
Abstract
Ectopic thyroid gland is a rare anomaly in the development of the thyroid gland. It is defined as any thyroid tissue that is not found on its usual topography. We present the case of a 62-year-old patient with difficulty swallowing solid food, occasional sore throat, hoarse voice, and difficulty speaking. The patient was in hypothyroid status. Thyroid scintigraphy and magnetic resonance imaging visualized a nodular mass on the base of the tongue, suprahyoid, and mediosagittal. The pathohistological finding revealed normal thyroid tissue with few colloidal changes, ruled out tumour infiltration and specific inflammatory process. She received hormonal suppression treatment as a first-line treatment. The patient showed significant improvement in symptoms with reduction of the dyspnea and the dysphagia and normalization of thyroid hormone tests.
Introduction
The ectopic thyroid gland was first described by Hickmam in 1869. 1 In most cases, it is located in the area of the base of the tongue (90%). Other potential localizations include the sublingual region, submandibular, or anterior part of the tongue. It can be also found in the trachea, larynx, mediastinum, and heart. Female is predominant (88.3%). 2
The ectopic thyroid gland at the base of the tongue is often asymptomatic but can cause local symptoms, such as dysphagia, dysphonia, upper airway obstruction, bleeding, and is often combined with hypothyroidism. The incidence of lingual thyroid is reported as 1:100,000. 1 The ectopic thyroid gland is in most cases identified during the neonatal period. In some cases, the onset of symptoms and diagnosis are prolonged until the sixth decade of life. The ectopic thyroid gland increases during stress or is accidentally diagnosed during radiological examinations. 3
Incomplete migration leads to cervical thyroid gland, and excessive migration leads to mediastinal localization. In affected individuals, 70% have a displacement of the thyroid gland and approximately 2/3 have varying degrees of hypothyroidism. 4 Other possible localizations of the ectopic thyroid gland are the head and neck: trachea, axilla, heart and ascending aorta, lymphoid tissue, gastrointestinal system, adrenal gland, and reproductive system. 5
Ectopic lingual thyroid is usually asymptomatic (47%) but can lead to foreign body sensation, dysphagia to solid foods, dysphonia, odynophagia, hoarseness, hot potato voice, and upper airway obstruction. 6 Clinical manifestations of hypothyroidism are present in 70% of cases. 7 Palpation of the neck is essential in order to check the presence or the absence of the thyroid gland in its normal position. 1
Case report
We present a 62-year-old patient who came for an examination due to the feeling of heart palpitations, difficulty swallowing solid food, occasional sore throat, hoarse voice, and discreetly difficult speech. Physical examination revealed no pathological findings. In laboratory tests, except for elevated values of the free thyroxine 10.3 nmol/L and the thyroid-stimulating hormone 25.3 μIU/mL, no deviations were observed. Thyroid ultrasonography revealed atrophic thyroid gland and submandibular ventrally ectopic vascularized nodes with a diameter of 34 × 27 mm. Laryngoscopic examination revealed a large smooth tumour in the area of the root of the tongue, pre-epiglottic, caudal to the hyoid. Technetium (Tc99m) thyroid scintigraphy in the projection of the thyroid gland did not visualize the accumulation of Tc99m but showed the inhomogeneous accumulation of radiopharmaceuticals in the projection of the base of the tongue (Figure 1).
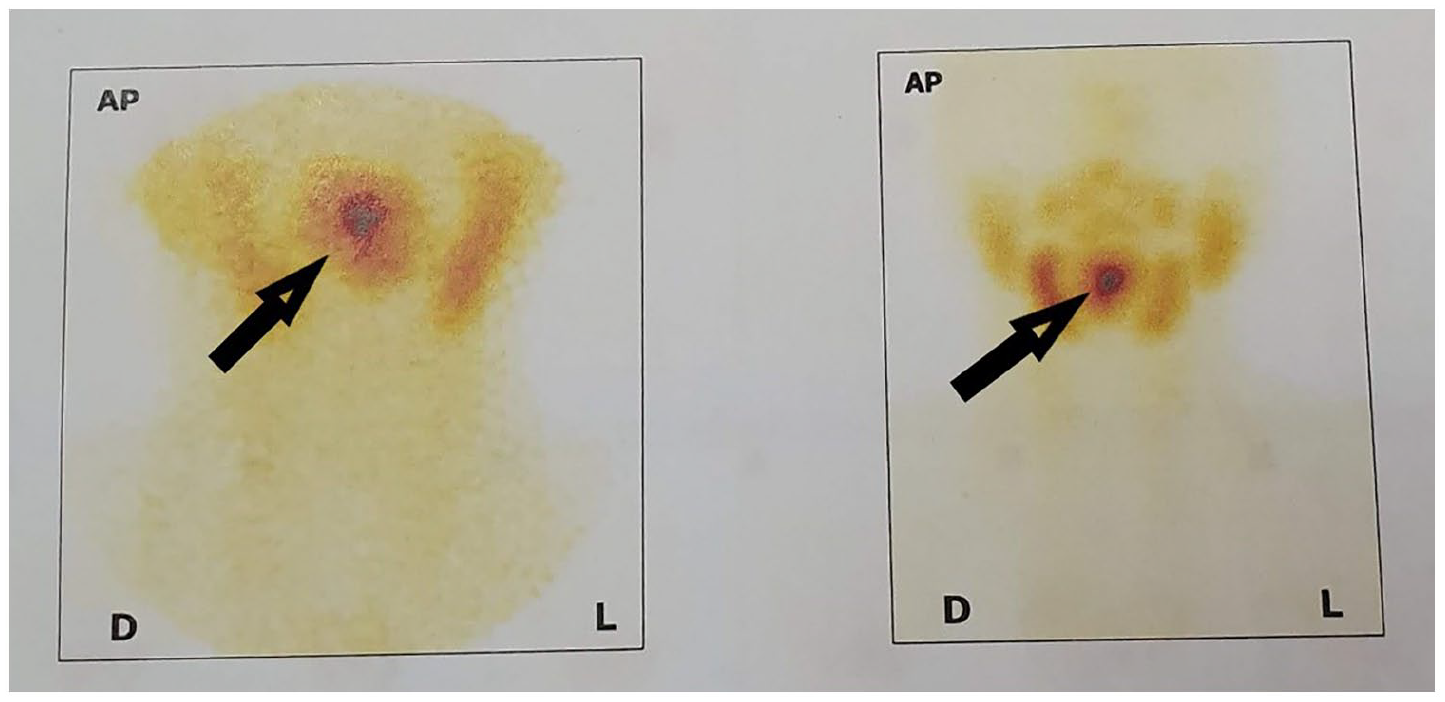
Thyroid scintigraphy visualizes a circular ectopic thyroid gland at the base of the tongue.
