
Abstract
Introduction
Papillary thyroid cancer corresponds to approximately 1% of all carcinomas; nevertheless, it is the most prevalent endocrine neoplasm in the world. Studies reveal that the BAX (−248 G > A) polymorphism may be associated with negative regulation of BAX gene transcription activity, causing a decrease in its protein expression.
Objective
The present study aimed to describe the genotype and allele frequencies of BAX single nucleotide polymorphisms (−248 G > A) (rs4645878) in the research patients, and to associate its presence with susceptibility to papillary thyroid cancer.
Methods
This case-control study was conducted with 30 patients with papillary thyroid cancer. For the evaluation of genetic polymorphisms, the polymerase chain reaction-restriction fragment length polymorphism technique was employed. Allele and genotype frequencies were estimated using the SPSS program, and significant associations were considered when p < 0.05.
Results
There was a significant genotypic difference between papillary thyroid cancer and the control group (p = 0.042). The GG genotype provided a protective factor for papillary thyroid cancer (p = 0.012, odds ratio (OR) = 0.313; confidence interval (CI) = 0.123–0.794). Likewise the G allele was a protective factor for papillary thyroid cancer (p = 0.009; OR = 0.360; CI = 0.163–0.793). The BAX gene polymorphism (−248 G > A) was associated with papillary thyroid cancer.
Conclusion
BAX (−248 G > A) GG genotype carriers, or at least one mutated allele, was associated with papillary thyroid cancer in the Brazilian population studied, and the G allele presence is considered a protective factor against papillary thyroid cancer occurrence.
Introduction
Thyroid carcinomas are classified into papillary thyroid carcinoma (PTC), follicular thyroid carcinoma, medullary thyroid carcinoma, thyroid carcinoma poorly differentiated, and anaplastic thyroid carcinoma, based on histopathology. 1 PTC is the most common histological type of thyroid cancer; nevertheless, it is also the least aggressive. 2 PTC incidence is more common in women and Caucasians and its incidence increases with age. 3
In Brazil, thyroid gland carcinoma corresponds to approximately 1% of all carcinomas and is the most prevalent endocrine neoplasm globally. The number of new thyroid cancer cases estimated for each year of the 2020–2022 triennium will be 1830 new cases in men and 11,950 in women. For the Federal District, the estimate is 140 new cases. 4
B-cell lymphoma 2 (Bcl-2) associated with protein X (BAX) is a crucial pro-apoptosis protein in the Bcl-2 family, mainly existing in the cytoplasm. When cells receive apoptotic signals, the BAX proteins transfer to the mitochondrial membrane, where they recognize and bind the membrane-bound Bcl-2 proteins to form the BAX-Bcl-2 heterodimer, thus inhibiting the Bcl-2 proteins' anti-apoptosis function. BAX proteins can also form the BAX-BAX homodimer in the mitochondrial membrane, thereby increasing the mitochondrial membrane's permeability and releasing cytochrome C, an apoptotic factor, into the cytoplasm to activate the apoptosis cascade response. Therefore, BAX has a vital role in regulating the signaling pathway for mitochondrial apoptosis. 5
The association between BAX gene polymorphisms and cancer is related to cancer occurrence and the patient's prognosis. Studies show that the (−248 G > A) polymorphism may be associated with negative regulation of BAX gene transcription activity, causing a decrease in its protein expression, which increases the Bcl-2 and BAX ratio and may inhibit the apoptotic process of tumor cells. 6
Thyroglobulin serum measurement and a 131I scintigraphy are generally accepted as a key part of the diagnostic strategy in patients with well-differentiated thyroid cancer (DTC) after thyroidectomy. However, neither planar nor single photon emission computed tomography (SPECT) acquisitions are able to determine the location of lesions correctly. Spanu et al. 7 state that the combination of SPECT and computed tomography (SPECT/CT) provides a better anatomical image and improves the 131I planar image's ability to detect iodine-avid foci suggesting that SPECT/CT is the best technique for the follow-up of thyroidectomized DTC patients. 131I-SPECT/CT appears to be superior to whole-body scintigraphy (WBS) in detecting malignant lesions and cervical lymph node metastases that could be used as a complementary tool to the WBS.8,9
Thyroid cancer molecular markers are found in more than 70% of differentiated carcinomas, and the understanding of its different molecular mechanisms is favorable to new perspectives for its diagnosis and treatment. 10 Among the various molecular markers described are the genetic variants; that is, a molecular alteration in at least 1% of the population, and when such molecular variations occur in only one nucleotide, these polymorphisms are called SNPs (single nucleotide polymorphisms). 11
To this end, the present study aimed to describe the genotype and allele frequencies of BAX SNP (−248 G > A) (rs4645878) in the research patients and to associate its presence with susceptibility to papillary thyroid cancer.
