
Abstract
Triple negative breast cancer (TNBC) is a highly heterogeneous tumor. There is increasing evidence of the role of tumor lymphocytic immune infiltrates in this subtype of breast cancer. Robust levels of tumor infiltrating lymphocytes (TILs) have been associated with improved disease-free and overall survival rates in TNBC patients with and without any treatment. Recent efforts have been made to develop a standardized methodology for evaluating TILs. The presence of TILs in the breast tumor microenvironment can also predict responses not only to neoadjuvant but also to adjuvant chemotherapy treatments. High numbers of TILs correlate with increased pathological complete responses (pCR) in TNBC. TILs are prognostic and predictive of response to standard therapies; thus, the immune system appears to play an active role in a subgroup of breast cancer. There is an increasing interest in directly targeting the immune system as part of breast cancer therapy, mainly in patients with TNBC. New immune modulatory agents, including immune checkpoints inhibitors, have shown promising activity in a subgroup of metastatic TNBC. Increased programmed cell death protein 1 ligand (PD-L1) expression on the surface of TNBC provides the rationale for implementing therapeutic strategies targeting the PD-1/PD-L1 axis in TNBC. The programmed cell death protein 1 (PD-1) inhibitor pembrolizumab, and the PD-L1 inhibitor atezolizumab have shown promising results in clinical trials.
Keywords
Introduction
The immune system plays a key role in cancer progression. 1 The concept of cancer immunoediting 2 explores the hypothesis that cellular immunity promotes tumor growth and can also eradicate the disease. Although contradictory, this theory is based on the dual role of the immune system in promoting host protection against cancer and facilitating tumor escape from immune destruction. The three phases of immunoediting are elimination, equilibrium and escape. 2 Although they are initially rejected by the immune system, tumor cells that survive can persist in a state of dormancy and, after upregulating pro-survival pathways, express molecules that promote immune suppression and angiogenesis.
Proinflammatory type I immunity, which includes CD4 and CD8 T-helper lymphocytes, is the immune response needed to eliminate cancer. 3 The ability to suppress immunity is crucial to protect normal tissues from collateral damage during immune responses against any type of pathogen. The cells of both the innate (neutrophils, monocytes, macrophages, and a host of APC) and the adaptive (B and T lymphocytes) immune system work together to respond to any type of pathogens, including tumor antigens. 3 Innate immune cells are required by B and T cells in order for them to identify immunogenic proteins, thus the subsequent generation of adaptive immunity allows for the development of memory cells, which are lymphocytes that remain in lymph nodes. Most antigens present in breast cancer are self-proteins that can stimulate T cells and also induce a regulatory immune response. 3
Breast cancer is capable of stimulating the immune system. Furthermore, the intensity of tumoral immune response influences the effectiveness of cancer therapy, and is correlated with favorable clinical outcome in this disease. 4 Some breast tumors have substantial lymphocytic infiltration, and tumor-infiltrating lymphocytes (TILs) have been recently proposed as a surrogate marker of adaptive immune response.5–8 The interaction of the immune system with tumor cells in breast cancer appears to be associated with triple negative breast cancer (TNBC) and HER2–positive breast cancer, and they are thought to be more immunogenic than luminal A carcinomas.
There is an emerging concept that the response to chemotherapy is at least partly dependent on an immunological reaction against tumor cells that are dying during the chemotherapy. 1 The large genetic and epigenetic changes present in most cancer cells provide many tumor-associated-antigens that the immune host system can recognize, thereby requiring tumors to develop specific immune resistance mechanisms. 9 An important immune resistance mechanism involves immune check-points, which normally mediate immune tolerance and mitigate collateral tissue damage (as autoimmunity or response to pathogenic infection). 9
TILs have been reported to be positively associated with improved survival, 5 particularly in TNBC. Furthermore, it has been shown that 30% to 50% of all breast cancers have upregulated programmed cell death ligand 1 receptor (PD-L1) on the tumor cell surface. 10 Programmed cell death protein 1 (PD-1) is an immune check-point that limits T cell effector functions within tissues. When PD-L1 binds with PD-1, which is present on the surface of T cells, the lymphocytes become inactivated. By upregulating ligands for PD-1, cancer cells block antitumor immune responses in the tumor microenvironment. 9 In metastatic TNBC, clinical trials of monoclonal antibodies blocking immune checkpoint proteins PD-1 and PD-L1 have shown similar results in metastatic melanoma and non-small cell cancer. 11
The present mini-review article summarizes the most relevant concepts about the role of TILs in TNBC and the promising immune checkpoint inhibitors therapy, such as anti-PD-L1/PD-1.
