
Abstract
Lenalidomide is an oral immunomodulatory drug that has helped improve outcomes in multiple myeloma (MM) patients. Combination lenalidomide and dexamethasone (Len+Dex) has been shown to increase response rates and prolong survival compared with dexamethasone alone in patients with relapsed or refractory MM (RRMM). Clinical benefit may be greatest when Len+Dex is given at first relapse, and continued treatment appears to provide greater depth of response and improved survival outcomes. The most common adverse events associated with Len+Dex are cytopenias, which are predictable and manageable. Len+Dex is associated with an increased risk of venous thromboembolism, which necessitates adequate prophylaxis. The risk of second primary malignancies does not appear to be increased in patients with RRMM treated with lenalidomide-based therapy. Here we review the safety and efficacy of Len+Dex in RRMM, and provide an overview of data from Spain on the use of Len+Dex in RRMM.
Introduction
Multiple myeloma (MM) is one of the most common hematological malignancies.1,2 According to the European Network of Cancer Registries, MM affects approximately 21,500 people each year in Europe, with 15,000 dying from MM annually. In the USA, an estimated 20,200 people are diagnosed with MM each year, and approximately 10,700 die from MM annually. 1 The disease primarily affects older adults (median age at diagnosis is approximately 70 years), and is characterized by clonal proliferation of malignant plasma cells in the bone marrow, monoclonal protein in the blood or urine, and associated organ dysfunction. 3
The goals of therapy for MM are to prolong overall survival (OS) by achieving durable remissions and to control disease symptoms. 3 Intensive chemotherapy with autologous stem-cell transplantation (ASCT) is an effective treatment option, but few patients are eligible for this procedure due to advanced age and comorbidity. Although long-term disease control is possible, virtually all patients eventually relapse. 4
The introduction of the novel therapies lenalidomide, thalidomide, and bortezomib has had a positive impact on survival outcomes in patients with MM.5–7 Patients treated with one or more of these agents were found to have significantly longer survival than those who were never exposed to these agents. 5 Lenalidomide, thalidomide, and bortezomib now have established roles in the management of patients with MM, although ongoing studies continue to refine the optimal use of these agents with regard to combination, sequence, and duration of therapy.
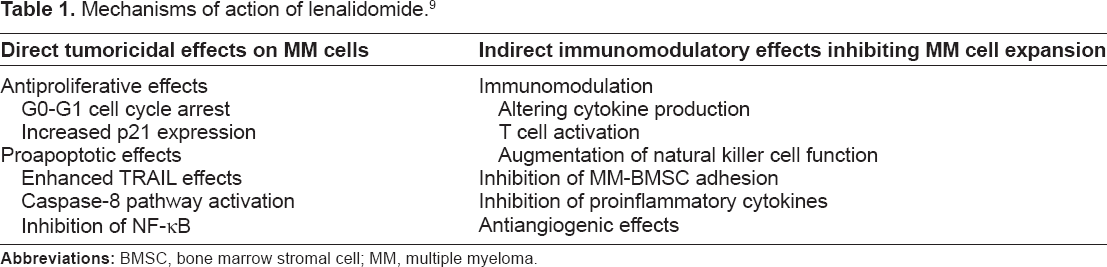
Lenalidomide is an orally administered immunomodulatory drug that is structurally related to thalidomide. It was originally developed to overcome some of the side effects associated with thalidomide and provide more potent inhibition of tumor necrosis factor-alpha. 8 The mechanism of action of lenalidomide in MM is complex and involves both direct tumoricidal effects on MM cells and indirect effects on the bone marrow microenvironment and host immunity; together, these effects inhibit MM cell growth and survival (Table 1). 9 Specifically, lenalidomide has been shown to prevent growth and induce apoptosis in MM cells,10–12 interfere with MM cell adhesion to bone marrow stromal cells, 13 inhibit angiogenesis, 14 and boost host immunity against MM cells.15–18 The activity of lenalidomide in MM is attributed to its ability to reduce the MM cell burden via its antiproliferative and proapoptotic effects while suppressing residual MM cell growth via its effects on the bone marrow microenvironment and immunomodulatory effects. The unique effects of lenalidomide may explain the additive antimyeloma effects observed when lenalidomide is combined with other active agents, such as dexamethasone, in vitro: for example, the caspase-8-mediated apoptosis induced by lenalidomide may complement the caspase-9-mediated signaling induced by dexamethasone, resulting in greater myeloma cell death; however, dexamethasone appears to antagonize the immuno-stimulatory effects of lenalidomide.10,12,19
