
Abstract
Background:
Programmed cell death ligand 1 (PD-L1) expression with respect to genetic alternations has not been well established in non-small cell lung cancer (NSCLC), especially in the Asian population.
Methods:
We reviewed 1370 NSCLC patients from a prospectively maintained database. Immunohistochemistry was performed on tumor cells and tumor-infiltrating lymphocytes (TILs) using the VENTANA (SP142) anti-PD-L1 antibody. The tumor proportion score (TPS) cutoff values were set at ⩾1% and ⩾50%, and the immune proportion score (IPS) cutoff values were set at ⩾1% and ⩾10%.
Results:
In tumor cells, PD-L1 positivity was observed in 405 (29.6%), 122 (8.9%), and 27 (2.0%) patients with TPS cutoff values at ⩾1% and ⩾50%. Contrastingly, TILs of 1154 (84.2%) and 346 (25.3%) patients stained positive at IPS cutoff values of ⩾1% and ⩾50%, respectively. PD-L1 expression was more common in patients who were mutation-negative irrespective of the TPS cutoff values and tumor size. PD-L1 expression in tumor cells was less frequent in patients harboring EGFR mutations (18.8% TPS ⩾ 1% and 4.6% TPS ⩾ 50%). Conversely, PD-L1 expression was high in the presence of KRAS mutations (47.3% TPS ⩾ 1% and 22.5% TPS ⩾ 50%). Overall, KRAS, BRAF, PICK3A, MET mutations and ROS1 and RET translocations were more frequent, while EGFR and HER2 mutations and ALK translocations were less frequent compared with the overall PD-L1 expression levels. Although the difference between TILs among the PD-L1-positive cases was comparatively small, PD-L1 positivity was less prevalent in EGFR-mutated tumors and more common in those with KRAS mutations, ROS1 translocations, BRAF mutations, or MET mutations.
Conclusion:
Our study showed the heterogeneity in PD-L1 expression with respect to nine major oncogenic drivers in China. Future studies are warranted to further clarify the association between PD-L1 expression and driver mutations in NSCLC.
Keywords
Introduction
Cancer immunotherapy has recently emerged as a new paradigm for treatment of lung cancer. Immune checkpoint inhibitors targeting programmed cell death 1 (PD-1) or its ligand, programmed cell death ligand 1 (PD-L1), have demonstrated promising survival benefits in patients with non-small cell lung cancer (NSCLC).1–4 The increased expression of PD-L1 shown by immunohistochemistry has been reported to be associated with a better clinical response to PD-1/PD-L1 inhibitors.4,5 Detection of PD-L1 expression by immunohistochemistry has, therefore, been officially approved as a companion or complementary diagnostic test to develop immunohistochemistry assays and scoring criteria for the application of each anti-PD-1/PD-L1 agent. However, some patients with PD-L1-negative tumors were also found to respond to PD-1/PD-L1 drugs4–8; PD-L1 expression alone may therefore not be sufficient to predict response to blockage of the PD-1/PD-L1 axis. 9
NSCLC is characterized by driver mutation-defined molecular subsets. Alternations in genes like epidermal growth factor receptor (EGFR) have been consistently reported in NSCLC patients, especially those in Asia. 10 Preclinical data indicated that activation of the EGFR pathway might be involved in antitumor immunity, thus contributing to immune escape from PD-1/PD-L1 inhibitors. 11 Patients with EGFR mutations were found to respond more poorly to PD-1/PD-L1 inhibitors than those with wild-type EGFR.1,4,6,12,13 Meanwhile, another study indicated that patients with EGFR mutation-positive NSCLC were highly eligible for PD-1/PD-L1 immunotherapy. 14 Nonetheless, patients with PD-L1-positive tumors were noted to have higher sensitivity to EGFR inhibitors (gefitinib or erlotinib) in terms of the response rate (p = 0.01), time to progression (p < 0.0001), and survival (p = 0.09). 15 Hence, it is appealing to consider PD-L1 expression and the driver mutation status when selecting candidate therapies for patients.