Pathologic and molecular heterogeneity of TNBC
Triple negative breast cancers are characterized by immuno-histochemistry for the lack of expression of estrogen, progesterone and HER2 receptors. The vast majority of TNBCs are high-grade, invasive ductal carcinomas with relevant nuclear pleomorphism, high mitotic rates and lack of tubule formation. However, TNBC comprise a diverse group of cancers with different prognoses.
Gene expression profiling has characterized 5 intrinsic molecular subtypes of breast cancer, luminal A, luminal B, HER-2 enriched, basal-like and claudin-low, as well as a normal breast-like group.12,13 TN and basal-like are usually interchangeable terms, but that is not accurate. Within TNBCs, all the intrinsic molecular subtypes can be identified, although the vast majority falls into the basal-like subtype (an average of 86%). 14 In addition, a cluster analysis of 587 TNBC identified at least 6 TNBC subtypes displaying unique gene expression and ontologies, including 2 basal-like (BL1 and BL2), an immunomodulatory (IM), a mesenchymal (M), a mesenchymal stem-like (MSL), and a luminal androgen receptor (LAR) subtype (Table 1). 15 Another recent genomic analysis using DNA and RNA profiling of 198 TNBC tumors described 4 subtypes with prognostic significance: luminal androgen receptor (LAR), mesenchymal, basal-like immune-suppressed, and basal-like immune-activated. 16 However, no data are yet available regarding the prognostic impact of the intrinsic molecular subtypes defined by any gene-expression profiling within TN disease. 14 If the presence of TILs is associated mainly with immunomodulatory or basal-like immuno-activated TNBC subtypes is not known.
Subtypes of triple negative breast cancer (TNBC) based on analysis of gene expression profiles.

As a whole, TNBC is a heterogeneous subtype of breast cancer with a high propensity for systemic metastases and poor survival, but in the clinic, markedly different natural histories and response to therapy can be identified. It is clear that additional tumor specific information is needed to find more effective treatments.
Different biomarkers are present in TNBC, such as epidermal growth factor receptor (EGFR), vascular endothelial growth factor (VEG), cKIT and basal cytokeratins, heat shock protein 90 (HSP 90), or mutations in p53. Unfortunately, targeted therapy directed against these biomarkers has not shown significant improvement in outcome in TNBC. 17 Nevertheless, many basal-like tumors (a subgroup of TNBC) have evidence of a DNA repair deficiency caused by either the loss of gene BRCA1/2 or the loss of chromosome 5q. Inhibitors of poly (ADP-ribose) polymerase (PARP), agents that target tumors with defective DNA-damage repair may have a therapeutic role in this subgroup of TNBC patients. 17
Tumor-infiltrating lymphocytes in TNBC
The presence of lymphocytes in close tumor proximity has been used as a crude surrogate for immune responsiveness to tumor peptides. The origin of the breast cancer immune response can be mediated by T cells that are reactive to new peptides arising from cancer-specific mutations, called neoantigens, as described for melanoma. 18
