interaction between these factors. Current research implicates the role of HLA expression, integrins, antisperm antibodies (ASA), cytokines, leukemia inhibitory factor (LIF), antiphospholipid antibody (APA), mucin 1, endometrial adhesion factors and uterine natural killer cells in reproduction.
Terms and definitions recommended by the European Society for Human Reproduction and Endocrinology's Special Interest Group in early pregnancy events.

HCG: Human chorionic gonadotropin.
Contrastingly, scarce evidence supports association of T cells, antiendometrial antibodies, antitrophoblast antibodies, anti-HLA antibodies, peripheral natural killer cells and inadequacy of blocking antibodies and suppressor cells in reproduction [1]. Both organ-specific and systemic autoimmunity have been reported to be associated with an increased risk of recurrent miscarriage. Prothrombotic mechanisms, as well as direct inhibitory actions against trophoblastic activity have been demonstrated in antiphospholipid antibody syndrome associated with miscarriage. In women with recurrent miscarriage a disturbed T-helper cell profile is often seen, where reduced numbers of Tregs have been reported. These cells are necessary for regulating excessive activity of the Th1 and Th17 subsets. These cells, operating through excessive natural killer cell activity, may have antipregnancy effects and may be crucial in investigating unexplained infertility or miscarriage. [20]
HLA may impact various stages of gestation (
Presently, anti-HLA antibodies are not regarded as important factors associated with pregnancy maintenance, instead anti-HLA antibodies may be the result of later stages of pregnancy. This is reinforced by evidence in which 62% of 226 women with live births failed to develop anti-HLA antibodies, whereas those who did develop anti-HLA antibodies did so only after 28th week of gestation [29].
Antisperm antibodies mainly affect gamete development and fertilization, although they might also influence pregnancy (
Studies in the 1980s discovered that ASA-positive women had lower rates of pregnancy than ASA-negative women. However, in these earlier studies serum samples were collected only after miscarriage had occurred suggesting ASA may be a result of pregnancy loss rather than a cause [34,35]. Later studies found no association between ASA and recurrent miscarriage or outcomes of IVF pregnancies. [36–38].
Integrins are adhesion molecules that facilitate cell–substratum and cell–cell interactions, which may play a role in fertilization, implantation and development of the placenta in humans (
Primitive interactions between oocytes and the female reproductive system, gamete development and embryonic and blastocyst development and implantation may be regulated by LIF [41]. LIF expression has been detected in the fallopian tube and follicular fluid which influences oocyte transportation and fertilization and embryonic development [42]. However, one study reported that there was no association between LIF expression in follicular fluid and development of IVF embryos [43]. Alterations in LIF expression in human endometrium during implantation has been linked to human reproductive failure. In vitro endometrial cultures from fertile women indicated an increase in LIF; contrastingly LIF concentrations remained constant in infertile women whereas women who had numerous implantation failures had a decrease in LIF concentrations [44].
APA possibly affects pregnancy from the blastocyst/trophoblasts stage through parturition (
Cytokines are involved in gamete development, trophoblast invasion, implantation, placental development, decidualization and immune tolerance to pregnancy [56]. Cytotoxic reactions and tissue injury in disease are produced by Th1 whereas antibody production and promotion or eosinophil function is mediated by Th2 [57]. Thus pregnancy maintenance may depend on whether immune response is pathological or protective suggesting a possible role of cytokines in reproductive outcome [58–60]. For instance, some studies reported that women with higher rates of recurrent spontaneous abortion (RSA) had a higher concentration of Th1 cytokines whereas women with successful pregnancies had higher levels of Th2 cytokines [60–62].
Natural killer (NK) cells which are found in peripheral circulation may play a role during the various stages of pregnancy (

Immunogenetic factors involved in regulation of fertility and miscarriage.
Hemostatic pathways are intimately involved in ovulation, implantation and development of the trophoblast or placenta. Trophoblast function is affected in women with inherited or acquired thrombophilia, and consequent abnormal placentation can result in pregnancy loss or other complications of pregnancy [70]. Similar mechanisms could underlie repeat implantation failure during IVF and recurrent pregnancy loss. Complement-inhibitory proteins, maternal regulatory T cells, tryptophan-catabolizing enzymes and immunoregulatory cytokines present at the maternal–fetal interface are thought to maintain maternal tolerance to fetal antigens and thereby help in preserving the pregnancy. Hence protein C, protein S, antithrombin III, lupus anticoagulant, activated protein C resistance, immunoglobulin M and G anticardiolipin antibodies, homocysteine, Factor V Leiden, prothrombin G20210A mutation, methylenetetrahydrofolate reductase C677T mutation, antithyroglobulin antibodies have all been implicated in unexplained infertility, implantation failure and recurrent miscarriage [71,72].