The global multicenter study EXPRESS by Dietel et al. has shown the relationship between PD-L1 expression and molecular biomarkers (including EGFR mutation and ALK translocation). 16 Although it is the largest real-world study to date to have evaluated PD-L1 tumor expression in advanced NSCLC, only a small portion of tumor sample came from Asia, and no samples were taken from the mainland China. Besides, it is worth noting that most of previous studies have focused on only one or a few driver mutations, like EGFR, KRAS, and/or ALK,17,18 and no consensus has yet been reached in view of the heterogeneity in PD-L1 immunohistochemistry assay and scoring criteria, oncogenic drivers analyzed, and ethnic difference.19,20
The present study was therefore carried out to further explore the association between PD-L1 expression and the mutation status of nine major cancer-related genes using Ventana SP142 antibody in a large cohort of Chinese NSCLC patients. The findings of our study may help to better understand the molecular association of PD-L1 expression in the Chinese population and thus shed light on the potential candidates for PD-L1 immunotherapy or targeted therapy.
Methods
Study populations
We established a prospective cohort of the NSCLC patients who underwent surgical resection or biopsy at the First Affiliated Hospital of Guangzhou Medical University (Guangzhou, China) between January 2014 and July 2018. All NSCLC cases were cytologically or pathologically confirmed. Patients were excluded if they had received previous treatment with neoadjuvant chemotherapy, radiotherapy, or EGFR-targeted therapy. Those who had inadequate tumor specimens (<20% tumor nuclei) for molecular analysis or had incomplete medical records were also excluded. Clinical data on age at surgery, sex, smoking status, tumor size, and histology were abstracted from the electronic medical records of the patients based on the LinkDoc database (LinkDoc Technology Co., Ltd., Beijing, China). The study protocol was approved by the Institutional Review Board, and informed consent was waived for this observational study.
PD-L1 immunohistochemistry assay
PD-L1 expression in tumor cells and tumor-infiltrating lymphocytes (TILs) was assessed by VENTANA PD-L1 immunohistochemistry assay (SP142, Roche, Basel, Switzerland) according to the manufacturer’s instruction. The signal was visualized using the OptiView Amplification Kit and OptiView DAB IHC Detection Kit (Roche). Two experienced pathologists were invited to evaluate the immunoreactivity of PD-L1. Discordant cases were reviewed by a third pathologist to achieve consensus. PD-L1 expression on tumor and immune cells was quantified as the tumor proportion score (TPS) and immune proportion score (IPS), respectively. The cutoff values were set at ⩾1% and ⩾50% for TPS, and at ⩾1% and ⩾10% for IPS.
Mutation tests
Genetic alternations were assessed by targeted next-generation sequencing (NGS) to cover critical mutations involving nine major drivers (EGFR, ALK, RAS, ROS1, RET, BRAF, PIK3CA, MET, and HER2) in NSCLC. 21 In brief, DNA was extracted and quantified by using the QIAamp DNA FFPE Tissue Kit (Qiagen, Hilden, Germany) and Qubit fluorometer (Thermo Fisher Scientific, Waltham, MA, USA) according to the manufacturers’ instructions. The products were then captured and sequenced on the Ion Proton Sequencer (Thermo Fisher Scientific). The data obtained were processed using a customized bioinformatics pipeline (Otype). Somatic alterations including single-nucleotide variations, short insertions or deletions, copy-number variations, and gene rearrangements were identified.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics 17.0 (SPSS, Chicago, IL, USA). The data were expressed as mean values ± standard deviations (SD) or frequencies and proportions, when appropriate. Statistical comparison of PD-L1 expression between the patients with and without genetic alternations was made using a chi-squared test. PD-L1 expression with respect to each driver mutation was analyzed. A p value of < 0.05 was considered statistically significant.
Results
Clinical and molecular characteristics of patients
A total of 1802 consecutive NSCLC patients in the prospective database was reviewed. Finally, 1370 patients with sufficient tissues for mutation testing and PD-L1 immunohistochemistry assay were included in the study. Among them, 739 (53.9%) patients were male and 678 (49.5%) were non-smokers. The mean patient age at the time of surgery was 59.2 years, and 81.8% of the patients were aged 50 years or older. The majority of patients had adenocarcinoma (86.5%) and small tumors, sized ⩽3 cm (61.8%). The clinicopathological and molecular characteristics of the patients are summarized in Table 1. Overall distribution of PD-L1 expression in TCs and TILs was presented in Figure 1.
