
Abstract
Background
The aim of this study is to evaluate the prevalence of chronic complications in type 2 diabetic patients in Basrah (Southern Iraq).
Methods
This was a longitudinal descriptive study for patients with diabetes registered in Al-Faiha Diabetes and Endocrine Centre in Basrah (Southern Iraq) for the period from April 2003 to end of February 2009.
Results
Out of 4,926 patients enrolled, 51.0% were women, mean age was 55.0 ± 13.1 years and 67.6% were overweight or obese. Those with duration of diabetes more than 5 years constituted 50.6% and only 25.3% were on insulin. Mean Hemoglobin A1C was 9.3 ± 2.0. The prevalence of the 16 complications studied were as follows: Hypertension in 31.0%, peripheral neuropathy in 13.8%, ischemic heart disease in 7.8%, proteinuria in 6.6%, cereberovascular accident in 4.6%, interdigital fungal infection in 4.3%, heart failure in 3.4%, and erectile dysfunction in 6.0%. In this study 2.8% of patients died of cardiovascular causes, 2.7% developed diabetic foot, 2.4% had non-alcoholic fatty liver, 0.7% had amputation, 0.4% developed ophthalmoplegia, 0.2% had peripheral vascular disease, and 0.04% developed mucormycosis. The chronic complications which were more seen in those with diabetes more than 5 years were hypertension, peripheral neuropathy, ischemic heart disease, proteinuria, cereberovascular accident, heart failure, erectile dysfunction, cardiovascular death, diabetic foot, amputation and peripheral vascular disease.
Conclusion
This study provided the baseline for chronic complications of diabetes in Iraq. Screening for early complications is recommended.
The complications of diabetes account for substantial costs, with management of macrovascular disease being the largest and earliest. If improving glycemic control prevents complications, it will reduce these costs. 1
Cardiovascular disease which is common in type 2 diabetes includes coronary artery disease, stroke, peripheral vascular disease, cardiomyopathy and congestive heart failure. 2 It is estimated that 77% of hospitalizations for chronic complications of diabetes are attributable to cardiovascular disease 3 and 75% of patients with type 2 diabetes die of macrovascular events, such as acute myocardial infarction and stroke. 2
In a mortality study of more than 3,000 patients, 4-year survival was 92% for patients with diabetes duration ≤5 years, and 84% if diabetes duration was ≥5 years. 2
The cost of managing a patient with diabetes and coexisting coronary heart disease and hypertension over 3 years is 300% higher than for diabetes alone (US $46,000 versus $14,000). 4
The total number of people with diabetes is projected to rise from 171 million in 2,000 to 366 million in 2,030, 5 with the greatest increase occurring in developing compared with developed countries. 6
No data is available on the long term complications of diabetes in Iraq.
The aim of the study was to evaluate the prevalence of chronic complications in type 2 diabetic patients in Basrah (Southern Iraq).
Patients and Methods
This was a longitudinal descriptive study for patients with diabetes registered in Al-Faiha Diabetes and Endocrine Centre in Basrah (Southern Iraq) for the period from April 2003 to end of February 2009. The computer based data analysis was done in March 2009. It involved 4,926 type 2 diabetic patients. The study included patients registered in the diabetes center with at least 1 year of follow up.
Exclusion criteria were patients lost to follow up for at least 6 months, patients with incomplete investigations, those with diabetes less than 1 year, pregnant patients, type 1 diabetes patients, those with echocardiography suggestive of dilated cardiomyopathy, patients who had causes of death other than cardiovascular death, and if the age was below 20 years.
Subjects reporting smoking at least one cigarette per day during the previous 3 months before the examination were classified as current smokers. Insulin use was considered as those currently taking insulin whether they take oral therapy with or not.
Subjects were weighed with light clothes and no shoes, and body mass index (BMI) was calculated based on the formula weight/height. 2
Biochemical analyses
Total cholesterol, high-density lipoprotein-cholesterol (HDL-c), and triglycerides (TG) were measured by the enzymatic method (Human, Germany). Low-density lipoprotein-cholesterol (LDL-c) was calculated according to the Friedewald formula. Hemoglobin A1C (HbA1c) was assayed using high performance liquid chromatography (Bio-Rad VARIANT II).