Material and methods
Subjects
The Centro Universitário de Brasília (UniCEUB) Ethics Committee approved this study for genetic analysis under CAAE No 57382416.6.0000.0023.
The sample size was calculated using the Raosfot software (Sample Size Calculator), estimating a prevalence of 1% of thyroid cancer among the cancer types in the adult population, a 5% sampling error and 95% confidence interval (CI) in the number of 8450 patients a sample size of 12 participants was reached. A sample size of 30 PTC patients was admitted considering possible compensation of losses.
As a case-control study, the research participants were divided into two groups. The case group consisted of 30 PTC patients (20 female, 11 male) over 18 years old (average age: 48 ± 13 years) that underwent thyroidectomy and radioiodine therapy at a Federal District private clinic. The control group consisted of 81 healthy volunteers (43 female, 38 male) with a mean age of 52 ± 5 years, paired and unrelated to the case group. The participants were excluded from both groups if they were younger than 18 years old, were not eligible for radioiodine therapy, and refused to participate in the research or for whom legal representatives did not consent.
Laboratory methods
After signing the Free and Informed Consent Terms and the Biological Material Guard Terms, and answering a proposed questionnaire, each participant had 10 mL of venous blood collected.
For the evaluation of genetic polymorphisms, DNA was extracted from peripheral blood using the PureLink®Genomic DNA Mini Kit from Invitrogen (catalog # K1820-02, lot # 19339891) and had an average concentration of 20 ng/μL. Then, the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) technique was applied to study the SNPs’ distribution.
The polymerase chain reaction (PCR) technique was performed for BAX genotyping (−248 G > A) (rs4645878). The primers used were 5′–CATTAGAGCTGCGATTGGACCG −3′ (sense) and 5′–GCTCCCTCGGGAGGTTTGGT −3′ (antisense).
The thermocycling conditions were 96°C/5 min (initial denaturation), followed by 35 denaturation cycles at 96°C/45 s, succeeded by 56°C/40 s for the primers' annealing, and 72°C/30 s for the fragments' extension. The final extension was performed at 72°C/10 min.
These primers amplified a 109 bp DNA fragment that was then digested using the MspI Fast Digest restriction enzyme (Fermenta, Lote 00066274, Exp. 03.2014). This digestion was performed in a water bath at 37°C for 2 hours and then revealed through a 4% agarose gel, stained with 4 µL of ethidium bromide (10 mg/mL) using the transilluminator. The following genotypic pattern was observed: the wild homozygote (GG) produced two bands (89 bp and 20 bp), the heterozygote (GA) produced three bands (20 bp, 89pb, and 109 bp), and the mutated homozygous allele (AA) produced only one 109 bp band.
Statistical analysis
Allelic and genotypic frequencies were estimated using the SPSS version 20.0 program by direct counting and expressed as a percentage. The Chi-square test and the odds ratio (OR) were applied to compare the frequency distributions and analyze possible associations with the alleles and genotypes between the two groups evaluated (case and control) and describe their summary statistics. Mann-Whitney test and Kruskall-Wallis test were used to compare PTC patients' genotype frequencies with their clinical characteristics: thyroglobulin, TSH, and BMI. Fisher's exact test and OR was used to analyze the association between the distribution of antithyroglobulin (IU/mL), sex, and administered radiopharmaceutical dose (mCi) in PTC patients and their genotype. Fisher's exact test and OR were also used to examine the association between PTC patients' tumor staging, per TNM classification, and their genotype. Significant associations were recognized if probabilities were less than 5% (p < 0.05).
Results
Thirty participants (mean age 43 years ± 13 years) with PTC constituted the case group, whereas 81 healthy participants (mean age 40 years ± 9 years) constituted the control group. The BAX (−248 G > A) polymorphism genotype frequency in the control group was in Hardy–Weinberg equilibrium (p = 0.130).
