
Abstract
Background
Cervical cancer is preventable with regular PAP tests and the human papillomavirus (HPV) vaccine.
Objective
Identify factors influencing initiation into regular sexual health examinations within a group of undergraduate health science students who have high parental SES.
Methods
After reviewing the literature, a survey of knowledge, attitudes and behaviors about HPV exposure and cervical cancer prevention through vaccination and cervical cancer screening was developed. The survey was circulated using a web-based survey tool to undergraduate Faculty of Health Sciences student.
Results
Two hundred and three students at McMaster University completed the survey. The sample included 72% women and 28% men. The mean age was 19.4 years. This sample represents a population of young adults who the previous literature would suggest are most likely to have regular health care since they are affluent (FAS greater than 6.7 ∓ 1.4). This group is also motivated in health education as 83.3% knew about the HPV vaccine and 76.4% could define the purpose of a PAP smear. Both male and female students were more likely to consult their family doctor about sexual health than their family. More than half of sexually active females have a family doctor, 82.1% of which visit them regularly. Sexually active women visit more regularly than sexually inactive women (p ≤ 0.01). The majority (66%) are comfortable discussing sexual health with their family doctor, yet only 62.5% of women have had this discussion. 57% of sexually active women and less that 1% of non-sexually active women had had a PAP smear or a pelvic exam.
Conclusion
These affluent and well educated students do not appear to be able to apply their knowledge of HPV and PAP smears to their own sexual health. Thus they require access to tools that help motivate university students to personalize information and make important health decisions.
Keywords
Introduction
Cervical cancer is the second leading cause of cancer in women worldwide. 17 In Canada, about 1,300 women will be diagnosed with cervical cancer each year. Cervical cancer affects relatively young women compared with other cancers. It affects women in their reproductive years at a time when they have young families or are still desirous of childbearing. In Canada, about 1,300 women will be diagnosed with cervical cancer each year, and 940 Canadian women aged 20-44 died from cervical cancer. 9 Half of the Canadian cases of cervical cancer occur in women who have not had regular Papanicolaou (PAP) smear screening. Currently in Canada, PAP smear screening is the gold standard method for detecting preinvasive cervical disease. Without screening, the cancer usually present in advanced stages when cure rates are low. Clinical guidelines for those under 20 years indicate that those who are sexually active should be seen within 3 years of first intercourse or at age 18 for a PAP smear; however, the actual rates of pelvic screening for young women are unknown.
Oncogenic HPV is the causative agent in cervical cancer. Almost all women will have an HPV infection at some point in their lives. Collins showed that 50% of women have evidence of an HPV infection within the first 3 years of sexual debut. 11 Unlike other STIs, all forms of sexual contact spread HPV and there is mixed evidence as to whether condoms provide protection. 8 In fact, computer simulation studies at McGill University suggest that it averages 11 sexual acts to acquire HPV in comparison to 100 sexual acts to acquire Herpes Simplex virus. 6 For HPV infections, 80%-90% are usually cleared by the immune system with two years of infection. 21 Persistent HPV infections are of the same oncogenic HPV type seen over time and are more likely to lead to genital warts and dysplasia. 22 Young women (peak time: 20-24 years old) 7 and men (peak time: 25-29 years old) 25 are most at risk of infection and the younger a person starts sexual contact, the more likely they are to have a persistent HPV infection.
The recent release of the HPV vaccine shows promise in helping decrease the incidence of cervical cancer in Ontario women. One concern regarding the vaccine involves coverage. 4 In Ontario, it appears that there was only 53% uptake of the first dose and there is no information regarding the second and third doses. 4 Another concern is the longevity of the vaccine and the fact that the current vaccine only prevents against 70% of the cancer causing HPV types. Thus regular PAP smears continue to be very important. 21
We undertook a cross-sectional study of highly motivated, university students interested in a health professional career concerning their knowledge of HPV prevention using vaccines and screening by PAP smears and how this influenced their health seeking attitudes and behaviors.
Methods
Sample
The sample from which the population was drawn includes all undergraduate male and female students in the Bachelor of Health Sciences (Honours) and Bachelor of Science (Nursing) Programs at McMaster University.
Survey and Data Collection
Using an online questionnaire, we measured the students' knowledge of human papillomavirus (HPV), willingness to receive the HPV vaccine, willingness to attend regular PAP smears as well as their attitudes and opinions towards the vaccine.
To gather our information, we developed male and female questionnaires that would be delivered online through Survey Monkey™. The questionnaire components were as follows:
The questionnaire was pilot tested with ten women and men for readability and feasibility. Revisions were made to improve appropriate language choice based on their feedback. The final male (30 questions) and female (38 questions) version of the questionnaires and the consent form were made available online through Survey Monkey™. Questionnaires were collected using a variety of methods; in-class; at a booth to publicize HPV awareness; and, a link to the questionnaire was posted in electronic message board for the health sciences and nursing students. Ethics approval for this study was obtained through the research ethics board at McMaster University, Hamilton, Ontario, Canada.