Thus, depending on the point of action in the fertility process, immunological disturbances may result in either miscarriage or infertility. [73,74]
Chromosomal abnormalities
Accurately assessing the genetic contributions to infertility and susceptibility to miscarriage is difficult as other contributing components such as immunological, hormonal and advanced age are likely to have a genetic element. A current theory suggests that occurrence of most of the chromosomal abnormalities are de novo and are due to random errors created during embryonic development and gametogenesis [75]. Genetic testing of miscarriage samples has enabled miscarriage to be viewed as a rescue mechanism to impede the continued growth of an abnormal implanted pregnancy [76].
Chromosomal abnormalities are the most common causes (50%) of first trimester pregnancy losses and are associated with a reduction in fertility [77]. It is suggested that submicroscopic chromosomal alterations not identified by conventional cytogenic analysis can provide an explanation for some unexplained miscarriages [78].
Maternal advanced age associated with trisomies is the most common risk factor for infertility and miscarriage, accounting for approximately 25% of all first trimester pregnancy losses. Furthermore, other aneuploid concepts such as trisomies 1 and 19 are lost before they are clinically detected. Aberrant spermatogenesis may cause reciprocal Y-autosome translocation – t(13ql4q) is the most frequent Robertsonian translocation identified in infertile males and arises from unusual behavior of the rearranged autosomes during spermatogenesis [79,80]. In a 1990 review based on 22199 couples who experienced multiple pregnancy losses, 5% of the couples had chromosomal abnormalities (inversion and reciprocal and Robertsonian translocation). This carriership was ten-times more likely to occur in RM couples than in the normal population.
Factor V Leiden is the most frequently inherited predisposition to thrombosis [81]. It was discovered that 9% of 139 abortuses had an elevation of Factor V Leiden carrier frequency compared with 4% of 403 unselected pregnant females [82,83]. However, some studies found no association between Factor V Leiden and RM, especially if the miscarriage occurred early in pregnancy [84–86].
Sperm chromosome abnormalities, multifactorial disorders and skewed X chromosomes inactivation are some other genetic mechanisms which may influence the etiology of pregnancy loss [87]. Research of spermatozoa and RM found no substantial difference between the spermatozoa of the RM group and that of the control for the following factors: rate of aneuploidy, total rate of anomalies, hyperhaploidy and hypohaploidy and total rate of structural anomalies. However, the study did demonstrate an important difference in the incidence of chromosome breaks [88].
Chromosomal abnormalities, especially maternal age associated trisomies play a role in the etiopathogenesis of both infertility and miscarriage although the specific abnormalities implicated vary in the two conditions. While Factor V Leiden is most commonly implicated genetic predisposition to miscarriage and recurrent miscarriage, sperm chromosomal abnormalities play a greater role in male factor or unexplained infertility.
Risk factors common to infertility & miscarriage
Advanced age
Numerous studies have demonstrated the relationship between advanced age with a decrease in fertility and the increasing incidence of miscarriage [89–91]. The primary causes for the reduction in fertility are due to the decrease in oocyte number and oocyte quality. The decline in oocyte quality can be observed in IVF patients where the embryo viability decreases with age [92,93]. Aneuploidy is the main cause of miscarriage in these groups of women. Over the age of 40 years, only 50% of women are still capable of conceiving and the risk of miscarriage is five-times greater than 31–35-year-old women. Furthermore, within 10 years half of these women would have reached menopause [93].
Maternal obesity
Although maternal obesity has not been shown in the literature to be a risk factor for infertility per se, access to assisted reproduction techniques (ART) is often restricted for overweight and obese women until they have lost weight. The reason for this is that pregnancy outcomes of ART are often poor in women with a high BMI [94]. Moreover, in a meta-analysis of observational studies, Metwally et al. showed that maternal obesity was strongly associated with both the risk of sporadic and recurrent miscarriage in spontaneous and assisted conceptions [95,96].
Smoking
The harmful effect of tobacco on fertility and reproduction is under appreciated. Cumulative data supporting the evidence that cigarette smoke has an adverse effect on fertility have been summarized by several reviews [97–102]. A recent large-scale study with a sample of nearly 15,000 pregnancies investigated the time to conception. Along with smoking other factors such as ethnicity, alcohol consumption and parental age were assessed to determine their level of impact. It was discovered that failure to achieve conception within 6–12 months was linked to active smoking. This delay in conception was 54% higher in smokers than in nonsmokers [103].