Mechanisms of action of lenalidomide. 9
Early clinical studies indicated that lenalidomide is active in patients with relapsed or refractory MM (RRMM), including those who had received prior thalidomide. 13 Notably, adverse events commonly associated with thalidomide, such as somnolence, constipation, and neuropathy, were not observed. The addition of dexamethasone to lenalidomide treatment was found to further increase response rates. 20 In two phase III placebo-controlled studies in patients with RRMM, the combination of lenalidomide plus dexamethasone (Len+Dex) significantly increased response rates and prolonged progression-free survival (PFS) and OS, compared with dexamethasone alone.21–23 The Len+Dex regimen was effective regardless of the type of prior therapy received24,25 and was effective in patients with renal impairment, provided that appropriate dose modifications are made. 26 Moreover, Len+Dex was found to be most effective when given at first relapse. 27 Continued treatment led to greater depth of response and improved survival outcomes.28,29 These data led to the approval of Len+Dex for the treatment of patients with MM who have received at least 1 prior therapy. 30
As clinical experience with lenalidomide increases, more is learned about its long-term safety and efficacy in MM. For example, recent findings from Spain suggest that lenalidomide is effective in MM patients with extramedullary plasmacytomas.31,32 The purpose of this article is to review the current understanding of the safety and efficacy of lenalidomide-based therapy in the treatment of patients with RRMM, with a special focus on the Spanish experience (Alegre A, Oriol-Rocafiguera A, García-Laraña J, et al. Safety, efficacy, and quality-of-life of lenalidomide plus dexamethasone for the treatment of relapsed or refractory multiple myeloma: the Spanish experience. Submitted to Leukemia and Lymphoma, 2011).31,33,34
Efficacy
The efficacy and safety of Len+Dex in RRMM was demonstrated in two pivotal phase III trials (MM-009 and MM-010).21–23 Both studies compared Len+Dex with placebo plus dexamethasone in patients who had received at least one prior therapy. Lenalidomide was given orally at a dose of 25 mg per day on days 1–21 of each 28-day cycle until disease progression. In both treatment groups, dexamethasone was given orally at a dose of 40 mg per day on days 1–4, 9–12, and 17–20 for the first four cycles. After the fourth cycle, dexamethasone was given on days 1–4 only of each cycle.
Both studies indicated that Len+Dex significantly improved response rates and time to progression compared with placebo plus dexamethasone.21,22 These results were confirmed in a pooled analysis of data from both studies, which showed significant differences in response rates (61% vs. 22%; P < 0.001) and TTP (13.4 months vs. 4.6 months; P < 0.001), favoring Len+Dex. 23 With a median follow-up of 48 months for surviving patients, median PFS was significantly longer with Len+Dex (11.1 months vs. 4.6 months; P < 0.001) (Fig. 1A) and median OS was 38.0 months with Len+Dex and 31.6 months with placebo plus dexamethasone (P = 0.045) (Fig. 1B). 23 The significant improvement in OS is notable because nearly half of the 351 patients assigned to placebo plus dexamethasone received lenalidomide-based therapy at the time of progression or unblinding of the study.

