
Abstract
Objectives
To analyze the associations of serum uric acid (SUA) level with diabetic microvascular complications, including diabetic retinopathy (DR) and diabetic nephropathy (DN), in patients with type 2 diabetes mellitus (DM).
Methods
Three hundred eighty-nine inpatients with type 2 DM were included in this retrospective analysis. Nonmydriatic fundus cameras were used to identify DR. Urinary albumin creatinine ratio was used to identify DN. Patients were divided into four groups according to SUA quartiles.
Results
The prevalences of DR and albuminuria increased with increasing SUA level. Multivariate logistic regression analysis showed that, following adjustment for other risk factors, higher levels of SUA (Q3 and Q4) were associated with greater risk for DR, compared with the lower level (Q1) (odds ratio [OR]: 3.056, 95% confidence interval [CI]: 1.506–6.198; OR: 3.417, 95% CI: 1.635–7.139, respectively). Moreover, higher levels of SUA (Q2, Q3, and Q4) were associated with greater risk for albuminuria (OR: 2.418, 95% CI: 1.059–5.522; OR: 7.233, 95% CI: 3.145–16.635; and OR: 8.911, 95% CI: 3.755–21.147, respectively).
Conclusions
SUA level was independently associated with DR and albuminuria in patients with type 2 DM. Elevated SUA level might be predictive for the occurrence of DR and DN.
Keywords
Introduction
Diabetes mellitus (DM) is one of the most common chronic diseases worldwide. It is continuously increasing in prevalence and public health importance because lifestyle changes have led to reduced physical activity and greater rates of obesity. Notably, the International Diabetes Federation reported that there were 451 million adults with DM worldwide in 2017; this number is expected to increase to 693 million by 2045. 1 The increasing incidence of DM has a considerable impact on the prevalence of diabetic microvascular complications, including diabetic retinopathy (DR) and diabetic nephropathy (DN). Diabetic microvascular complications constitute a substantial social, financial, and healthcare burden; they also have a considerable negative impact on quality of life for affected patients. 2 DR is a major cause of acquired blindness in working-age adults and is presumed to be responsible for 12% of blindness in developed countries. 3 Furthermore, DN is a leading cause of end-stage renal disease; the incidence of end-stage renal disease caused by DN is estimated to range from 35% to 50%. 4 In clinical practice, we have observed that rigorous control of blood glucose in patients with diabetes does not result in satisfactory efficacy; thus, the incidence of microvascular lesions in these patients remains high. Accordingly, we speculate that other risk factors might be associated with the incidence of DR and DN in patients with DM.
Uric acid is the end product of purine metabolism, mainly excreted by the kidneys. 5 Previous studies have demonstrated that serum uric acid (SUA) is biologically active and can stimulate oxidative stress, endothelial dysfunction, inflammation, and vasoconstriction. 6 A recent study of 749 Taiwanese patients with type 2 DM reported that an elevated SUA level was associated with DR. 7 Several large observational prospective studies have shown that hyperuricemia contributes to the development and progression of DN.8,9 However, DN and DR are both diabetic microvascular complications; to the best of our knowledge, their relationships with SUA have not been concurrently examined in a single study. The increasing incidence of albuminuria in patients with DM is a characteristic of DN; it is also a common predictor of renal function in patients with DN. 10 This cross-sectional study was performed to evaluate the associations of SUA with DR and albuminuria in patients with type 2 DM.
Materials and methods
Patients and study design
This retrospective analysis was conducted on inpatients with type 2 DM (aged 21 to 85 years) who underwent treatment from March 2017 to September 2017 at the Department of Endocrinology, Shandong Provincial Hospital Affiliated with Shandong University. All patients had been diagnosed in accordance with the 1999 World Health Organization criteria for DM, with a fasting plasma glucose concentration ≥7.0 mmol/L or 2-hour post-glucose load concentration ≥11.1 mmol/L. 11 All patients provided written informed consent to participate in this study. Unique patient numbers were used to de-identify patient records during data analysis. Patients who met the following criteria were excluded: (1) diagnosis of cancer, immunologic disease, and/or infection (e.g., urinary tract infection); (2) diagnosis of other kidney disease (e.g., chronic nephritis); (3) diagnosis of other fundus disease (e.g., high myopic maculopathy and/or age-related macular degeneration); (4) use of medications that could affect SUA or urine albumin levels; (5) pregnancy. This study was approved by the ethics committee of Shandong Provincial Hospital Affiliated with Shandong University (IRB no. 2018-219).