Table 1 describes the genotypic and allelic distribution in the case and control group, in which most of the PTC group (60.0%) had a GG genotype. The same occurred in the control group (82.7%). Furthermore, the genotypic difference between the groups was statistically significant (p = 0.041).
BAX (−248 G > A) polymorphism genotypic distribution in the case and control groups.
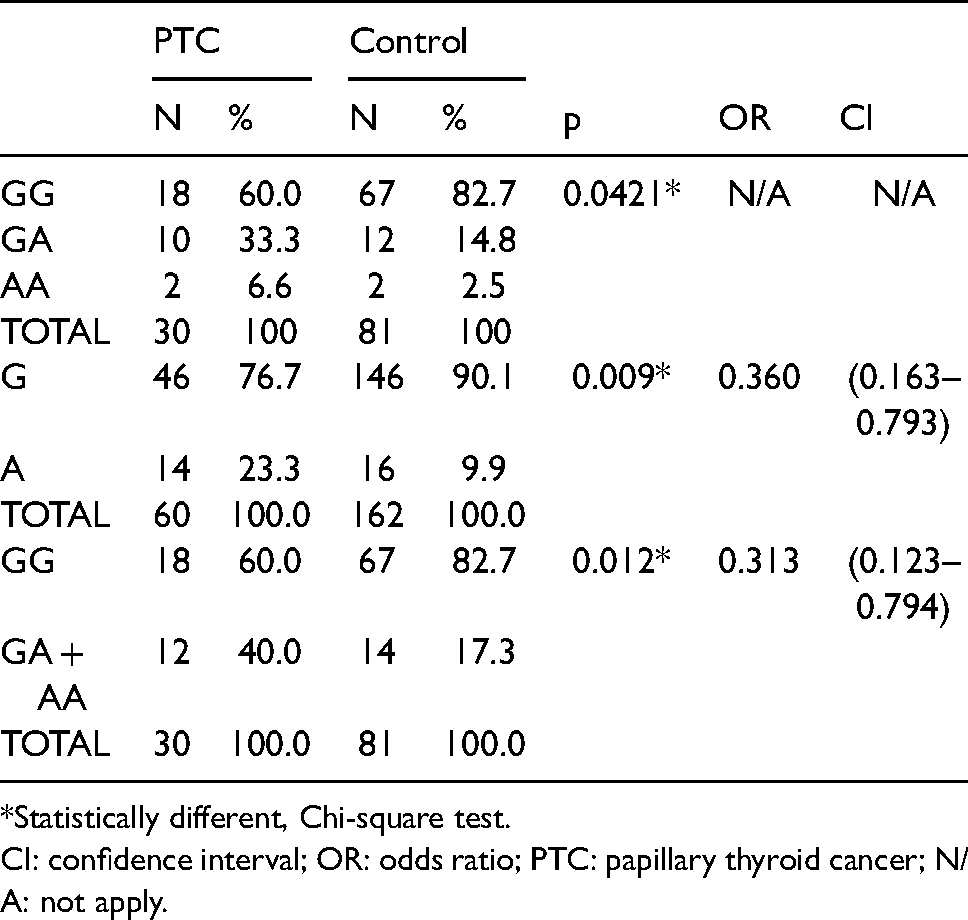
*Statistically different, Chi-square test.
CI: confidence interval; OR: odds ratio; PTC: papillary thyroid cancer; N/A: not apply.
When assessing the allelic distribution, 76.7% of the PTC patients had the G allele, against 90.1% in the control group, and a statistical difference between the alleles studied and protection for the PTC occurrence in the wild allele carriers was observed (p = 0.009; OR = 0.360; 95% CI = 0.163–0.793). Moreover, when dichotomizing the genotypes, it was possible to observe a statistical difference between the data, suggesting that the GG genotype presence was a protection against the PTC occurrence (p = 0.012; OR = 0.313; 95% CI = 0.123–0.794).
From the results obtained, the associations between the genetic variant and clinical characteristics linked to PTC patients were analyzed, such as thyroglobulin serum concentration, thyroid-stimulating hormone (TSH), antithyroglobulin, body mass index (BMI), sex, administered dose, and tumor staging (tumor node metastasis (TNM) classification). No statistical differences were found between the BAX genetic variant and these variables (Table 2).
Median, 25th percentile (P25), 75th percentile (P75), and p-values of the variables: thyroglobulin, TSH, and BMI in PTC patients, according to the genotype.