Complications
A search for 16 complications in those patients including hypertension, ischemic heart disease, heart failure, cereberovascular accident, peripheral neuropathy, erectile dysfunction, proteinuria (macroalbuminuria), interdigital fungal infection, death, diabetic foot, amputation, non-alcoholic fatty liver, tuberculosis, ophthalmoplegia, peripheral vascular disease and mucormycosis were done. Search for retinopathy and microalbuminuria were not feasible in this study.
The blood pressure was recorded in the right upper arm in the sitting position after five minutes rest. Patients were categorized as being hypertensive if they were receiving antihypertensive treatment or if the systolic blood pressure was more than 140 mm Hg and/or diastolic blood pressure more than 90 mm Hg.
Ischemic heart disease was diagnosed if there was history of myocardial infarction or angina based on hospital records, angiography, percutanous coronary intervention or coronary artery bypass graft history. Heart failure was based on hospital or clinic records, which were suggestive, or echocardiographic systolic dysfunction.
Cereberovascular accident diagnosis was based on hospital records or any neurological deficit which lasted for more than 24 hours with suggestive neuroimaging.
Peripheral neuropathy was considered if there was persistent numbness, Paresthesia, with loss of a tuning fork tested sense of vibration, or failure to elicit knee and/or ankle jerk reinforcement.
Erectile dysfunction has been defined as the inability to achieve and/or to maintain an erection for a sufficiently long period of time so as to permit satisfactory sexual intercourse.
Proteinuria (macroalbuminuria) was considered for persistent proteinuria by urinary dipstick with at least 3 readings in absence of infection.
Interdigital fungal infection (tinea pedis) was diagnosed based on history and clinical appearance of the feet in addition to direct microscopy of a potassium hydroxide (KOH) preparation for fungal hyphae.
Cardiovascular death was considered in those who died suddenly, or died of acute coronary syndrome or cereberovascular accidents.
Diabetic foot was considered as any past or present history of diabetic foot (any full-thickness skin lesion distal to the ankle excluding minor abrasions, fissures or blisters and amputation (lower extremity) considered if it was done for a diabetic foot at any time. Non-alcoholic fatty liver diagnoses was based on ultrasound findings (The definition of ultrasonic fatty liver was based on a comparative assessment of image brightness relative to the kidneys). Tuberculosis was considered for any site depending of medical records.
Ophthalmoplegia was considered for those with old records or new features of 3rd, 4th or 6th cranial nerve palsies if no other cause was found.
Peripheral vascular disease was considered to be present if there was a definite history of intermittent claudication or if one or more of the peripheral pulses (dorsalis pedis or posterior tibial) were absent on both feet. Mucormycosis diagnosis based on hospital records.
Statistical analysis
Data were collected initially in a specialized data collection form of Microsoft Access, then introduced into Statistical Package for Social Sciences (SPSS) version 15.0 for Windows (SPSS 15.0, SPSS Inc., Chicago, IL, USA) for analysis. Differences between the groups (those with diabetes 5 years and below and the others) were tested by Student's t-test in the case of continuous data and by Chi-square test or Fisher's exact test (low numbers) in case of categorical data. Logistic regression analysis was performed to determine the effect of duration of diabetes and age on complications. P < 0.05 was considered significant.
Results
Basic characteristics of the patients are in Table 1. Of 4,926 enrolled patients, the mean age was 55.0 ± 13.1 years (51.0% women). Smokers constituted 20.3% and mean qualification was 4.8 ± 5.6 years. The mean BMI was 27.4 ± 5.6 (67.6% were overweight or obese). Those with duration of diabetes more than 5 years were 50.6% and only 25.3% were on insulin. The mean HbA1c was 9.3% ± 2.0% with only 4.2% achieving the target. The mean total cholesterol was 207.4 ± 42.9 mg/dl, TG 193.6 ± mg/dl 99.1, HDL-c 46.4 ± 13.1 mg/dl and LDL-c 77.3 ± 66.5 mg/dl.