Demographic and health behavior.

The data was exported and analyzed using SPSS 17. Analysis included frequency tables, t-tests, Pearson correlations and cross tabs.
Results
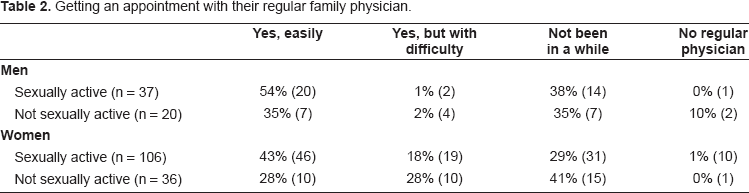
Completed questionnaires were submitted by 203 students, 146 women (72%) and 57 men (28%). The mean age was 19.4 years. Socioeconomic status was assessed using the Family Affluence Scale (FAS). The Canadian average FAS score is 5.7; our sample mean was 6.7 (∓1.4) (Table 2). Ninety-five percent of the students were non-smokers. Seventy-three percent of women (n = 106) and 65% (n = 37) of men were sexually active and at risk for exposure to HPV.
Getting an appointment with their regular family physician.
Comfort level and interaction with the family doctor concerning sexual activity.

Knowledge
The average knowledge score did not differ significantly between the men and women. The average molecular biology knowledge score was 54.8% for men and 51.3% for women. The behavioral knowledge scores were much higher (66% for men and 70% for women). There was a very low correlation between the molecular biology knowledge scores and the behavioral knowledge scores (r = 0.2). This may mean that students' knowledge of the mechanism of HPV does not translate to understanding the behaviors that puts one at risk for cervical cancer.
Advice seeking for sexual health
Students were asked to rate “who they would most likely go to for advice about their sexual health” on a scale of 1 to 6 where one indicates they were very unlikely to go and six indicates that the students were highly likely to go to for advice. Figures 1 and 2 show that the university students highest rated preference for sexual health advice were the Internet (males = 5.1 females = 5.2), and the family doctor (males = 5.7 females = 5.0). Men who were sexually active were more likely to value in person contacts (such as their family physician, school health clinic, friends and the public health clinic) when compared to those men who were not sexually active (Fig. 2). Women who are sexually active also were more likely to seek advice from in person sources (i.e. friends, school health clinic and public health clinic), but the differences between those who were not sexually active are less pronounced (Fig. 1).
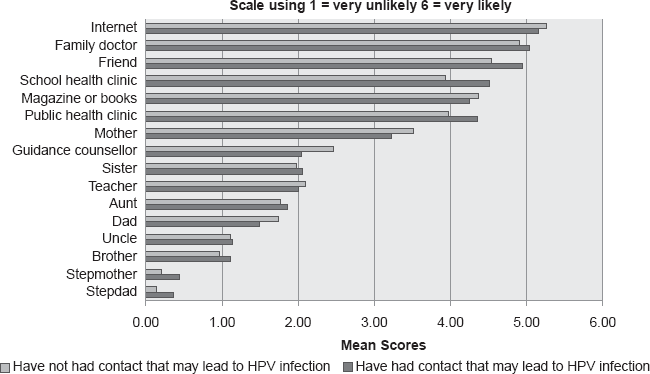
Females “Who would you most likely go to for advice about your sexual health?”
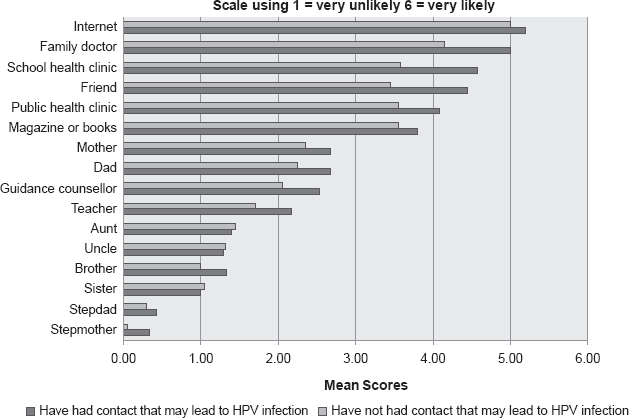
Males “Who would you most likely go to for advice about your sexual health?”
Access to a family physician and their comfort with their sexual health
Sexually active women (43%) and men (54%) were much more likely to indicate that they had a regular family physician they could easily get an appointment with compared to their non-sexually active counterparts (men = 35% women = 28%). More sexually active women than sexually active men had difficulty in getting an appointment with their family doctor. There were approximately equal rates of men and women who had not been to their family physician in a while and those reporting that they were without a family physician (Table 2).