Increasing risk of miscarriage (natural and assisted reproduction) has been linked to smoking through many studies [104,105]. One study using women 14–39 years old [105] found that 34.6% of women who had a miscarriage smoked, as compared with 21.8% smokers among those who did not have a miscarriage. Other studies showed that smokers required twice as many IVF cycles to conceive compared with nonsmokers. Additionally the damaging effect of smoking is more distinguishable in older women [105]. Limited data are available on the possible link between smoking and chromosomal abnormalities in abortus tissue. Nonetheless, some constituents of cigarettes such as nicotine, cyanide and carbon monoxide may result in placental deficiency and restrict embryonic and fetal growth, leading to their demise. Other effects include ovarian follicular depletion and loss of reproductive function [106].
Alcohol
Alcohol intake has been reported to show a connection with pregnancy loss. These reports, however, fail to determine the direct impact of alcohol and the influence of secondary changes consequent of alcoholism, like cirrhosis [107]. Moreover, Abel observed that blood alcohol levels >200 mg/dl could promote miscarriage [108]. Nonetheless, the link between moderate alcohol consumption and spontaneous abortion (SA) is undecided. For instance, Harlap and Shiono stated that miscarriage risk is only increased in females with habitual moderate consumption but not for moderate consumption. Furthermore, they reported a twofold increased risk of miscarriage with daily alcohol consumption compared with nondrinkers [109]. Also, Anokute has indicated a dose–response association between miscarriage and alcohol consumption [110], whereas Parazzini, among several studies have disputed this alcohol miscarriage association [111].
Currently, knowledge on the effect of alcohol consumption on fertility is limited as these studies generally depend on timing and levels of alcohol consumption [112], but in men alcohol can reduce libido and quality of sperm and cause impotence [113,114].
A study that looked at alcohol consumption in both sexes before and during ART treatment found that alcohol consumption by both partners reduced probability of a live birth and elevated the risk of a miscarriage [115]. Contrastingly, in a similar study no association was found between female fertility and alcohol consumption [116].
Pre-existing medical disorders including gynecological disorders
Polycystic ovarian syndrome (PCOS) is associated with infertility. Characteristics of PCOS that cause infertility include ovarian dysfunction and hyperinsulinemia which may disturb follicular maturation inhibiting a dominant follicle selection [6,117]. The effect of the condition on pregnancy loss is not established, but it is speculated that PCOS may indirectly increase the risk of miscarriage. The majority of PCOS patients are obese and obesity, including high BMI, increases miscarriage frequency independently of PCOS. Furthermore, insulin resistance in PCOS has a two- to four-fold greater risk of the patient developing diabetes which is associated with increased risk for SA. Additionally, high levels of luteinizing hormone in PCOS patients during the follicular is associated with miscarriage [118].
Endometriosis, a pelvic inflammatory disease has a higher prevalence in subfertile populations than the normal population. Endometriosis is also linked to reduced pregnancy rate after ART treatment. The only reliable data supporting this are meta-analysis by Barnhart et al. which found that fertilization, implantation, oocytes retrieval, estradiol concentration and pregnancy rates were lower in endometriosis patients compared with controls [119].
Thyroid auto-immunity (TAI) is found in greater prevalence in infertile women compared with parous age-matched women. This is particularly in women with PCOS and endometriosis. Women with TAI are at a significantly greater risk of pregnancy loss during the first trimester compared with non-TAI patients [120].
The use of cancer treatment regimens such as radiotherapy and aggressive chemotherapy in young cancer survivors can cause ovarian atrophy and decreased follicular stores resulting in premature menopause and permanent infertility. Fertility preservation techniques have included embryo/oocyte preservation, ART and gynecological surgeries in selected patients. For gynecological cancers such as uterine, cervical and ovarian cancers, obstetric/reproductive outcome is highly successful, although 8% of cervical cancer survivors in a large review of the literature experienced second trimester miscarriage [121,122]. For breast cancer, more than 8% of fertile survivors conceive, though limited data are available. However, the available data did not reveal any association with pregnancy loss.