Baseline characteristics and complications of 4926 patients enrolled in this study.
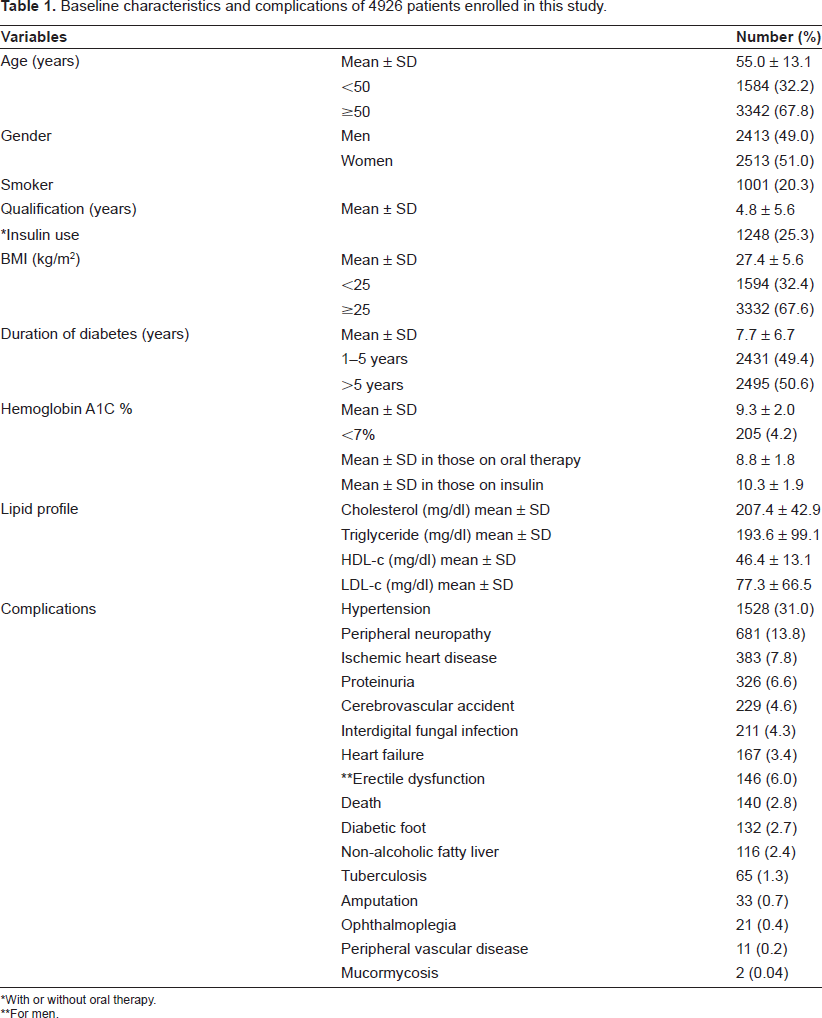
With or without oral therapy.
For men.
The frequency of the 16 complications studied were as follows: Hypertension was seen in 31.0%, peripheral neuropathy in 13.8%, ischemic heart disease in 7.8%, proteinuria in 6.6%, cereberovascular accident in 4.6%, interdigital fungal infection in 4.3%, heart failure in 3.4%, and erectile dysfunction in 6.0%. In this study 2.8% died of cardiovascular causes, 2.7% developed diabetic foot, 2.4% had nonalcoholic fatty liver, 0.7% had amputation, 0.4% developed ophthalmoplegia, 0.2% had peripheral vascular disease, and 0.04% developed mucormycosis.
In Table 2, study of variables was done according to duration of diabetes. Among those with diabetes duration of more than 5 years, the mean age was higher (57.0 ± 12.6 year), with higher qualification (5.4 ± 5.6 year). They are more likely to be overweight or obese (52.3%) and 70.5% of them were insulin users with higher Hemoglobin A1C and TG.
Characteristics and complications distribution according to duration of diabetes.