Clinicopathological and molecular characteristics of patients.

NSCLC, non-small cell lung cancer; SD, standard deviation.

Overall distribution of PD-L1 expression in TCs and TILs.
Genetic alternations were found in 865 (63.1%) patients, including 649 EGFR mutations, 129 KRAS mutations, 35 ALK translocations, 15 ROS1 translocations, and 43 alterations of other genes (Table 1). PD-L1 positivity was observed in tumor cells of 405 (29.6%), 122 (8.9%), and 27 (2.0%) patients using the SP142 antibody with TPS cutoff values at ⩾1% and ⩾50%, respectively. On the other hand, TILs of 1154 (84.2%) and 346 (25.3%) patients stained positive at IPS cutoff values of ⩾1% and ⩾50%, respectively.
PD-L1 expression with respect to driver mutations in NSCLC
Overall, PD-L1 expression on the tumor cells was more common in patients who were mutation-negative, irrespective of the TPS cutoff value set (1% or 50%). As shown in Figure 2, over 36% of patients with wild-type mutation status for all nine oncogenic genes had a PD-L1 TPS of ⩾1 %, while only 25.4% of those with driver mutations had the same TPS (p < 0.001). When it comes to the TPS cutoff of ⩾50%, although several patients harboring EGFR mutations were PD-L1-positive, the proportion was still significantly higher in the wild-type group than in the group with driver mutations (TPS ⩾ 50%: 11.7% versus 7.3%, p = 0.005). As for PD-L1 expression in TILs, there was no significant difference between the wild-type and the mutation group with regard to IPS ⩾ 1% (86.5% versus 84.4%). Meanwhile, at IPS ⩾ 10%, many more patients were PD-L1-positive in the wild-type group (32.2% versus 21.3%, p < 0.001, Figure 2).

PD-L1 expression in tumor cells and tumor-infiltrating lymphocytes with respect to driver mutations in NSCLC patients (A) and those with small-sized tumors (⩽3 cm).
The heterogeneity among the different driver mutations was then further considered. As reported in Table 2, the PD-L1 expression of tumor cells was less frequent in patients harboring EGFR mutations (18.8% at TPS ⩾ 1% and 4.6% at TPS ⩾ 50%), especially those with EGFR 19del or EGFR L858R mutations, even at a high cutoff of 50%. Conversely, PD-L1 expression on tumor cells was notably higher in the presence of KRAS mutations (Figure 3). The PD-L1 positive rates were 47.3% at TPS ⩾ 1% and 22.5% at TPS ⩾ 50%. Overall, KRAS, BRAF, PICK3A, and MET mutations and ROS1eRET translocations were more frequent, while EGFR and HER2 mutations and ALK translocations were less frequent compared with the overall PD-L1 expression level. By contrast, no case harboring HER2 mutation was positively stained for PD-L1, even at the lower cutoff value of TPS ⩾ 1%.
PD-L1 expression with respect to driver mutations in NSCLC patients.

IPS, Immune proportion score; NSCLC, non-small cell lung cancer; PD-L1, programmed cell death ligand 1; TCs, Tumor cells; TILs, Tumor-infiltrating lymphocytes; TPS, Tumor proportion score.