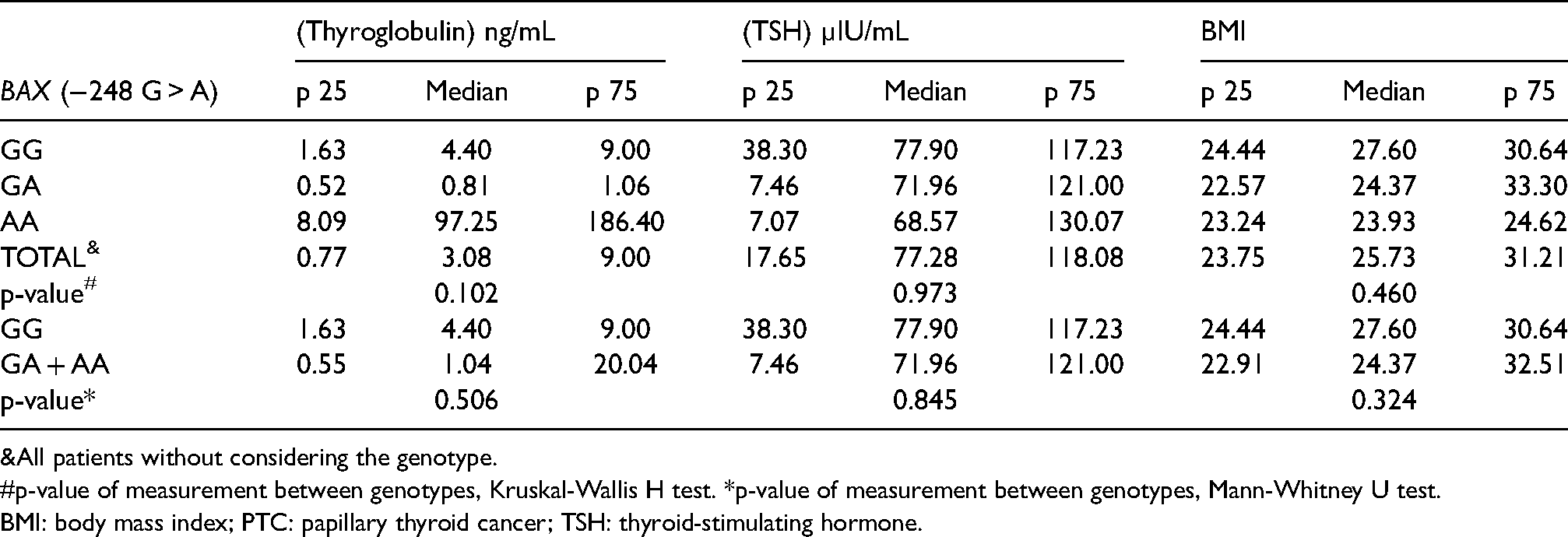
All patients without considering the genotype.
p-value of measurement between genotypes, Kruskal-Wallis H test. *p-value of measurement between genotypes, Mann-Whitney U test.
BMI: body mass index; PTC: papillary thyroid cancer; TSH: thyroid-stimulating hormone.
Table 3 describes the association of the genetic variant studied and the antithyroglobulin concentration in PTC patients, in addition to their sex and the administered drug dose. Regarding antithyroglobulin concentration, 10 of the PTC participants (76.9%) with the GG genotype had a concentration > 20 IU/mL. Furthermore, most of the PTC carriers with the GG genotype (70.6%) were female compared to the male. It is worth mentioning that there was no statistical difference between the genotypic groups and the variables studied. Regarding the dose of the radiopharmaceutical administered, 14 patients (82.4%) with the GG genotype received doses ≤ 150 mCi and only 3 (17.6%) with the GG genotype received the dose > 150 mCi. None of these three studied characteristics presented a statistically significant difference.
Analysis of the association between the distribution of antithyroglobulin (IU/mL), sex, and administered radiopharmaceutical dose (mCi) in PTC patients, according to the genotype.
