
Abstract
Two cases of neck masses in adults are presented. In each case, imaging suggested diagnosis of a thyroid mass. Further investigation eventually found this to be at variance with the true pathology. These cases are published to illustrate the difficulties that can be encountered in delineating the organ of origin for certain neck tumours.
Case Reports
Case 1
A 29 year old male, with no significant past medical history, presented to his general practitioner after a lower respiratory tract infection. On examination a goitre was noted. Chest x-ray demonstrated a right upper mediastinal mass with marked tracheal deviation to the left (Fig. 1a). Computed tomography (CT) scan of the neck (Fig. 1b and 1d) was interpreted as an enlarged right lobe of the thyroid (80 × 52 × 44 mm) with retrosternal extension and also a suggestion of an enlarged left submandibular gland (Fig. 1c and 1d). Ultrasound scan confirmed the right neck mass and reported it as enlargement of the right lobe of the thyroid gland with heterogenous echogenicity consistent with a multinodular goiter and a normal left lobe (Fig. 1e). Ultrasound guided fine needle aspiration (FNA) showed features consistent with multinodular goitre.
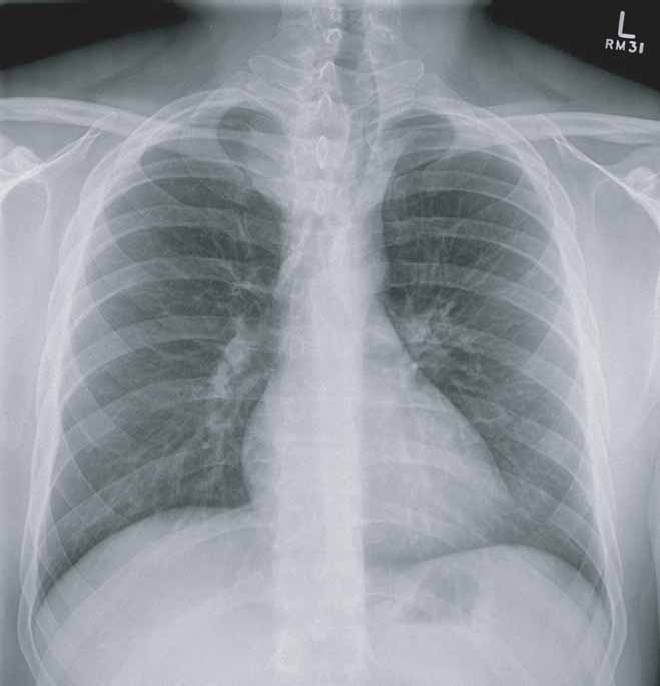
Chest x-ray demonstrating marked tracheal deviation to the left due to the mass extending down into the mediastinum from the right neck.

Axial scan through the base of the neck showing the mass displacing the trachea to the left.

Axial scan at the level of the mandibular angles showing the nodule medial to the left mandibular angle.

Coronal reformat showing both the mass in the right neck and the left submandibular nodule.