Anatomical defects
Uterine septum is the congenital anomaly most closely associated with reproductive failure including infertility, miscarriage and RM [123,124]. One review found that miscarriage occurred in 79% of pregnancies in women diagnosed with septate uteri [125]. Intrauterine adhesions have been found in 7–30% of patients who have had a miscarriage. Furthermore, in women who were investigated for infertility and several of those who had failed IVF attempts, 13.5% were found with adhesions [126–128]. Other anatomical abnormalities such as endometrial polyps have been discovered at higher rates (46.7%) in infertile women with endometriosis and in lower rates (0.6–5%) in RM patients [129–131]. Uterine fibroids can also account for infertility as well as miscarriage [132].
The management of infertility & miscarriage
Follicle stimulating hormone level is normally done for measuring ovarian reserve irrespective of maternal age and menstrual regularity. CD3 follicle stimulating hormone level <10 mIU/ml is within normal range of fertility whereas a ≥10 mIU/ml is prognostic of decreased fertility [133,134].
In the management of miscarriage, research has demonstrated the importance of an early pregnancy assessment unit. The benefits have included an early confirmation of diagnosis usually on the initial visit, reduction of prolonged hospital admissions and the number of National Health Service (NHS) beds being occupied [135,136].
For miscarriage diagnosis a biochemical pregnancy loss does not entail the use of an ultrasound assessment, it comprises a history of positive pregnancy test followed by a negative pregnancy test. On the other hand, a clinical diagnosis of a miscarriage is determined by vaginal bleeding history and either vaginally passed conception substances or the discovery of an open cervical os. However, clinical characteristics should not be used as the only means to diagnose a miscarriage as discrepancies can be found within this method. Furthermore, declining levels of serum human chorionic gonadotropin, can be used to diagnose miscarriage [3], but has no role in the management of infertility.
Common management strategies
Preimplantation genetic testing includes preimplantation genetic diagnosis and screening and is the process by which embryonic cells produced by in vitro fertilization are analyzed to diagnose genetic abnormalities prior to intrauterine transfer such that only those embryos with the highest chance of survival are transferred [138]. This should logically increase the chances of IVF success, but evidence surrounding this is controversial [139]. The process can start at the stage of oocyte retrieval in IVF procedures when maternal inherited disease is tested in the oocyte nuclei. Alternatively, blastomere or trophectoderm can be used from the embryo at the six- to eight-cell stage on day 3 after fertilization.
Preimplantation genetic diagnosis aims to detect a single gene mutation, while preimplantation genetic screening screens for aneuploidies using PCR, or FISH techniques. These techniques can be used for sex determination of the embryo so that sex linked inherited disorders can be eliminated. However, misdiagnosis is relatively common and arises from the small amount of DNA available for testing, the short time period for testing and failure of amplification of the specific DNA segment.