Both intratumoral and stromal TILs can be assessed by hematoxylin and eosin-stained sections. The International TILS Working Group recently published a guideline to standardize TILs evaluation (Fig. 1). 19 These recommendations mainly propose to focus on stromal TILs and test their clinical impact as a continuous variable. 19 Tumors that have more than 50% lymphocytic infiltrate are called lymphocyte-predominant breast cancer (LPBC) and have the best prognosis. 3 Different percentages of LPBC in tumors have been reported (Table 2), at approximately 10%,6,7 or only 4.4% in one paper, 8 although in a recent trial an LPBC phenotype (in this case ≥60% TILs) was found in 28.3% of the 314 TN tumors and 20% of HER2–positive BC. 20 Another retrospective set of 897 TNBC patients showed a median percentage of 20% TILs and 21.9% LPBC. 21
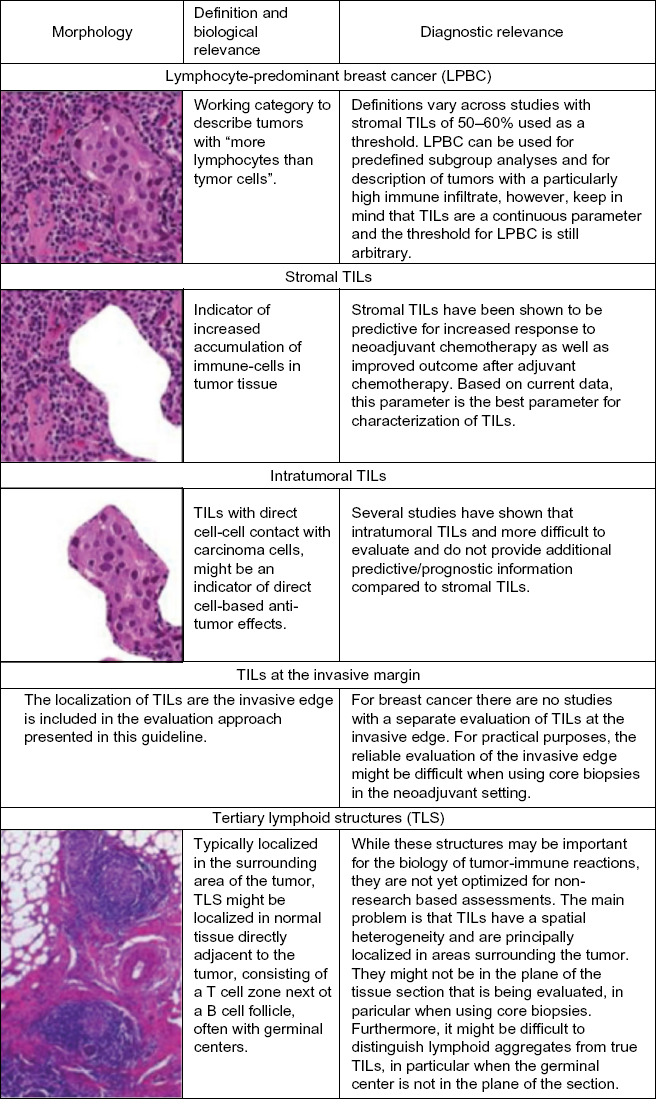
Morphology, definitions, biological and diagnostic relevance of different immune infiltrates seen in breast cancer.
Representative adjuvant trials including determination by hematoxylin-eosin of rich TILs and recent reported LPBC percentages in TNBC treated with neoadjuvant chemotherapy.

TILs as a prognostic factor
The presence of TILs has been associated with survival in breast cancer. 22 In TNBC without treatment the presence of TILs is correlated with improved overall survival,7,8 increased metastasis-free survival, 23 and decreased distant recurrence.7,8 Some of the most relevant studies including analysis of presence of TILs evaluated by hematoxylin – eosin in TN phenotype are summarized in Table 2.
In the Breast International Group (BIG) 02–98 trial only 256 TNBC from 2,009 lymph node positive breast cancer patients treated with anthracycline containing adjuvant chemotherapy showed that stromal TILs (sTILs) were related to outcome.
6
For every 10% increase in intratumoral and sTIL, there was a 17% and 15% reduced risk of relapse, respectively, and a 27% and 17% reduced risk of death regardless of chemotherapy type, respectively.
6
These results were verified in another retrospective analysis of 481 evaluable tumors from 2 phase III trials (Eastern Cooperative Oncology Group [ECOG] 2197 and ECOG 1199); for every 10% increase in sTIL, a 14% reduction of risk of recurrence (P = 0.02), an 18% reduction of risk of distant recurrence (P = 0.04) and a 19% reduction of risk of death (P = 0.01) were observed.
8
As seen above, there is a strong concordance between different studies showing that there is a 15–20% reduction in any recurrence and mortality for every 10% increments in rich TILs (Fig. 2).
8
Prognostic value of stromal tumor-infiltrating lymphocytes (sTILs) in TNBC. Kaplan-Meier curve of estimated overall survival (OS) for TNBC patients for sTIL (grouped as 0 [defined as 0% to 1%] V 10 [2% to 10%] V 20 to 40 [11% to 40%] V 50 to 80 [41% to 80%].