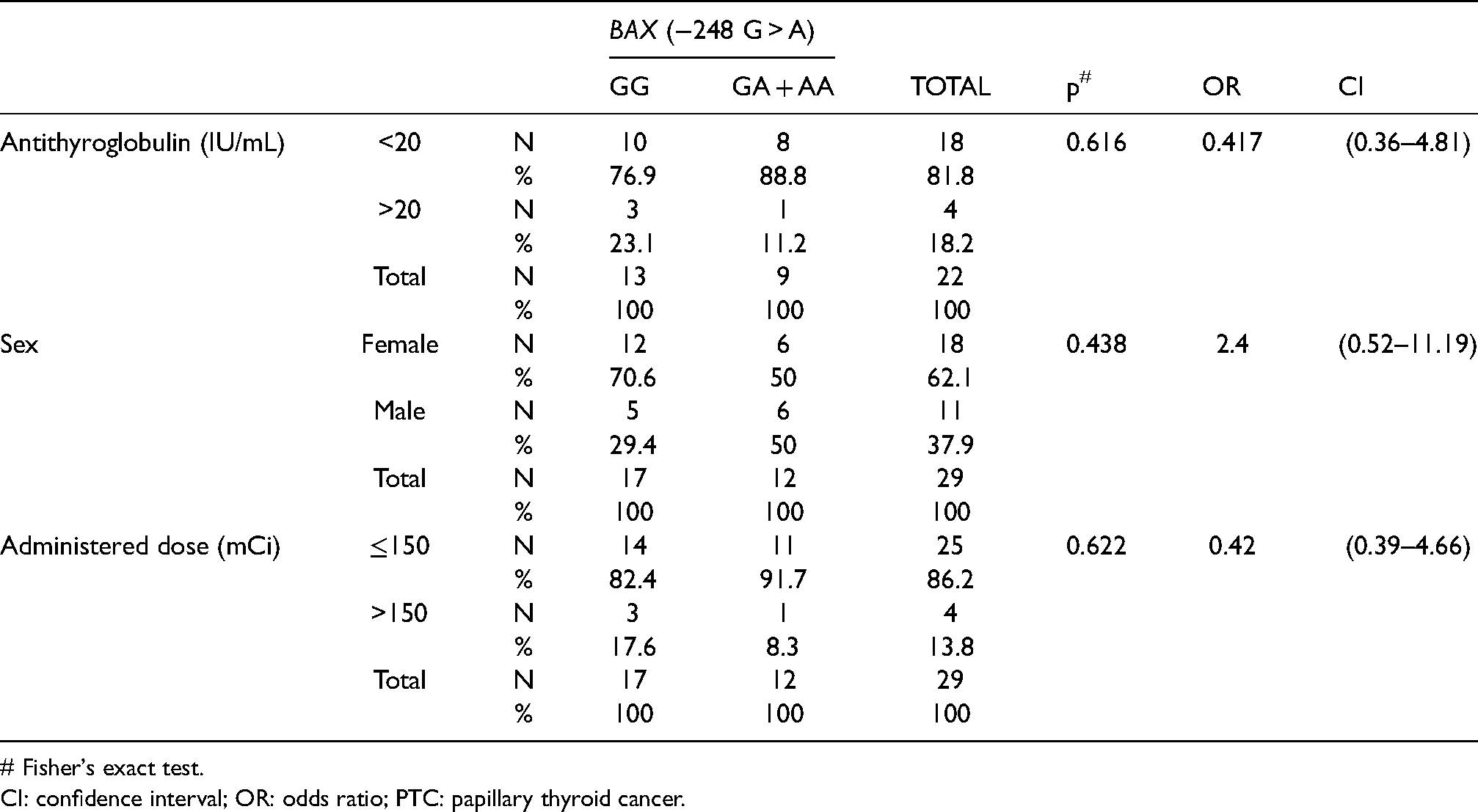
# Fisher's exact test.
CI: confidence interval; OR: odds ratio; PTC: papillary thyroid cancer.
Analyzing tumor staging per TNM classification system, half of the PTC patients with the GG genotype had T1 + T2 staging, while the other half had T3 + T4 staging. It was also noted that when assessing the N stage in GG genotype individuals (two), one (50%) had N0 staging, the other (50%) had N1 staging. In the statistical evaluation of the characteristics studied, no significant differences were observed. As for metastasis (M), one participant with the GG genotype and one with the GA + AA genotype presented M1 staging (Table 4).
Analysis of the association between tumor staging per TNM classification and PTC patients, according to genotype.