For men.
The chronic complications seen in those with diabetes more than 5 years were hypertension, peripheral neuropathy, ischemic heart disease, proteinuria, cerberovascular accident, heart failure, erectile dysfunction, death, diabetic foot, amputation and peripheral vascular disease.
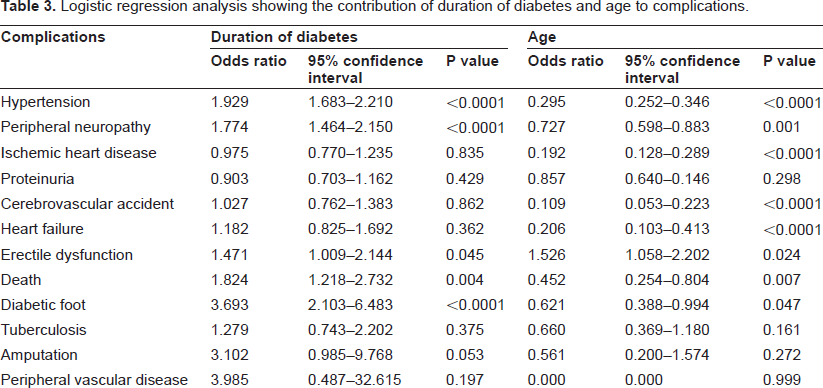
Table 3, shows the influence of duration of diabetes and age on complications. Duration of diabetes has influence more on hypertension (OR, 1.929; 95% CI, 1.683 to 2.210 p < 0.0001), peripheral neuropathy (OR, 1.774; 95% CI, 1.464 to 2.150 p < 0.0001), diabetic foot (OR, 3.693; 95% CI, 2.103 to 6.483 p < 0.0001), death (OR, 1.824; 95% CI, 1.218 to 2.732 p = 0.004) and erectile dysfunction (OR, 1.471; 95% CI, 1.009 to 2.144 p = 0.045). While age contributed more to hypertension (OR, 0.295; 95% CI, 0.252 to 0.346 p < 0.0001), ischemic heart disease (OR, 0.192; 95% CI, 0.128 to 0.289 p < 0.0001), cerebrovascular accident (OR, 0.109; 95% CI, 0.053 to 0.223 p < 0.0001), heart failure (OR, 0.206; 95% CI, 0.103 to 0.413 p < 0.0001), peripheral neuropathy (OR, 0.727; 95% CI, 0.598 to 0.883 p = 0.001) and diabetic foot (OR, 0.621; 95% CI, 0.388 to 0.994 p = 0.047).
Logistic regression analysis showing the contribution of duration of diabetes and age to complications.
In Table 4 comparisons between men and women was made. There were higher mean ages for women (56.0 ± 12.3 vs. 53.9 ± 13.7). Men were more likely to be smokers (81.4% vs. 18.6%) with higher qualifications (7.0 ± 5.7 vs. 2.8 ± 4.6), but higher BMI was found among women. Men had higher duration of diabetes, but women were more likely to use insulin. There were no differences regarding HbA1c, total cholesterol, HDL-c, and LDL-c, but men had higher TG. As regards complications the following complications were found more in women: hypertension, interdigital fungal infection and non-alcoholic fatty liver, while peripheral neuropathy, ischemic heart disease, heart failure, death, tuberculosis and amputation were found more in men.
Characteristics and complications according to gender.

Discussion
This study started for the first time to delineate the pattern of chronic complication of diabetes in Iraq.