Other studies focus on the prognostic significance of CD8+ TILs tested by immunohistochemistry (usually >0) and/or FOXP3, given that most TILs in breast cancer are CD8+ T cells.24–27 In TNBC, as well as in HER2 positive BC, the presence of CD8 + T-cells within the tumor was associated with a 28% [95% confidence interval (CI) 16% to 38%] reduction in the hazard of breast cancer-specific mortality, and CD8+ T cells within the stroma were associated with a 21% (95% CI 7% to 33%) reduction in hazard. 26
TILs as a predictive factor
In TNBC, TILs can predict improved pathological complete response (pCR) to neoadjuvant chemotherapy (NACT).5,28,29 Higher pCR rates are seen after anthracycline and taxane-based NAC in TN and HER2–positive breast cancer with high levels of TILs.6–8 In the GeparSixto trial of anthracycline and taxane-based NACT exploring the effect of adding carboplatin, it was shown that increasing stromal TILs (sTILs) and LPBC predict pCR in TNBC, with a 74% pCR rate in LPBC TNBC vs 46% in non-LPBC in the carboplatin arm. 20
A recent meta-analysis showed that the detection of higher TIL numbers in pre-treatment biopsy was correlated with better pCR to NACT (OR = 3.93, 95% CI 3.26–4.73), and TILs also predicted higher pCR rates in TN (OR = 2.49, 95% CI 1.16–3.83). 29 For the TIL subset, higher levels of CD8+ and FOXP3+ T-lymphocytes in pre-treatment biopsies respectively predicted better pathological response to NACT, but all studies analyzed in this meta-analysis were retrospective; therefore, results must be interpreted cautiously. 29 Not only CD8+ but also PD-L1 and other immunological markers had positive correlations with stromal TILs and were significantly linked to increased pCR by chemotherapy. 20
The question of why TILs would be predictive of a better response to chemotherapy generates different hypotheses. 30 Chemotherapy may facilitate an antitumor immune response by decreasing tumor burden and also modifying the microenvironment, thus enabling a more effective immune response. In addition, some chemotherapeutic agents, such as anthracyclines, induce an immunogenic tumor cell death. 1 Chemotherapy can deplete myeloid-derived suppressor cells and regulatory T-cells that inhibit the immune antitumor response.1,31 Moreover, chemotherapy can generate somatic mutations that may produce new peptide antigens that appear different to the immune system, thus avoiding immune recognition.32,33 Unfortunately, currently TILs do not help to guide the selection of chemotherapy.
TILs as biomarkers of residual disease
Residual disease after NACT in TNBC is considered to be a poor prognostic factor. 34 NACT can increase TILS in the residual tumor, 4 and the presence of TILs in residual TNBC after NACT is also prognostic for better metastases-free and overall survival.35,36 Those patients with high TILs had the most favorable outcomes, even if they did not achieve a pCR. 35 The same has been reported regarding CD8+, as high CD8+ and a high CD8/FOXP3 ratio in residual tumors were powerful indicators of improved breast cancer specific survival. 37
In summary, approximately 20% of TNBC express robust TIL, which means greater than 50% lymphocytic infiltrate and are called LPBC. Several lines of evidence indicate that a greater number of TILs in the tumor stroma is associated with higher probability of cure in early stage TNBC, as well as a better chance of pCR after NACT treatments. Moreover, the high presence of TILs in residual disease after NACT seems to be related to more favorable outcome as expected.