Progression-free survival (
Several prespecified subanalyses of MM-009 and MM-010 data were performed to further define the activity of Len+Dex. These analyses confirmed that clinical benefit was observed regardless of whether patients had previously received thalidomide therapy. 24 Similarly, prior high-dose chemotherapy with ASCT did not affect the benefit of Len+Dex at relapse. 25 The analyses also showed that Len+Dex was most effective when given at first relapse, rather than as a later line of therapy. 27 The quality of response to Len+Dex improved over time, with 38% patients who had an initial documented partial response (PR) by cycle 6 achieving complete response (CR) with continuous treatment. Furthermore, the achievement of CR or very good PR (VGPR) as best response was linked to improved OS, irrespective of when CR or VGPR was achieved. 29 It was also shown that continuing treatment until disease progression appears to improve OS. 28 The promising effects of long-term lenalidomide therapy when used as maintenance therapy in patients with newly diagnosed MM35–37 provide further support for prolonged use of lenalidomide-based therapy in RRMM.
Other studies conducted in a daily practice setting have provided further evidence of the safety and efficacy of Len+Dex in RRMM. Two studies recently evaluated Len+Dex when given through compassionate use programs in the Netherlands 38 and Spain. 33 In the Dutch Compassionate Use Program, 114 patients with RRMM received Len+Dex. 38 Patients had received a median of 3 prior lines of therapy, and 91% had received prior thalidomide. The response rate was 69%, including a CR rate of 6%. Notably, response was not influenced by prior thalidomide or bortezomib therapy. Median time to progression and median OS were 9 and 22 months, respectively. Grade 3 or higher hematologic adverse events were reported in 37% of patients, and the incidence of venous thromboembolism (VTE) was low (5%) with appropriate thromboprophylaxis. Similar results were found in the Spanish Compassionate Use Registry, which is discussed in detail in the following sections. Results from the Spanish cohort of the expanded access program (MM-018) on the long-term use of Len+Dex are also discussed (Alegre A, Oriol-Roca-figuera A, García-Laraña J, et al. Safety, efficacy, and quality-of-life of lenalidomide plus dexamethasone for the treatment of relapsed or refractory multiple myeloma: the Spanish experience. Submitted to Leukemia and Lymphoma, 2011). 34
Safety
The primary adverse events associated with Len+Dex in RRMM are cytopenias, VTE, rash, fatigue, and muscle cramps. 23 In phase III trials, Len+Dex was associated with a significantly higher incidence of severe neutropenia, thrombocytopenia, anemia, and VTE compared with dexamethasone alone (Fig. 2). 23 Peripheral neuropathy, a common and problematic side effect of thalidomide and bortezomib, is rarely observed with lenalidomide.23,39
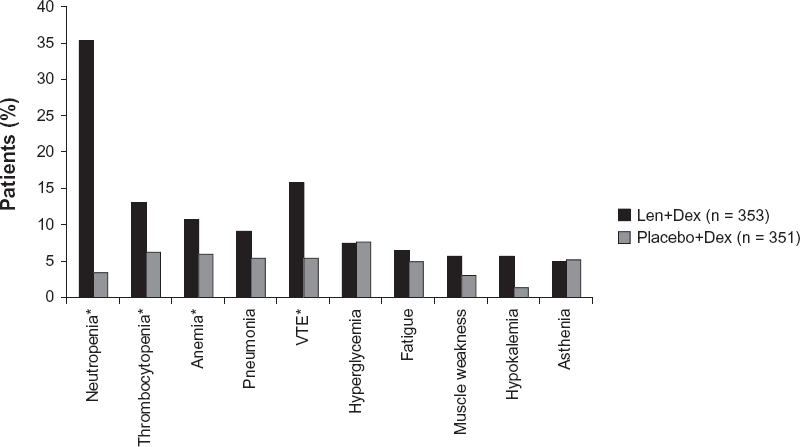
Grade 3 or higher adverse events occurring in more than 5% of patients with relapsed or refractory multiple myeloma treated with combination lenalidomide and dexamethasone (Len+Dex) or placebo plus dexamethasone (Placebo+Dex).
Lenalidomide is not nephrotoxic, but it is excreted renally.30,40 Impaired renal function can delay clearance, resulting in increased drug exposure. Consequently, lower doses of lenalidomide may provide sufficient drug exposure in patients with renal impairment, and dose reductions are recommended for these patients.30,40 Among the 353 patients who were treated with Len+Dex in the MM-009 and MM-010 studies, response rates were comparable in patients with mild or no renal impairment (creatinine clearance >60 ml/min; 64%), moderate renal impairment (30–60 ml/min; 56%) or severe renal impairment (<30 ml/min; 50%). 26 Moreover, renal function improved during Len+Dex treatment in 72% of patients who had moderate or severe renal impairment at study entry. PFS was similar in all groups according to renal function. Compared with patients with mild or no renal impairment, those with severe renal impairment were more likely to experience thrombocytopenia, to require lenalidomide dose reductions, and to have shorter OS.