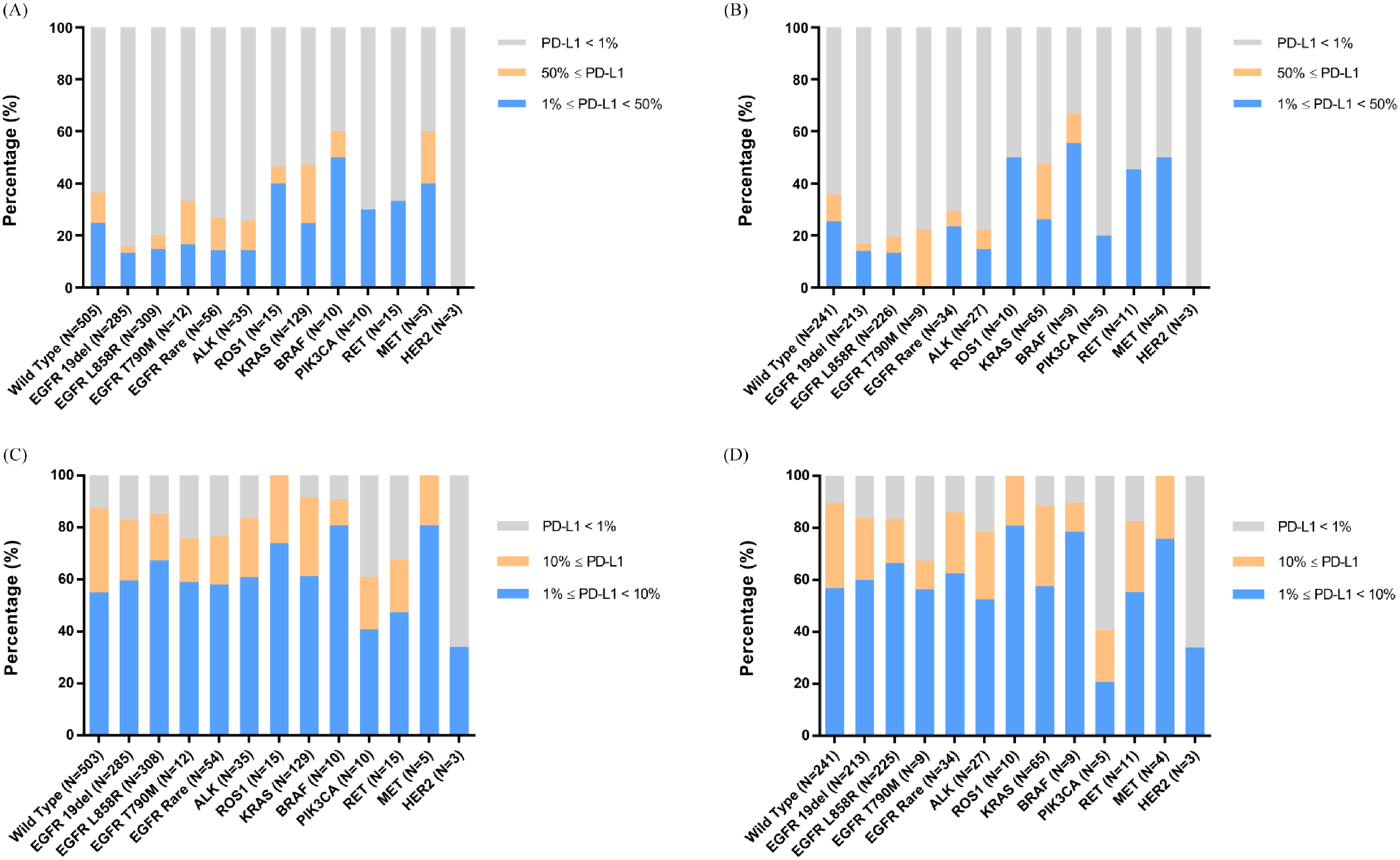
PD-L1 expression in tumor cells and tumor-infiltrating lymphocytes with respect to driver mutations in NSCLC patients (A and B) and those with small-sized tumors (⩽3 cm) (C and D).
However, the difference in the proportion of patients with PD-L1-expressing TILs was comparatively small, particularly at the cutoff of IPS
PD-L1 expression with respect to driver mutations in small-sized NSCLC (⩽3 cm)
We then limited the patients to those with small-sized tumors (⩽3 cm; n = 847) to further investigate the PD-L1 expression with respect to genetic alternations. A total of 847 patients with tumor size of 3 cm or less were analyzed. Overall, the expression of PD-L1 showed similar trends as in the entire population (Figure 2). In brief, PD-L1 expression was more common in the absence of any driver mutations. The presence of EGFR mutations remained correlated with lower rates of PD-L1 expression regardless of cutoff criteria. Moreover, KRAS mutations were correlated with higher PD-L1 expression rates (Figure 3 and Table S1). Nonetheless, genetic alternations in ROS1, BRAF, RET, and MET showed a trend toward increased PD-L1 expression at lower cutoff values, but not at higher values, possibly due to the small number of positive cases involved.