Targeting the immune system in triple-negative breast cancer: potential role of immune checkpoint inhibitors
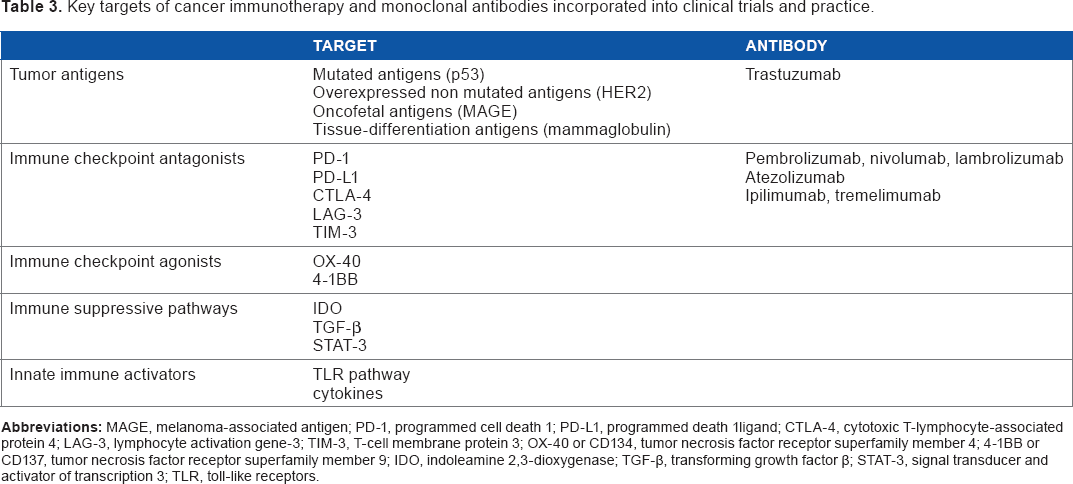
As seen above, TNBC is the subtype of breast cancer most associated with the presence of TIL, and not only TILs but also lymphoid aggregates can predict survival and response to standard breast therapies. The description of an immunomodulatory subtype of TNBC characterized by elevated expression of genes involved in antigen processing and T cell functions suggests a likely option for immunotherapy against this disease. 15 The key targets of cancer immunotherapy include immune checkpoint inhibitors or antagonists (see Table 3), as immune checkpoint antagonists of the PD-1/PD-L1 axis and CTLA4 (Fig. 3, from Drake 2014). 38
Key targets of cancer immunotherapy and monoclonal antibodies incorporated into clinical trials and practice.

Immune checkpoint blockade. This approach of immunotherapy is exemplified by antibodies against CTLA-4 (ipilimumab, tremilimumab), which have shown significant activity in melanoma and in non-small-cell lung cancer (NSCLC). A second major checkpoint is mediated by PD-1 on T cells or its ligand PDL1 on tumor cells and antigen-presenting cells. Reproduced with permission from C. G. Drake 2014. 38
Immune checkpoint proteins are present in normal tissues, cells of the innate immune system and lymphocytes. When a T-cell interacts through its immune checkpoint receptor protein like PD-L1, then this T-cell will be inactivated. 3 Immune checkpoint proteins are part of the host's natural defenses, which work to limit immune-destruction of normal tissues. A blockade with antibodies to PD-1 or PD-L1 results in the preferential activation of T-cells with specificity for the cancer, restoring anti-tumor T cell activity (Fig. 4, from Raufi). 39 In contrast to most approved monoclonal antibodies for cancer therapy, antibodies that block immune check-points do not target tumor cells directly, instead they target lymphocyte receptors or their ligands to enhance endogenous antitumor activity. 9
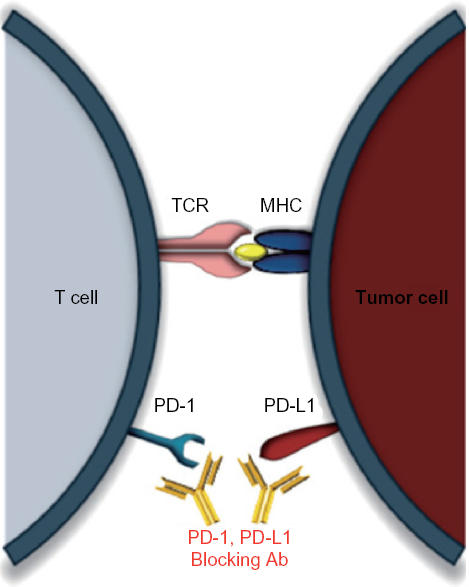
Immune checkpoint blockade of PD-1/PD-L1. PD-1, expressed on T lymphocytes, inhibits the action of T lymphocytes upon binding to its ligands PD-L1/2 (which are expressed on tumor cells). Blocking antibodies to either PD-1 or PD-L1 allows for T cell activation, enhancing anti-tumor effects. Reproduced with permission from Raufi, 2015. 39
Only melanoma and renal cell cancer were considered as immunogenic tumors. However, the results of a phase I study with an anti PD-1 monoclonal antibody, nivolumab, showed clinical responses in non-small cell lung cancers, suggesting that any tumor may respond to the immune checkpoint inhibition strategy. 45 Currently, three immune checkpoints have been approved by the Food and Drug Administration for the treatment of metastatic melanoma: one antibody against CTLA-4 (ipilimumab) and 2 against PD-1 (pembrolizumab and nivolumab). Nivolumab is also approved for the treatment of patients with metastatic squamous non-small cell lung cancer with progression on or after platinum-based chemotherapy and for advanced renal cell carcinoma. Agents that antagonize the PD-1 pathway have demonstrated not only durable clinical activity but also overall survival benefit in melanoma (pembrolizumab and nivolumab) and metastatic non-small cell carcinoma (nivolumab). 22 Multiple anti PD-1 and PD-L1 monoclonal antibodies are under evaluation in different digestive tumors, such as those for gastric cancer. 39