Overweight or obese constituted 67.6% in this study, which is not strange since worldwide, 90% of individuals with type 2 diabetes are either overweight or obese. 7
Further more the study reported very high mean HbA1c and only the minority achieved the target of < 7%. This was higher than mean HbA1c of 8.3 ± 2.5 for diabetics in the United Arab Emirates. 8 Worldwide less than 40 percent of patients with diabetes successfully achieve HbA1c level of less than 7%. 9 One reason for this is the reluctance of patients and physicians to start insulin therapy. Only 25.3% of our patients were using insulin. Data from the UK Prospective Diabetes Study suggest that 53% of patients will require insulin after 6 years following diagnosis and 75% of patients will need multiple treatments after 9 years.10,11
Hypertension was seen in 31.0% of patients. It is estimated that the prevalence of hypertension in type 2 diabetes ranges from 20% to 60%. 2 Hypertension was higher in our study compared to the 25% reported by Famuyiwa 12 but comparable to the 34% by Al-Nozha in Saudi Arabia. 13 This figure will even reach 96.7% for patients with diabetic nephropathy in Saudi patients. 14 In Iran hypertension was reported in 28.6% to 45.8% of diabetics. 15
Peripheral neuropathy was seen in 13.8% in this study, while it was seen in 34.7% of diabetics in Al Ain, United Arab Emirates, 8 in 13.7% to 35.9%, in Saudi Arabia.12,16 and up to 66.8% among diabetic nephropathy patients referred to the nephrology clinic in Saudi Arabia. 14 In Iran, diabetes-related neuropathy was found among a wide range (33.3% to 71.5%). 15
Ischemic heart disease was reported in 7.8% of the patients. Coronary heart disease was seen among 10.5% in Al Ain, United Arab Emirates, 8 up to 41.3% in Saudi patients, 13 in 25.2% of diabetics in the UK 17 and 28.0% of diabetics in Iran. 15
Proteinuria was seen in 6.6% in this study. Macroalbuminuria was prevalent in 6.8% Egyptians, 12.8% of Saudis, 12.7% of Lebanese and 12%–23% of Iranians.15,18
Cereberovascular accident was reported in 4.6% in this study. While it was seen in 9.4%–10.4% of Saudi patients12,14,16 and in 9.6% of 10,709 diabetic patients in the UK. 17
In this series, 2.7% developed diabetic foot and 0.7% had related lower extremity amputation. While in Saudi patients diabetic foot was seen in 4.3%, amputation in 1.9% in one study 16 and foot infections in 10.4% and amputations in 5.1% in another. 13 Diabetic foot was seen in 13.5%, and amputation in 5.4% among diabetic nephropathy patients referred to nephrology clinic in Saudi Arabia. 14 In Iran, diabetic foot ulcers were reported to be 2%–4% with 0.7% amputation 15 and complications relating to the diabetic foot were seen in 18.1%, of diabetics in the UK. 17
Peripheral vascular disease was seen in 0.2% in this study, while it was seen in 11.1% of diabetics in the United Arab Emirates. 8 A very high figure of peripheral vascular disease was seen in up to 65.7%, reported among diabetic nephropathy patients referred to nephrology clinic in Saudi Arabia. 14 This discrepancy between our study and others is because we were not using doppler study to assess the peripheral arterial disease and we used only symptomatic patients.
Cardiovascular cause of death was reported in 2.8% in this sample of patients. Among 1,952 patients seen in one institution in Saudi Arabia, 8.2% died. 16
Both the duration of diabetes and age contributed to chronic complications of diabetes in this study. Individual and multiple complication frequency increased with both age and duration of diabetes and the bulk of morbid complications are in the population with type 2 diabetes. 17
Neuropathy was found more in women in the study while the reverse was seen in Saudi patients. 16 In this study and that of Saudi patients, the mortality was higher in men.
Limitations
Microalbuminuria and retinopathy were not examined. The death was based on centre records and not from the community, so definitely the mortality is underestimated.
conclusion
This study provided the baseline for chronic complications of diabetes in Iraq. Of 4,926 diabetic patients the commonest chronic complications were hypertension, peripheral neuropathy, ischemic heart disease, proteinuria, and cereberovascular accident. Screening for early complications is recommended.
Conflict of Interest
The author declares that there are no conflicts of interest.
Footnotes
Acknowledgements
The author wish to thank Lesley Pocock Publisher and Managing Director medi + WORLD International World CME for reviewing of the manuscript.
The efforts made by the medical staff of the Al-Faiha Diabetes and Endocrine Centre in Basrah were quite appreciated through out the study.