Managing Myelosuppression
Neutropenia and thrombocytopenia are common in patients treated with Len+Dex but their occurrence is predictable and manageable.23,40,41 Guidelines on management of cytopenias during lenalidomide therapy have been developed.30,40 Generally, neutropenia and thrombocytopenia can be managed with a combination of growth factor support or platelet transfusions, and lenalidomide dose modifications or discontinuation.
Managing VTE risk
Like thalidomide, lenalidomide is associated with a low risk of VTE when given as monotherapy. 42 When combined with other agents, such as dexamethasone, however, the risk of VTE increases.42–44 The risk can be reduced by administering thromboprophylaxis. Patients treated with Len+Dex should, therefore, receive appropriate thromboprophylaxis based on their individual risk status.40,44 A recent randomized trial compared three forms of thromboprophylaxis (aspirin, fixed low-dose warfarin, or a low-molecular-weight heparin [LMWH]) in patients with MM treated with thalidomide. It showed that aspirin and warfarin were as effective as the LMWH in reducing the risk of VTE; in elderly patients, warfarin was less effective than the LMWH. 45
Second primary malignancies
Recently, concerns have been raised regarding the risk of second primary malignancy (SPM) following treatment with lenalidomide. Reports of increased risk of developing SPM have been generated from trials evaluating lenalidomide as first-line therapy or as maintenance therapy following ASCT in patients with newly diagnosed MM.37,46–48 In patients with RRMM, an increased risk of SPM has not been currently demonstrated.49,50 An analysis of pooled data from the MM-009 and MM-010 studies indicated that SPM incidence was low in both treatment groups, and similar to expected background incidence according to the US Surveillance, Epidemiology, and End Results (SEER) cancer registries. 49 A pooled analysis assessed data from 3839 patients treated with lenalidomide-based therapy in 11 clinical trials, including 313 patients (8%) who received lenalidomide for 24 months or more. 50 No significant increase in incidence rates of SPM were found compared with incidence rates reported in the SEER registries. Thus, at this time, an increased risk of SPM has not been demonstrated in patients with RRMM treated with lenalidomide-based therapy, even with long-term therapy. Ongoing studies will continue to help determine the risk of SPM.
The Spanish Experience
Spanish Compassionate Use Registry
Lenalidomide was approved for the treatment of patients with RRMM in Spain in January 2008. 33 Access to the drug prior to that time was possible through a compassionate use program for those patients with RRMM and no other treatment options. We conducted a nationwide cross-sectional retrospective study of 111 patients with RRMM who received lenalidomide through the Spanish Compassionate Use Registry. 33 Baseline characteristics are summarized in Table 2. 33 Patients had advanced disease (median disease duration 37.4 months [range, 4–200 months]) and had received a median of 3 prior lines of therapy (range, 1–8). Fourteen patients (12.6%) had renal failure, defined as creatinine levels greater than 177 μmol/L. Approximately 61% had multiple lytic lesions, 24% had extramedullary plasmacytomas, and 17% had cytogenetic abnormalities. Most patients (90%) had received prior bortezomib, 26% had received prior thalidomide, and 35% had undergone high-dose chemotherapy with ASCT.
Disease characteristics, prior therapy, and lenalidomide dose and schedule in 111 patients with relapsed or refractory multiple myeloma. 33

Defined as creatinine >177 μmol/L.
Approximately 90% of patients received Len+Dex. In 80% of patients, lenalidomide was administered according to the standard schedule: 25 mg per day for the first 3 weeks of each 4-week cycle. The remaining patients received less intensive doses and schedules. Among the 14 patients with renal failure at baseline, 5 received the standard schedule and 8 were given lenalidomide at a dose of 25 mg per day for 3 days per week for the first 3 weeks of each 4-week cycle; 1 patient received lenalidomide at a dose of 15 mg per day for the first 3 weeks of each 4-week cycle.