Magnetic resonance imaging of the neck indicated a nodular mass suprahyoid and midsagittal, clearly demarcated towards the lumen of the oropharynx and palatine arches. The mass was 24 × 27 mm, inhomogeneous, mixed-signal intensity in T2W, isointense with hypointense zones, without diffusion restriction, with intense inhomogeneous postcontrast signal intensity amplification. The thyroid gland was not clearly differentiated. No pathologically altered lymph nodes in the neck were observed (Figure 2).

Magnetic resonance imaging of the neck, sagittal view (T1W) showed a clearly limited inhomogeneous nodular mass relative to the lumen of the oropharynx.
Microlaryngoscopy to take biopsy samples was performed. The pathohistological finding revealed normal thyroid tissue with few colloidal changes, ruled out tumour infiltration and a specific inflammatory process. After substitution with 100 mg of levothyroxine, 4 weeks later, she was introduced into the euthyroid state via thyroid-stimulating hormone (1.3 μIU/mL). Suppressive therapy with exogenous thyroid hormone was performed in order to decrease the size of the gland. Evolution has been favourable, and the patient showed significant improvement in symptoms with reduction of the dyspnea and the dysphagia and normalization of thyroid hormone tests. Elective surgery following the suppression therapy was planned in case of worsening symptoms. Clinical examination was performed and thyroid function monitored at regular intervals. She was advised to have a liquid diet and intensive care of the oral cavity.
Discussion
We present this case report to indicate the possibility of the absence of symptomatology over a longer period and to show the importance of diagnostic and therapeutic procedures in lingual ectopic thyroid. Lingual thyroid does not usually lead to any symptoms unless an increase in gland size occurs. In symptomatic cases, patients present with complaints of dysphagia, dysphonia, foreign body sensation in the throat, cough, pain, bleeding, and dyspnea. 8
Asymptomatic euthyroid patients usually do not require therapy but are under regular monitoring. For those with symptoms, treatment depends on the size of the gland, nature of the symptoms, status of the thyroid gland, and pathohistological findings. In patients with compensated hypothyroid–status euthyroid, suppressive hormonal therapy is used at the start of treatment. This therapy causes a reduction in the size of the gland. 9
Thyroid stimulating hormone (TSH) levels rise during childhood, puberty, pregnancy, and menopause, leading to ectopic tissue hypertrophy.6,10 Our patient had the mentioned course of disease development. Malignant transformation can occur, though the incidence is only 1%. 11
Technetium (Tc99m) thyroid scintigraphy may avoid the need for a diagnostic biopsy, which involves risk of uncercible bleeding or acute thyrotoxicosis. Treatment depends on severity of symptoms, size of the lesion, sex and age of the patient, and thyroid function. 12 Therapeutic approach should be assessed according to symptomatology. No treatment is required when the lingual thyroid is asymptomatic. Treatment could be conservative with substitutive hormone treatment in patients with mild symptoms. 6 Suppressive therapy with thyroid hormone should be tried first in order to decrease the size of the gland. 6 Administration of a suppressive dose of thyroid hormones aims to decrease the TSH level and therefore can reduce the ectopic glandular volume and consequently reduce all the compressive symptoms. 8 Indications for surgical removal are malignancy, cystic degeneration, bleeding, ulceration, uncontrolled hyperthyroidism, and severe compressive, and respiratory symptoms. 6 Alternatives to surgery are embolization alone or transoral laser excision, radio frequency, or radioiodine previous to surgery. In literature, several surgical approaches are described, such as surgical removal of the mass with external approaches, trans-hyoid, lateral pharyngotomy, or transoral radiofrequency ablation.6,8,13 New technique recently used for surgery is transoral robotic surgery. 13 Ablative radioiodine therapy is an alternate approach recommended in aged patients or patients unfit for surgery.6,12 Alternative treatment for patients not accepting surgical treatment or those not fit for general anaesthesia is radioactive iodine therapy. 8 Some lingual thyroid glands are visible on the neck, and female patients prefer surgical removal for cosmetic reasons.9,14
Conclusion
Management of lingual thyroid is still controversial. All treatments options would allow the patient to improve quality of life. The risks and benefits of treatment modality should be discussed with the patient. Careful examination is recommended in order to trace any potential complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient provided written informed consent for publication of the case report.