Discussion
In the present study, we explored the molecular associations of PD-L1 expression in tumor cells and associated immune cells with respect to nine major cancer-related genes in 1370 NSCLC patients in China. Using the SP142 antibody, we showed that PD-L1 expression was more common in the absence of any genetic alteration, irrespective of different immunohistochemistry scoring criteria applied (TPS of ⩾1% versus ⩾50%, and IPS of ⩾1% versus ⩾10%) and tumor size (small (⩽3 cm) versus whole population). Notably, PD-L1 expression was found to vary regarding different driver mutations. Patients harboring EGFR mutations were more likely to have lower rates of PD-L1 expression than those harboring none or other activating mutations, such as KRAS mutations. Meanwhile, patients with KRAS mutations showed comparatively higher rates of PD-L1 expression than those with the wild-type genotype or with alternations other than KRAS in both tumor cells and TILs. In addition, patients with alterations in genes like ROS1, BRAF, and MET showed an increased tendency towards PD-L1 expression. To the best of our knowledge, this is the first study that used a large number of NSCLC patients to investigate PD-L1 expression with respect to genetic alternations in China.
The association between PD-L1 expression and genetic alternations has been previously investigated, for example, the study EXPRESS by Dietel et al., which was the largest real-world study to evaluate PD-L1 tumor expression in advanced NSCLC, has showed the relationship between PD-L1 expression and molecular biomarkers (including EGFR mutation and ALK translocation), but tumor samples of patients in the Chinese mainland were not included. 16 PD-L1 expression was previously found to be more common in NSCLC patients carrying no mutation in EGFR, ALK, ROS1, or KRAS or being “pan-negative” (without EGFR, KRAS, HER2, and BRAF mutations and ALK, ROS1, and RET translocations).19,22 These results were consistent with our observations, indicating a significantly higher rate of PD-L1 expression with respect to wild-type genotype of nine major oncogenic drivers. As for the specific driver mutations, our study showed a lower rate of PD-L1 expression in the presence of EGFR mutations and a comparatively higher rate with respect to the KRAS mutations. Using the 22C3 antibody at TPS cutoff values of ⩾1% and ⩾50%, PD-L1 expression has been reported to correlate negatively with EGFR mutations and positively with e mutations, but not with ALK/e rearrangements or MET mutations in Hong Kong NSCLC patients. 23 On the other hand, PD-L1 positivity was correlated with wild-type EGFR, but not with KRAS mutations or ALK/ROS1 rearrangements in Korea lung adenocarcinoma patients in a study using SP142 antibody with the cutoff at ⩾5%. 24 Moreover, the presence of EGFR mutations was found to be associated with increased PD-L1 expression in Japanese NSCLC patients in a study using a rabbit polyclonal anti-PD-L1 antibody and a median histological score value of 30 as the cutoff point. 17 Similar results were observed in the Italian population in a study using the anti-PD-L1 antibody ab58810, with staining intensity of ⩾2 in more than 5% of tumor cells being considered as PD-L1 positive. 15 Furthermore, a study of Germany NSCLC patients showed that PD-L1 expression was associated with KRAS mutations but not with EGFR, BRAF, or PIK3CA mutation status when using the primary antibody 5H1 at a TPS cutoff of ⩾1%. 25 Other studies have reported no significant association between PD-L1 expression and genetic alternations in EGFR, KRAS, ALK, BRAF, ROS1, MET, BRAF, or HER2.26–30 These conflicting results may be partially explained by the variations in antibodies used for staining, the score criteria, oncogenic genes analyzed and their mutation rates among the different ethnicities, and the variations in study populations.