Ultrasound view of the right neck showing a large hypervascular mass replacing the right thyroid lobe.
At preoperative surgical review five months later, the right sided goitre was confirmed clinically; however enlarged left cervical nodes were noted. Neck ultrasound identified a mass immediately lateral to the left submandibular gland (2.5 × 2.5 × 1.5 mm) felt to be consistent with an enlarged lymph node. Ultrasound guided FNA of this mass raised the possibility of thyroid tissue. A tentative diagnosis of thyroid carcinoma was made and the patient planned for total thyroidectomy, central lymph node dissection and left modified radical neck dissection.
At the initial left neck dissection, there were enlarged left upper jugular nodes (1–3 cm), and a normal left submandibular gland. In addition, there was a gray nodule straddled across the bifurcation of left common carotid artery consistent with a “carotid body tumour”, which is essentially a paraganglioma occuring at the carotid bifurcation. The thyroid gland was macroscopically normal. The apparent “right goitre” appeared to be a large paraganglioma. Histology revealed enlarged reactive left jugular nodes, normal thyroid, and bilateral paragangliomas with no evidence of malignancy.
Case 2
A 44 year old female presented to her general practitioner after twelve months of generalized bone pain and general deterioration of health. There was no significant past medical history. Biochemical investigations were normal apart from hypercalcaemia and a raised alkaline phosphatase. Thoraco-abdominal CT scan demonstrated multiple lytic lesions within the spine, ribs, pelvis and femora. Furthermore, a mass was noted on the right side of her neck suspicious of a primary thyroid tumour. Radionuclide thyroid scan demonstrated a non-functioning right hemi-thyroid nodule.
A dedicated head and neck CT showed a large soft tissue mass (32 × 30 mm) almost completely replaced the right lobe of the thyroid. It extended behind the trachea and reached across the midline to the posterior aspect of the left hemi-thyroid (Fig. 2a). There was also in-bowing of the right posterolateral wall of the trachea suggesting possible local invasion. A 9 mm lymph node was noted behind the right sternocleidomastoid at the level of the suspected thyroid tumour (Fig. 2b). Widespread skeletal metastatic deposits were again noted. A 99 mTc MDP whole body bone scan also confirmed widespread metastatic deposits (Fig. 2d). The conclusion was that of right sided thyroid cancer with probable cervical lymph node involvement.

CT at the level of the thyroid gland demonstrating a mass related to the posterior aspect of the right lobe of thyroid. Note the deformity of the adjacent trachea and extension of the mass to the posterior of the left lobe of the thyroid.

CT demonstrating 9 mm lymph node behind the right sternocleidomastoid.

CT showing a subtle tissue plane between the metastatic salivary gland tumour deposit and the right hemithyroid.