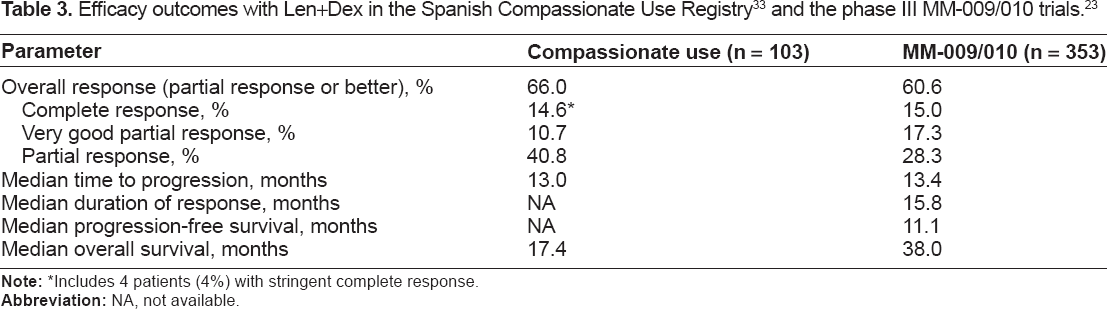
In this heavily pretreated group of patients, the overall response rate was 66%, which is comparable to results from phase III trials evaluating Len+Dex (Table 3). 23 Notably, the overall response rate was also high in patients with renal failure (54%), which is also comparable to findings from phase III trials, 26 although the depth of response was not as good as that achieved in the total population (Fig. 3). Overall, the median time-to-progression of 13.0 months was similar to that achieved in phase III trials, but the median OS of 17.4 months was lower than that achieved in phase III trials (38 months), which may reflect the more advanced condition of patients receiving treatment on a compassionate use basis. Adverse events consisted primarily of myelosuppression and were generally predictable and manageable. Most patients (87%) received some form of thromboprophylaxis, and the subsequent incidence of deep-vein thrombosis was low (<2%).
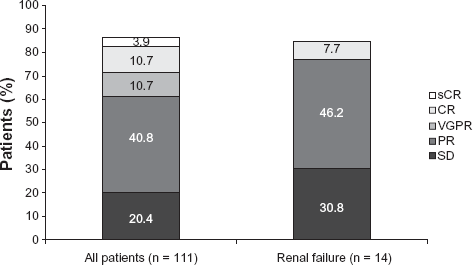
Response rates to lenalidomide-based therapy in patients with advanced and heavily pretreated relapsed or refractory multiple myeloma. Renal failure defined as creatinine >177 μmol/L. Data from Alegre et al. 33
Includes 4 patients (4%) with stringent complete response.
These data generally support the findings from the registrational phase III trials evaluating Len+Dex in patients with RRMM.21–23 The median survival time in our study was somewhat shorter than that reported in the phase III trials, which may reflect the more advanced disease state of patients who received lenalidomide on a compassionate use basis. The findings from the Spanish Compassionate Use Registry, therefore, complement the existing clinical trial data by providing further evidence of the efficacy and safety of lenalidomide when given outside the context of a clinical trial.
MM-018 Spanish cohort
Recently, data were presented on the Spanish cohort of patients who participated in an expanded access program for lenalidomide (MM-018) (Alegre A, Oriol-Rocafiguera A, García-Laraña J, et al. Safety, efficacy, and quality-of-life of lenalidomide plus dexamethasone for the treatment of relapsed or refractory multiple myeloma: the Spanish experience. Submitted to Leukemia and Lymphoma, 2011). 34 The MM-018 study was a multicenter, single-arm, open-label study that evaluated safety and quality of life in patients with RRMM treated with Len+Dex. 51 A total of 587 patients were enrolled in one of three geographic cohorts (Spain, UK/Ireland, or Austria/Australia). The Spanish cohort consisted of 63 patients with a median age of 62 years. Approximately half of the patients received 12 or more cycles of Len+Dex. The response rate was 78%, including a CR rate of 21%. The median duration of response was 18.4 months, and the depth of response appeared to improve with prolonged therapy.