Active and passive immunization using lymphocyte immunization and IvIg treatment have been suggested to improve the immunological recognition of pregnancies by establishment of microchimerism, reducing NK cell activity and modifying cytokine production in unexplained RM or infertility. The 2006 Cochrane review concluded, however, that this treatment was no better than placebo in preventing miscarriage [140]. Moreover, [141] Wilczinsci et al. found that treatment with PLI-induced preconception ally cytokine changes which neither indicated Th2 shift nor correlated with subsequent pregnancy success in RM or unexplained infertility.
Summary of etiopathogenesis and management options for infertility and miscarriage.
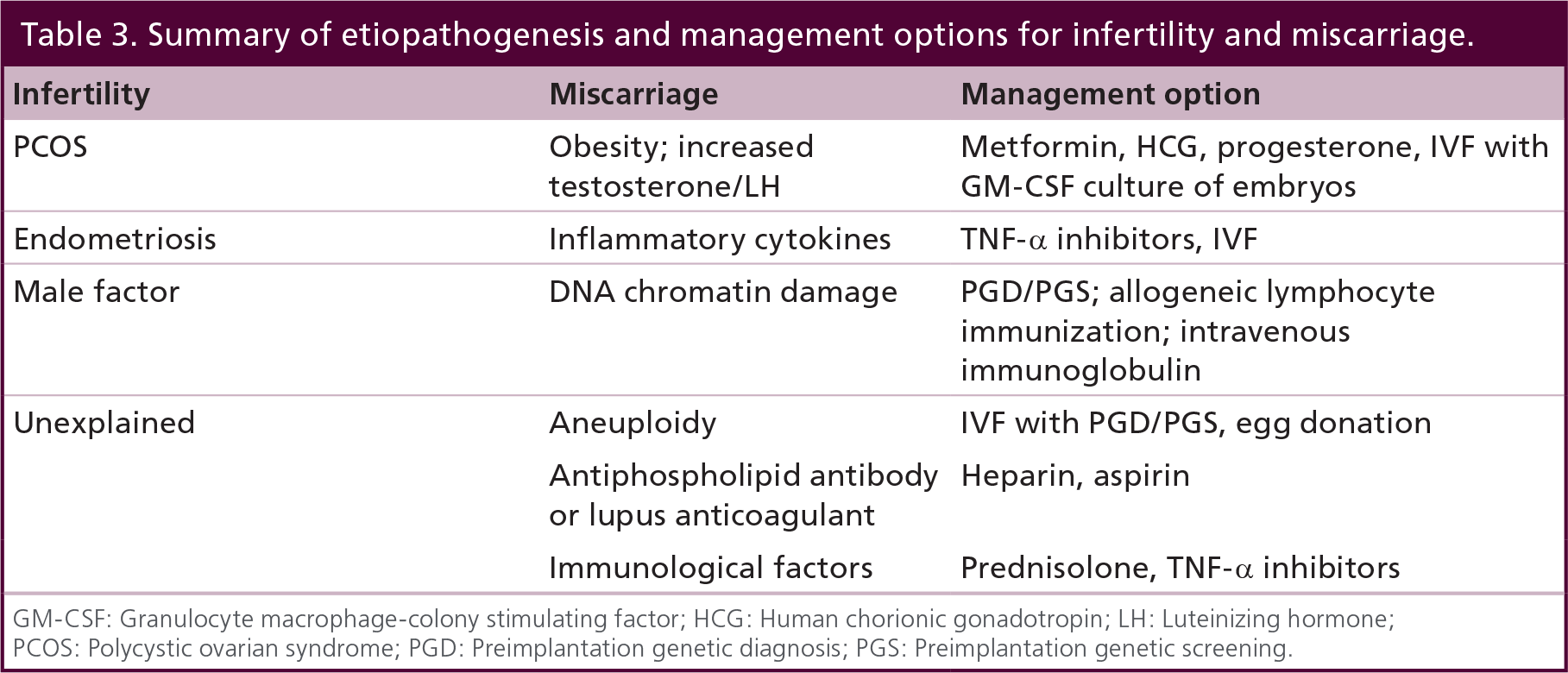
GM-CSF: Granulocyte macrophage-colony stimulating factor; HCG: Human chorionic gonadotropin; LH: Luteinizing hormone
PCOS: Polycystic ovarian syndrome; PGD: Preimplantation genetic diagnosis; PGS: Preimplantation genetic screening.
Low molecular weight Heparin with or without aspirin is often used to treat women with recurrent miscarriage [142]. Both drugs being antithrombotic agents may be effective in treating RM especially those with antiphospholipid syndrome but their role in the management of infertility is controversial. The Cochrane review on aspirin or anticoagulants for treating recurrent miscarriage in women without antiphospholipid syndrome, reported similar live birth rates in the aspirin and placebo groups [143]. It is biologically plausible that aspirin may be effective in treating miscarriages occurring in the second trimester through a similar mechanism to preeclampsia prevention by increasing placental perfusion. Stern et al. reported that heparin and aspirin did not improve pregnancy or implantation rates for APA-positive or antinuclear antibodies (ANA)-positive patients with IVF implantation failure [144]. In their systematic review, Seshadri et al. found that while nonrandomized observational studies consistently found increased clinical pregnancy and live birth rates with adjuvant heparin therapy, pooled effect measures from randomized trials did not show any improvement of outcomes [145].
Similarly, progesterone and prednisolone have both been suggested as remedies for RM. Progesterone is known to induce secretory changes and differentiation of the endometrium to facilitate implantation. It also reduces myometrial contractility and maintains the corpus luteum of pregnancy. However, the Cochrane review including 15 trials on 2118 women found no statistical difference in miscarriage rates between the progestogen and placebo or no treatment groups [146]. Prednisolone, a glucocorticoid receptor agonist, has been suggested as a treatment in RM with high number of NK cells in the uterus.
Although assisted reproductive technology is becoming increasingly popular for the management of infertility, its role in the treatment of recurrent miscarriage is controversial. Vissenberg and Goddijn in their review conclude that currently there is insufficient evidence to support the use of IVF or intrauterine insemination (IUI) for the treatment of recurrent miscarriage [147]. Nevertheless, oocyte donation in case of age-related infertility and implantation failure and immunotherapy for endometriosis may have some beneficial effects on preventing unexplained miscarriage and infertility. Moreover, surrogacy, adoption and fostering are all time-tested methods to prevent childlessness.