In view of the heterogeneity of PD-L1 immunohistochemistry assays and inconsistent results obtained, we have reviewed previous studies regarding molecular association of PD-L1 expression using Ventana SP142 antibody. The results in combination with the present study are summarized in Table 3. PD-L1 expression was found to be consistently lower in patients harboring EGFR mutations, while consistently higher in those harboring KRAS mutations, regardless of PD-L1 positivity threshold and study populations.24,31–37 These results suggest a negative correlation between PD-L1 expression and EGFR mutations, while a positive correlation with respect to KRAS mutations. Only one study investigated ALK alternations: PD-L1 was found to be positive in one (33.3%) of three ALK rearrangement cases at TPS ⩾ 1% and negative (0.0%) in all three cases at TPS ⩾ 50%. By contrast, in cases without ALK rearrangements, PD-L1 was positively stained in 27 (61.4%) and 11 (25.0%) out of 44 cases at a TPS cutoff of ⩾1% and ⩾50%, respectively. 37 These results were unlike the results observed in this study, which showed a similar rate of PD-L1 expression irrespective of ALK mutation status and cutoff criteria applied (29.7% wild-type ALK versus 25.7% ALK rearrangements at TPS ⩾ 1% and 8.9% wild-type ALK versus 11.4% ALK rearrangements at TPS ⩾ 50%; present study versus study by Krawczyk et al., respectively). A small sample size in their study and the ethnic difference may help to interpret this discrepancy. One thing worth noting is that PD-L1 expression seem to be comparatively higher in the Polish and United States (US) NSCLC patients than in the Chinese population.34,37 Meanwhile, our results were highly consistent with those from Japanese populations.31,32,36 Hence, there may be potential difference in PD-L1 expression with respect to ethnicity, as corroborated a previous study that suggested ethnicity as a significant factor affecting the prevalence of PD-L1 expression. 23
Summary of studies on molecular association of PD-L1 expression using the SP142 antibody.

ADC, adenocarcinoma; M, mutations; n, number; NSCLC, non-small cell lung cancer; PD-L1, programmed cell death ligand 1; Pts, patients; TPS, tumor proportion score; WT, wild type.
With regards to driver mutations other than those of EGFR, KRAS, or ALK, few studies have been carried out using the SP142 antibody. Our study showed a trend of increased PD-L1 expression with respect to ROS1 rearrangements and PIK3CA, RET, BRAF, and MET mutations in tumor cells. Meanwhile, PD-L1 was negative in all three cases harboring HER2 mutations, even at the lower TPS cutoff value of ⩾1%. Unfortunately, in view of the few positive cases involved in this study, it is difficult to conclude whether driver mutations of those less commonly investigated genes are correlated with PD-L1 in NSCLC patients. Nonetheless, our results were consistent in part with a previous study that showed a higher level of PD-L1 expression in patients harboring ROS1 rearrangements or MET mutations (using the 22C3 antibody, with a TPS cutoff at ⩾1% and ⩾50%), although the difference did not reach statistical significance. 23 In addition, that study also showed a similar level of PD-L1 expression regarding ALK rearrangements. 23 Nevertheless, our study did show a difference in PD-L1 expression with respect to different driver mutations and ethnic contexts.
Conclusion
In conclusion, our study reflects the real-world association of PD-L1 expression with driver mutations in nine major cancer-related genes in a large sample of NSCLC patients in China. Expression of PD-L1 was found to be more common in patients harboring no driver mutations and to vary with different oncogenic drivers. Overall, KRAS, BRAF, PICK3A, and MET mutations and ROS1 and RET translocations were more frequent, while EGFR and HER2 mutations and ALK translocations were less frequent compared with overall PD-L1 expression levels. Future studies are warranted to further clarify the association between PD-L1 expression and driver mutations in NSCLC.
Supplemental Material
Supplementary_Data_2 – Supplemental material for PD-L1 expression with respect to driver mutations in non-small cell lung cancer in an Asian population: a large study of 1370 cases in China
Supplemental material, Supplementary_Data_2 for PD-L1 expression with respect to driver mutations in non-small cell lung cancer in an Asian population: a large study of 1370 cases in China by Caichen Li, Jun Liu, Zhanhong Xie, Feng Zhu, Bo Cheng, Hengrui Liang, Jianfu Li, Shan Xiong, Zisheng Chen, Zhichao Liu, Yi Zhao, Limin Ou, Ran Zhong, Wei Wang, Jun Huang, Jinyun Sun, Chunya Zhang, Landong Weng, Jianxing He, Wenhua Liang and Zhenkui Pan in Therapeutic Advances in Medical Oncology
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study database was developed by LinkDoc Technology Co. Ltd. (Beijing, China) and supported by the China National Science Foundation (Grant No. 81871893) and Key Project of Guangzhou Scientific Research Project (Grant No. 201804020030).
Research ethics and patient consent
The study protocol was approved by the Institutional Review Board of the First Affiliated Hospital of Guangzhou Medical University (approval number: KLS-17-03) and informed consent was waived for this observational study.
Supplemental material
Supplemental material for this article is available online.