The safety profile in the Spanish cohort was generally consistent with that observed in the total study population (Table 4)34,51 and reports from previous trials: the primary adverse events were myelosuppression and deep-vein thrombosis. Health-related quality of life was assessed at baseline and after 6 months of treatment using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for patients with cancer (EORTC QLQC30) and the EORTC QLQ for patients with myeloma (EORTC QLQ MY-20). While scores in the total study population indicated that quality of life was maintained during 24 weeks of treatment with Len+Dex, scores in the Spanish cohort revealed marked patient-reported improvement in nearly all EORTC QLQ C30 scales, including global quality of life, fatigue, pain, and emotional, physical and cognitive function. The EORTC QLQ MY-20 results showed a meaningful improvement in future perspective scores.

Plasmacytomas
Extramedullary disease does not respond to thalidomide,52,53 but some reports indicate that it is sensitive to bortezomib.54–56 There is evidence that Len+Dex is also active in patients with RRMM and plasmacytomas, including extramedullary plasmacytomas.31–33 In the Spanish Compassionate Use Registry, 8 of 24 patients (33%) with extramedullary plasmacytoma responded to lenalidomide-based therapy, including 4 patients (17%) who had a CR. 33 In a case report recently presented by García Pérez, 32 11 cycles of Len+Dex were given to a 62-year-old woman with RRMM who had developed a large extramedullary plasmacytoma. Reduction in plasmacytoma size was seen after the third cycle. The patient continues to receive lenalidomide monotherapy at a dose of 10 mg per day. Lastly, in a prospective study of 18 patients with extramedullary plasmacytomas, lenalidomide-based therapy was found to induce a response at extramedullary sites in 11 patients (61%), 31 including complete disappearance of extramedullary disease in 8 patients (44%). Notably, all 18 patients had received prior bortezomib, and all had relapsed (n = 12) or refractory disease (n = 6) following their last therapy. These findings suggest that lenalidomide may be more effective than thalidomide and at least as effective as bortezomib in the treatment of RRMM with extramedullary disease, although larger prospective studies are needed to confirm these preliminary results.
Summary
Len+Dex prolongs PFS and OS in RRMM and has become a standard treatment option for patients who have received at least 1 prior therapy. Evidence suggests that Len+Dex is beneficial regardless of prior thalidomide exposure or prior ASCT. Len+Dex may be most beneficial when given at first relapse. Continued treatment appears to be associated with greater depth of response resulting in improved survival outcomes. The primary adverse events associated with Len+Dex in RRMM are myelosuppression and VTE; other common adverse effects include rash, fatigue, and muscle cramps. Lenalidomide does not appear to cause or exacerbate peripheral neuropathy. The risk of SPM continues to be investigated, particularly in newly diagnosed patients. In patients with RRMM, lenalidomide-based therapy does not appear to be associated with an increased incidence of SPM; the risk of SPM, therefore, does not appear to outweigh the potential benefits of treatment. The Spanish experience with Len+Dex in RRMM supports the findings from large clinical trials indicating that Len+Dex is effective and has a predictable and manageable safety profile. Moreover, data from the Spanish Compassionate Use Registry suggest that Len+Dex can be given safely and effectively to heavily pretreated patients with very advanced disease in a daily practice setting.
Disclosures
Author(s) has/have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s), author(s) was/were required to supply signed patient consent prior to publication. Author(s) has/have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Dr. A. Alegre is member of the medical advisory board of Ortho Biotech and Celgene Spain.
Footnotes
Acknowledgements
The authors would like to thank all physicians and teams who referred patients with multiple myeloma to the Spanish lenalidomide studies. These studies are impossible without the voluntary participation of our patients. We want to thank these patients and their families for their collaboration. The authors received editorial support from Excerpta Medica in the preparation of this manuscript, which was funded by Celgene Corporation.