Conclusion & future perspective
The definitions and nomenclature used for describing conditions of subfertility and miscarriage lack standardization, making comparison of the literature difficult. There needs to be a joint effort on behalf of the learned societies and relevant international organizations for global standardized definitions of terminology in infertility and miscarriage. Advanced maternal age at the time of first conception can pose a problem for both fertility as well as pregnancy loss. Raising awareness regarding the optimum age for motherhood should start early and be a part of school-based health education. Interventions to tackle other lifestyle factors such as obesity, smoking and alcohol and substance misuse should be evaluated in the light of enhancing fecundity by means of large multicentered randomized controlled trials. In fact, lifestyle modification by reducing weight and the antidiabetic biguanide drug Metformin has met with some success in the treatment of infertility and miscarriage associated with PCOS. Active and passive immunization using allogenic lymphocyte immunization and IvIg may be improve immunological recognition of pregnancies and thus improve prognosis in some cases of infertility and miscarriage [142].
Hormonal profiling, hysterosalpingographic or ultrasound examination of the female reproductive tract, endometrial biopsy, chromosomal and immunologic analyses all play their role in the diagnostics of both infertility and miscarriage, although the extent to which each investigation adds value varies between the two conditions. For example, investigations of the anatomy of the female reproductive tract play an important role in the investigation of infertility but not miscarriage. Advances in genetic and bioassay techniques such as preimplantation genetic testing, have meant better understanding of the etiopathogenesis and consequently the management of both infertility and miscarriage. Despite this, around 30% of cases of infertility and almost 60% of first trimester miscarriage remain unexplained. Future research should focus on the biological mechanisms underpinning these unexplained conditions with a view to developing evidence-based diagnostic testing that will inform clinical and cost–effective management strategies for both conditions. Meanwhile, adoption, fostering, surrogacy and oocyte donation remain viable options for childless couples.
Executive summary
Definitions and terminology for infertility and miscarriage lack standardization making comparison between studies difficult.
The prevalence of infertility and miscarriage are difficult to determine due to heterogeneity of definitions, terminology and samples used, denominator, exposure and outcomes.
Current research implicates the role of HLA expression, integrins, antisperm antibodies, cytokines, leukemia inhibitory factor, antiphospholipid antibody, mucin 1, endometrial adhesion factors and uterine natural killer cells in reproduction.
Contrastingly, scarce evidence supports association of T cells, antiendometrial antibodies, antitrophoblast antibodies, anti-HLA antibodies, peripheral natural killer cells and inadequacy of blocking antibodies and suppressor cells in reproduction.
Lack of expression of these factors could contribute to human reproductive failure.
Chromosomal abnormalities are the most common causes of first trimester pregnancy losses and are associated with a reduction in fertility.
Novel techniques include, FISH, array comparative genomic hybridization, comparative genomic hybridization, quantitative fluorescence polymerase chain reaction, multiplex ligation-dependent probe amplification.
Cytogenic research has demonstrated that numerical abnormalities account for the majority of those losses (86%), structural abnormalities (6%) and other genetic factors including mosaicism (8%) accounts for a small percentage (6%). Balanced translocations or inversions may contribute to 50% of structural abnormalities.
Maternal advanced age associated with trisomies is the most common risk factor for infertility and miscarriage accounting for approximately 25% of all first trimester pregnancy losses.
Common risk factors associated with infertility and miscarriage include advanced maternal age, obesity, smoking and alcohol, pre-existing medical conditions such as diabestes, polycystic ovarian syndrome, endometriosis and thyroid disorders are found in greater prevalence in infertile women and are linked to pregnancy loss.
Preimplantation genetic screening can play a role in preventing miscarriage due to chromosomal abnormalities in IVF pregnancies.
Active and passive immunization using allogenic lymphocyte immunization and IvIg may improve immunological recognition of pregnancies and thus improve prognosis in some cases of infertility and miscarriage.
Heparin with or without aspirin improves success in recurrent miscarriage in women with antiphospholipid antibody or lupus anticoagulant.
Progesterone and prednisolone are potentially effective in preventing miscarriage in high-risk cases with high NK cell count.
Where miscarriage and infertility are associated with polycystic ovarian syndrome, lifestyle modification and metformin therapy have met with some success.
Important factors in managing infertility and miscarriage include cost, legal and ethical considerations.
IVF/intra-cytoplasmic sperm injection although important management strategies for infertility, play a very small role in managing miscarriage, except where preimplantation genetic diagnosis is useful.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or a financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.