Pembrolizumab, a monoclonal anti PD-1, has been tested in a phase I clinical trial in metastatic PD-L1 positive TNBC. Pembrolizumab has showed preliminary overall responses of 18.5% in heavily pretreated TNBC. 40 In addition, one of the anti-PD-L1 antibodies, atezolizumab or MPDL3280A, has shown promising activity in TNBC. In a phase I study with atezolizumab, 21 evaluable patients with metastatic TNBC PD-L1 positive (37 PD-L1 positive from 54 initially tested patients) achieved an overall response rate by RECIST of 19%. 10 Three patients with PD-L1 positive TNBC experienced pseudoprogression, continued treatment and finally demonstrated responses. 41 Preliminary results of a combination of atezolizumab plus nab-paclitaxel chemotherapy in metastatic TNBC (mTNBC) have been reported, 42 and a phase III trial as first line therapy in untreated mTNBC cancer has been opened. Multiple additional immune-checkpoints receptors and their ligands are prime targets for blockade, as the cytotoxic T lymphocyte antigen-4 (CTLA-4). The monoclonal antibody tremelimumab, which inhibits the CTLA-4 pathway was evaluated in hormone-positive breast cancer and has shown activity. 22
The PD-1/PD-L1 pathway as a potential biomarker in triple-negative breast cancer.
As previously mentioned, PD-1 is an immune checkpoint transmembrane receptor protein that functions as a negative regulator of the immune system, limiting T-cell effector functions within the tumor. 9 PD-1 is expressed on many tumor-infiltrating CD8+ T-cells, as well as other cells of the immune system. By upregulating the ligands for PD-1 (either PD-L1 or PD-L2), tumor cells block antitumor immune responses in the tumor microenvironment, resulting in reduced proliferation of activated CD8+ T-cells. PD-L1 (also known as B7–H1 and CD274) expression has been reported in a variety of solid tumors, and a higher expression of PD-L1 correlates with better prognosis in lung cancer, colon carcinoma and melanoma. 43
The evaluation of PD-L1 protein expression is challenging due to a lack of specific and reproducible antibodies for use on formalin-fixed paraffin-embedded tissue. 44 A phase I trial of an anti-PD-1 antibody on various solid tumor types showed that the only patients with objective response to anti PD-1 therapy were those whose tumors expressed PD-L1. 45 In breast cancer, the reported rates of PD-L1 in carcinoma cells vary between studies, due to differences in sample size, sampling format (eg, tissue microarray versus whole section), and the method used to detect PD-L1 expression.45–50 PD-L1 protein expression has been observed between 15.8% and 30% in studies (Table 4), and in situ mRNA hybridization has been detected in PDL1 mRNA in 55% to 60% of tissue microarrays of primary breast cancers. 43
Different reported PDL1 expression in breast cancer, focus on TN subgroup.

One potential mechanism by which tumors can drive PD-L1 expression is by oncogenic signaling pathways, as loss of phosphatase and tensin homolog (PTEN). 47 PTEN is a negative regulator of the phosphatidylinositide 3–kinase (PI3K) pathway. PD-L1 mRNA levels were altered after either PTEN knockdown or PI3K inhibition, providing evidence of transcriptional regulation. 47 These authors suggest that agents targeting PI3K may enhance adaptive immune responses. 47 A second possibility is a positive feedback loop whereby inflammatory factors produced by immune cells in the tumor microenvironment causes tumor cells to increase cell surface expression of PD-L1, a possible mechanism through which cancer cells evade the adaptive immune response. 47 This paper suggests that therapeutic strategies targeting the PI3K pathway may enhance adaptive immune response against TNBC.