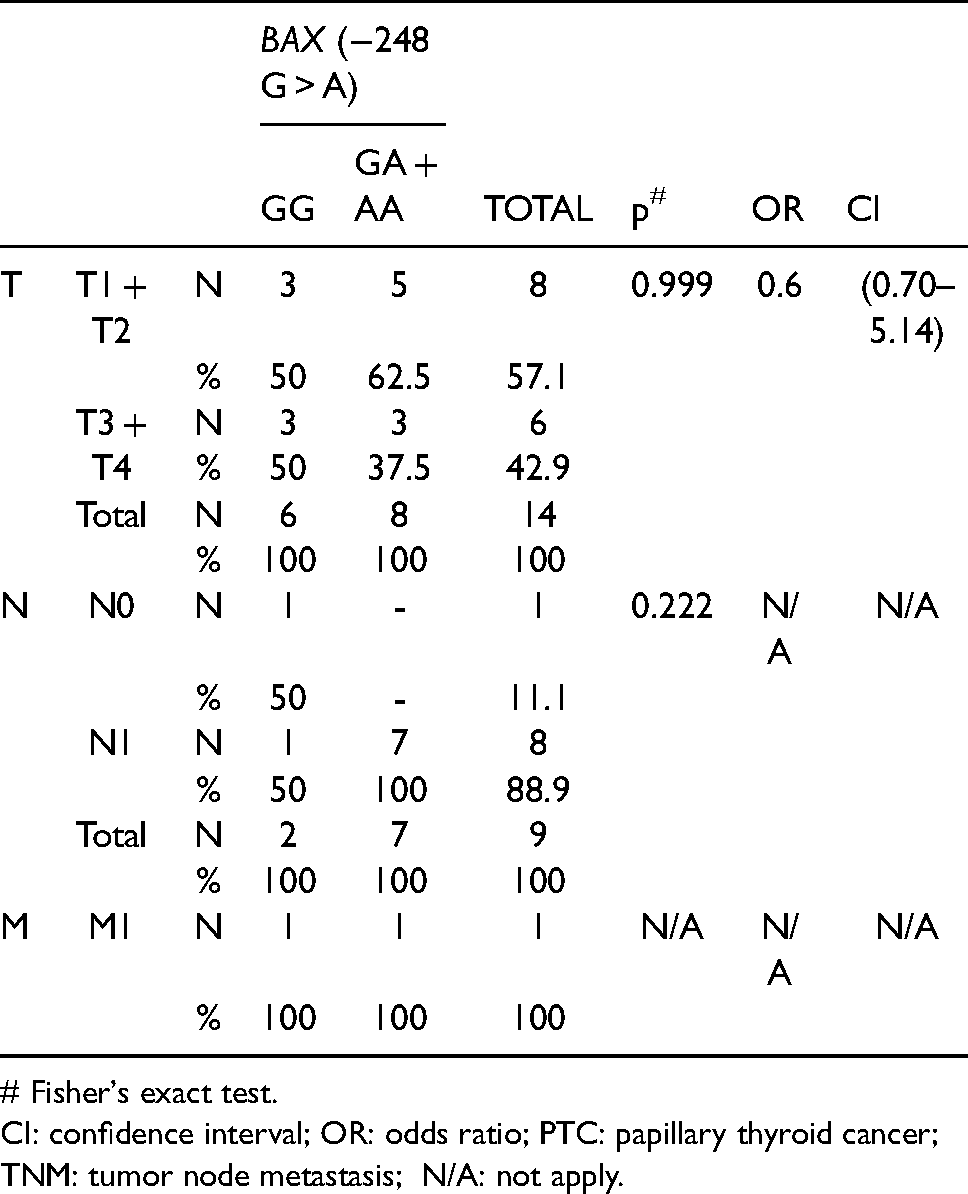
# Fisher's exact test.
CI: confidence interval; OR: odds ratio; PTC: papillary thyroid cancer; TNM: tumor node metastasis; N/A: not apply.
Discussion
The present study found a statistically significant difference between the G allele presence in the BAX gene polymorphism (−248 G > A) and PTC occurrence, and the G allele is the most common allele among the PTC and control groups (p = 0.009).