Sexually active students report being comfortable discussing their sexual behaviour with their family physicians (men = 76% women = 80%) when compared to non-sexually active students (men = 35% women = 55%). Women were twice as likely to recall being asked about their sexual behavior by their family physicians than men whether they were sexually active or not. Both male and female students who were not currently sexually active were less comfortable compared to their sexually active peers discussing their sexuality with their family doctors (men
There were high rates of having heard about the HPV vaccine among women (86.2%) and men (80%). Of the women, 32.6% would be interested in talking to the family doctor about the vaccine and 5% had already received it. All of the women knew what a PAP smear was but only 73.7% of men did. Of the 75% of women who were sexually active, 32.4% had had a pelvic exam and 26.8% were aware of having had a PAP smear. 32% of all women (57% of sexually active women and less than 1% of non-sexually active women) reported having a PAP smear or pelvic exam. Figure 3 shows that all of the women reported having negative reactions to a pelvic exam. When comparing women who have never had a pelvic exam, they describe considerably stronger negative feelings than those who report a previous pelvic exam. Of the options offered on the survey to describe potential negative feelings about pelvic exams, all but one of the negative emotions were endorsed to a higher degree in those women who did not report a previous pelvic exam and these difference were statistically significant (p ≤ 0.00 for these comparisons; NS for “afraid”). Figure 4 shows the simple steps women felt would make the pelvic exam a better experience (like explaining what was happening). Women who have not previously reported having a pelvic exam are more likely to want a person they know present in the room with them compared to those who previously report having a pelvic exam.

Negative feelings towards having a pelvic exam (Females only): “Having a pelvic exam would be…”

Improvement to pelvic exam experience (Females only) “Having a pelvic exam would be a better experience for me when…”
Discussion
We have undertaken to address the knowledge about HPV in a well-educated, highly affluent young group of sexually active university students. We addressed their attitudes toward sexual health and behaviors in following through on having either/both a discussion of their sexuality with their physician, having the HPV vaccine, or a PAP smear. We identified high rates of having heard about the HPV vaccine (85%) and knowing what a PAP smear was (86%). There was also a high comfort level of talking with their physician about sexual health (74% in women and 60% in men). However, rates of following through with personal preventative health care were mediocre to poor (32% for PAP smear and 5% for HPV vaccination). Education in the virology of HPV is not a strong enough motivator for regular sexual health checkups.
The HPV vaccine is recommended to women 9 to 26 years of age. The vaccine is funded provincially for grade 8 girls in Ontario. The vaccine can be obtained in Ontario through family doctors or student health care clinics if you pay for it. Despite this, only 5% of university health sciences women who were interested enough to participate in this survey had actually had the vaccine. Mitchell showed in 330 students from 4 faculties at the University of Toronto that after reading an educational segment of the NACI guidelines the intention rates rose significantly to speak with a physician about the vaccine (48%), and get the vaccine (28%). 20 These high intention rates have been reported in the literature.18,19,23 These studies support Blumenthal's work in high school girls. 3 He hypothesizes that knowledge and acceptance of risks are the keys to improving vaccination rates. 3 In contrast, our work shows that despite in-depth knowledge about HPV in a sexually active population of university students, only one in three would be interested in having a discussion with their family doctor about primary prevention and very low rates (5%) actually had the vaccine. Prior work in 240 female nursing students also showed this disconnect. Despite high rates of high-risk sexual behaviors, they had a low perceived susceptibility and low perceived seriousness regarding HPV and cervical cancer. 13 Clearly in our sample where knowledge and finances are not a barrier to obtaining the vaccine, there is a need to identify the reasons behind the lack of vaccine uptake.
The SOGC HPV clinical guidelines indicate that, “failure to undergo screening may be due to such reasons as lack of knowledge, lack of access and failure of the clinician to offer screening”. 8 In our population the knowledge was excellent and access to family physicians was quite good. We did show that there was a low rate of discussion of sexual behaviour with physicians that was more marked in male students. In our sample of women, only one third of sexually active women had undergone a PAP smear. We cannot comment on whether the PAP smear had been offered but was declined. This rate is much lower than the 72% reported in the 1996-1997 National Population Health Survey. 2 PAP smear rates in this population vary from 70% in some studies5,14 to rates more in keeping with our population of 18% 22 to 40%. 15 There is a need to identify barriers to obtaining PAP smears in this population of young women and determine acceptable opportunities to improve screening rates.
The strengths of this study are that it is the first cross-sectional study in a highly educated group of university students interested in pursuing a career in health care that shows a clear disconnect between knowledge and self care. It was completed within a short period of time. The limitations include we did not conduct a full model assessment addressing barriers to following through on provincially endorsed preventative modalities (i.e. HPV vaccine and PAP smears). Parameters that could be measured include health belief, issues related to cost, and invincibility.
Conclusion
This study clearly shows that knowledge about the causes of cervical cancer is not enough to motivate sexually active students interested in a profession in health care toward cervical cancer prevention practices. Although there is a high comfort level in discussing sexual health with the family doctor, in this group of students there was a mediocre follow through with primary or secondary prevention strategies. Assessing barriers to prevention strategies is one direction for future research. Alternatively, work involving identification and implementation of successful motivating factors is clearly needed.
Disclosures
The authors report no conflicts of interest.