99mTc MDP whole body bone scan showing widespread skeletal metastases.
Ultrasound-guided FNA cytology demonstrated malignancy but was unable to conclude on tissue typing even with the use of immunohistochemistry. During this time the patient had continued to deteriorate and developed a pathological left neck of femur fracture. At surgery for a left hip hemi-arthroplasty, samples from the femoral reamings and the left femoral head were supportive of poorly differentiated metastatic tumour. The tumour was distinctly basaloid but with some adenoid cystic carcinoma features and with diffuse and strong CD117 positivity (1). This morphology and immunophenotype were most likely from a salivary gland hybrid carcinoma.
Discussion
The solitary neck mass is a clinical problem that can be difficult to evaluate as there is an extensive potential differential diagnosis. As has occurred in our cases, such masses may be clinically evident or may be detected incidentally in the course of imaging for other clinical indications. A major factor in the differential diagnosis is the patient's age. Younger patients less than 40 years of age are likely to have a benign lesion which may be congenital and inflammatory. In older patients most lesions are malignant either primary or metastatic. However if the mass is of thyroid origin, only an estimated 5–10% of solitary thyroid nodules are malignant. Therefore accurately identifying the anatomical origin of a lesion is of value. Although a thorough history and examination can go a long way towards establishing a diagnosis, acquisition of histology or cytology is often needed to reach a definitive diagnosis. The technique of fine needle aspiration (FNA) has been described since the 1840's and is certainly a well accepted diagnostic tool (2,3). Supported by imaging guidance, usually ultrasound, it is even safer and more accurate and is today the main diagnostic tool in the work up of such masses. The false negative ultrasound-guided FNA rates for thyroid carcinoma range from half a percent to five percent (4–7). False positive rates are less than five percent and usually involve focal hyperplasia or cellular atypia in adenoma (8,9). La Rosa et al presented the most comprehensive study in this regard demonstrating false negative rate of 2.3 percent and a false positive rate of 1.1 percent in a series of 5605 FNA procedures (10).
Ultrasound is the most commonly used imaging modality in the evaluation of thyroid and neck masses. This non-invasive study provides an evaluation of the relationship of the lesion to other normal structures. The ability of ultrasound to distinguish between malignant and benign lesion is however very limited. CT and MRI can also be used to evaluate soft-tissue extension of large or suspicious thyroid or masses and to assess cervical lymph node metastases. CT is usually the imaging modality of choice being more available and cost effective. The development of newer technology and methods of acquisition, such as the multidetector CT scanner, allows improvement in image quality, resolution, better reconstructions, and less artefacts (11,12). MRI is superior to CT scanning in soft tissue detail and is particularly useful in the evaluation of the extension of metastatic lymphadenopathy into the base of the skull (11).
In patients with a retrosternal goitre and normal thyroid function, there is little or no role for a nuclear medicine thyroid scan in the management. Assuming a scan was performed in the setting of the first case, the mass would be “cold”, an FNA would have been done and the end result would be the same. That is, surgery would have been offered for a young patient with a significant “retrosternal, cold goitre”.
Both of these cases reported represent rare causes of neck tumours that could not be diagnosed with the traditional diagnostic strategy and demonstrates the difficulties that can confront radiologists in trying to identify the origin of neck tumours.
In the first case, the right lobe of the thyroid was erroneously interpreted as being enlarged on both ultrasound and CT. The initial CT scan, which was with intravenous contrast, was organized by the patient's family doctor, prior to being seen by our team. It is recommended that intravenous contrast be avoided when performing a neck CT scan for thyroid goiter, just in case the patient has a well differentiated thyroid cancer. This is because the iodine in the contrast may interfere with post-operative radio-active iodine treatment. However, it is not an absolute contraindication. If a patient has had contrast, the radioactive iodine therapy can be delayed for six months with no detrimental effect to the patient's longevity. The mainstay of treatment for well differentiated thyroid cancer is good surgery.
The FNA of the right lobe of the thyroid was incorrectly reported due to the similar appearance of neuroendocrine cells and thyroid tissue. The problems on the left side of the neck were compounded by large reactive jugular nodes. Ultrasound guided FNA mistook the “carotid body tumour” for a jugular node again due to the similar appearance of the neuroendocrine cells of the carotid body tumour to thyroid epithelium. The intra-operative finding of bilateral paragangliomas was not suspected clinically and could not have been predicted using traditional diagnostic strategy. These tumours are usually diagnosed via contrast or radionuclide angiography (13), or by duplex Doppler ultrasound but a significant proportion (one third of all cases) remain misdiagnosed pre-operatively (14). Angiography has been considered as the investigation of choice as it confirms the diagnosis and indicates the size and vascularity of the tumour; determines bilaterality, distal intracranial outflow and collateral circulation. Angiography was not requested in this case as the possibility of a carotid body tumour was not suspected at initial workup. FNA diagnosis is generally considered precarious and unnecessary.
In the second case, the right sided neck mass was an incidental CT finding and was not clinically obvious. Initial interpretation of the CT was confusing, suggesting a thyroid tumour. However the ultrasound guided FNA was not able to provide a tissue diagnosis. Furthermore, the patient's clinical picture was not supportive of a thyroid cancer because the patient presented with many months of bone pain, widespread skeletal metastases, a pathological hip fracture and did not have an obvious thyroid nodule. This would be quite an unusual presentation for thyroid cancer. This case highlights the importance of considering the clinical picture of patients in the interpretation of investigation results. On retrospective review of the CT films, the mass appeared to be behind and separate from the right lobe of the thyroid, as normal thyroid could be seen compressed anteriorly by the mass and there appeared to be a tissue plane between the two structures (Fig. 2c).
In summary, these cases demonstrate that there will be the odd occasion where masses which initially appear to be arising from the thyroid on either ultrasound, CT or radionuclide imaging may not actually be thyroid masses at all. Therefore, a high degree of suspicion has to be held when the overall clinical picture does not fit with “just another thyroid nodule”.