Likewise, an Indian study on ovarian cancer and BAX −248 G/A polymorphism detected an association and an increased risk in individuals with the AA genotype and ovarian cancer occurrence (ORs = 4.1; 95% CI = 1.23–13.97). 12 Mirmajidi et al., 13 in a polymorphic analysis of the BAX (−248 G > A) gene in a sample of patients with gastric cancer, also noted that the G allele was more frequent between the case and control group. This study's in silico analysis demonstrated that the BAX (−248 G > A) alteration removed the SP1 transcription factor from AA genotype samples, affecting the cell's gene expression. Thus, BAX (−248 G > A) polymorphism might affect its protein expression, and the G allele presence might be protective against cancer occurrence.
A retrospective study of the medical records of patients undergoing thyroidectomy at a public oncology referral hospital in the São Paulo State from 2009 to 2010 observed, among other factors, an increase in the percentage of patients with well-differentiated thyroid cancer as the BMI (defined by the ratio of weight to height squared) increased, though without a statistical difference. 14 Conversely, the present study found no statistical differences between the genetic variant studied with BMI values.
Tumor markers are molecules that might be present in tumors. An ideal biological marker must be specific and sensitive, identifying the tumor's type and characterizing its severity and staging. For instance, the TSH, produced by the pituitary gland, stimulates the thyroid gland to produce triiodothyronine (T3) and thyroxine (T4). 15 Moreover, all three hormones are used as thyroid cancer markers.
Fighera et al. 16 retrospectively reviewed the medical records of 622 patients with uni/multi-nodular goiter, noting that a TSH > 1.64 mU/L persisted as a risk factor for malignancy regardless of other variables. Patients with follicular lesions had higher TSH levels than patients with a benign cytological diagnosis and concluded that elevated TSH serum levels increased the risk of malignant thyroid nodules and thyroid cancer aggressiveness. No statistical differences were detected between the BAX genetic variant and the thyroglobulin serum concentration, TSH, and BMI values (p = 0.102, 0.973, and 0.460, respectively).
Antithyroglobulin antibodies are produced by immune cells, mainly by lymphocytes that react against auto-thyroid antigens and progressively infiltrate the thyroid gland. The antithyroglobulin antibody incidence is approximately twice as high in patients with differentiated thyroid carcinoma, especially in PTC, compared to the general population, suggesting an association between autoimmune thyroid disease and differentiated thyroid carcinoma. 17 The present study observed no association between the BAX gene (−248 G > A) polymorphism and antithyroglobulin concentrations or the administered radioiodine dose, as there was no statistically significant difference between the PTC patients' genotype groups.
Bilous et al. 18 states that BAX RNA messenger levels decrease in patients with elevated anti-thyroglobulin and anti-thyroid peroxidase serum autoantibody levels, and increase in patients with hypothyroidism resulting from autoimmune thyroiditis and postoperative hypothyroidism.
Kelly et al., 19 in a retrospective observational study, included 1093 patients with differentiated thyroid carcinoma treated between 1995 and 2010, with thyroidectomy performed on all patients included in the study. Women (78%) were predominant in this study—a fact also noted in the present study. PTC was the most frequent (88%), and T1 staging was present in 55.8%, T2 in 19.4%, T3 in 22.1%, and T4 in 2.4%. Concurrently, distant metastases presence was observed in 3.1% of the research participants. An analysis of tumor staging per TNM classification system revealed that half of the PTC patients with the GG genotype had T1 + T2 staging, while the other half had T3 + T4 staging.
Difficulties and limitations encountered during this research were a request for departure from one of the participants, and the results from specific exams were not obtainable for some participants.
In conclusion, BAX (−248 G > A) GG genotype carriers, or at least one mutated allele, was associated with PTC in the Brazilian population studied, and that the G allele presence is considered a protective factor against PTC occurrence. As for the other PTC characteristics and prognoses, no significant associations were detected linked to BAX (−248 G > A) gene.
Analyzing genetic variants assist and facilitate the comprehension of diseases that affect the population. Accordingly, studies that further new forms of early diagnosis, improve the quality of life, and identify risk factors—whether environmental or genetic—must be developed.
Footnotes
Acknowledgments
This work was supported by the Higher Education Personnel Improvement Coordination – Brazil (CAPES)–Financing Code 001. DPI/UnB.
CAPES–Financing Code 001 is a post-graduation scholarship and independent of the research subject.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES - Financing Code 001, N° 0004/2021), Decanato de Pós-Graduação (DPG)/UnB and Decanato de Pesquisa e Inovação (DPI)/UnB.