PD-L1 expression in tumor cells or its presence in the tumor microenvironment has been correlated with high levels of TILs and it has been positively associated with triple negative status in breast cancer.9,49 Furthermore, high PD-L1 and TILs have also been correlated with pCR after neoadjuvant chemotherapy, 9 and with improved clinical outcomes in TNBC. 49
In a recent paper, PD-L1 immunohistochemistry was performed by IHC on 161 primary TNBCs and assessed in the tumor and in immune cells in the stromal compartment. 50 PD-L1 expression was very common for TNBC in tumor cell membrane (64%), cytoplasm (80%) and stromal (93%) cellular compartments. While both PD-L1 expression and tumor-infiltrating lymphocytes were associated with a better outcome, only lymphovascular invasion and high tumor-infiltrating lymphocytes were independently prognostic for death due to breast cancer. 50
The potential value of PD-L1 could be its use as a target for PD-L1 axis-directed therapies, but PD-L1 expression status in tumor tissues does not seem to be an appropriate predictive biomarker to select patients for treatment with either anti-PD-1 or anti-PD-L1 antibodies, because PD-L1 is a dynamic marker that changes over time. 51 As opposed to mutated genes in cancers that permanently mark a tumor, the immune response is dynamic and changes rapidly. Moreover, in a phase I trial, approximately 10% of patients were deemed to be PD-L1 negative but did have clinical responses to anti PD-L1 therapy. 51
Recent findings have shown that TILs may be the primary predictor biomarker of response to immune checkpoint therapy. 52 Determination of TILs following the international WG guidelines 19 could consolidate its use in clinical practice. Conflicting results have been published regarding PD-L1 basal expression and response to anti PD-L1 therapy. In fact, clinical responses with anti-PD-1 have been observed in patients considered negative for PD-L1 expression in the tumor. 53 Another clinical trial with pembrolizumab reported that while expression of PD-L1 in pre-treatment tumor tissues correlated with clinical outcomes, the preexisting CD8 T cells in the invasive margin of the tumor were more predictive of clinical response to anti-PD-1. 52 Because of the constant evolution of an immune response, it is unlikely that a single immunologic biomarker can predict responses to any agent. 51
TILs can be used in designing novel clinical trials in neoadjuvant and adjuvant settings, but it is mainly for selecting those patients who most need novel therapeutic strategies. It is well known that there is an eventual relapse for most of patients with TNBC who do not achieve a pCR. Levels of TILs could identify a subgroup of patients with residual tumor cells and high TILs levels, who might benefit from finding immune checkpoint inhibitors that prevent tumor elimination.
Conclusion
Tumor infiltrating lymphocytes emerge as a robust prognostic biomarker of the host antitumor immune response in “immunogenic” breast cancer subtypes, especially triple-negative breast cancer. In TNBC, the increase of immune infiltrate with high levels of TILs predicts not only response to chemotherapy but also better survival.
Recent studies have focused on the role of the PD-1/PD-L1 axis in maintaining immunosuppression in the tumor environment. PD-L1, a ligand of PD-1 expressed by activated T-cells within the tumor microenvironment and on tumor cells, inhibits the local immune response. Biomarkers such as PD-1/PD-L1, but mainly TILs, could be potentially used to guide the selection of patients for therapeutic trials with T-cell activating antiPD-1/anti PD-L1 agents. Preliminary results of these trials in TNBC are encouraging.
Author Contributions
Conceived and designed: PGT. Analyzed the data: PGT. Wrote the first draft of the manuscript: PGT. Contributed to the writing of the manuscript: MLC. Agree with manuscript results and conclusions: PGT, MLC, IPF, YFP. Jointly developed the structure and arguments for the paper: PGT, MLC, IPF, YFP. Made critical revisions and approved final version: PGT, MLC, IPF, YFP. All authors reviewed and approved of the final manuscript.