Anthropometrics
Clinical data were obtained from our hospital’s medical records system. A detailed interview regarding each patient’s medical history had been conducted at the time of hospitalization. Demographic data compiled for this study included age, sex, duration of DM, systolic blood pressure, diastolic blood pressure, and body mass index (BMI). Systolic blood pressure and diastolic blood pressure were measured by using an automated sphygmomanometer with the patient in a sitting position, following at least 5 minutes of rest. BMI was calculated as the ratio of weight in kilograms divided by the square of height in meters.
Biochemical measurement
Blood samples were obtained from each patient after 8 hours of overnight fasting; samples were tested by the Laboratory Department of Shandong Provincial Hospital. Fasting plasma glucose, total cholesterol, triglycerides, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, SUA, and serum creatinine were measured by a Beckman Chemistry Auto-analyzer AU5800 System (Beckman Coulter, Brea, CA, USA). Hemoglobin was measured using a TOSOH G8-90SL hemoglobin detector (Tosoh Corp., Tokyo, Japan). Estimated glomerular filtration rate was estimated by the simplified Modification of Diet in Renal Disease equation. Early DN was diagnosed by the urine albumin creatinine ratio (UACR; albuminuria was defined as UACR ≥30 mg/g) measured in spot urine samples using a BIOSTEC BA-400 specific protein autoanalyzer (Biosystems S.A., Barcelona, Spain). Hyperuricemia was defined as SUA >420 μmol/L (7.0 mg/dL) for men and >360 μmol/L (6.0 mg/dL) for women.
Assessment of DR
Screening for DR was performed using a nonmydriatic fundus camera (TRC NW-300 camera; Topcon Corp., Tokyo, Japan). Fundus photography was performed by trained nurses in a dim room. The camera was focused on the macula and 45-degree digital color fundus images were captured. All photographs were stored on a computer and printed for analysis. An experienced endocrinologist or ophthalmologist, both of whom had more than 10 years of experience, evaluated the fundus photographs. Patients were diagnosed with DR in accordance with the Early Treatment Diabetic Retinopathy Study guidelines: DR was defined as the presence of at least one retinal microaneurysm or blot hemorrhage with or without additional lesions such as exudates (hard or soft), intraretinal microvascular abnormalities, venous beading, neovascularization (disc or elsewhere), and vitreous hemorrhage. 12 Patients with any unreadable photograph in at least one eye underwent direct examination by an ophthalmologist to determine their DR status.
Statistical analysis
Continuous variables are presented as means±standard deviations or medians (interquartile ranges). Comparison of continuous variables between groups was performed by single-factor analysis of variance or the Kruskal–Wallis test. Categorical variables are presented as percentages and between-group differences were assessed by R×C crosstabs chi-squared tests. Multivariate logistic regression analysis was performed to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for risk factors of DR and albuminuria. P-values < 0.05 were considered statistically significant. All data were analyzed with SPSS Statistics, version 23.0 (IBM Corp., Armonk, NY, USA).
Results
Patient characteristics
This study included 389 patients with type 2 DM (238 men [61.2%] and 151 women [38.8%]; mean age, 57.93 ± 11.41 years). The respective prevalences of DR and albuminuria were 41.9% and 34.4%. SUA concentrations among patients in this study ranged from 118 μmol/L to 571 μmol/L; the mean SUA level was 323.07±87.66 μmol/L. Men had higher mean SUA levels than women (347.18±86.50 μmol/L vs. 285.07±75.36 μmol/L, P < 0.001). Patients were divided into quartiles according to SUA as follows: Q1 (≤264.00 μmol/L), Q2 (264–315 μmol/L), Q3 (315–378 μmol/L), and Q4 (>378.00 μmol/L) (Table 1). Significant differences were observed among the four groups with respect to sex, diastolic blood pressure, BMI, triglycerides, high-density lipoprotein cholesterol, serum creatinine, estimated glomerular filtration rate, and prevalences of DR and albuminuria (P < 0.05 for all). No significant differences among groups were observed with respect to age, duration of DM, systolic blood pressure, fasting plasma glucose, hemoglobin, total cholesterol, or low-density lipoprotein cholesterol.
Baseline characteristics of the patients according to uric acid quartile.

Data for continuous variables are presented as the mean and standard deviation or median and interquartile range; categorical variables are presented as percentages. Quartiles of uric acid were ≤264.00, 264.00–315.00, 315.10–378.00, and >378.00 μmol/L.
BMI: body mass index, DBP: diastolic blood pressure, DM: diabetes mellitus, DN: diabetic nephropathy, DR: diabetic retinopathy, FPG: fasting plasma glucose, eGFR: estimated glomerular filtration rate, HbA1c: glycated hemoglobin, HDL-C: high density lipoprotein cholesterol, LDL-C: low density lipoprotein cholesterol, SBP: systolic blood pressure, Scr: serum creatinine, TC: total cholesterol, TG: triglyceride.
Prevalences of DR and albuminuria according to SUA quartile
We investigated the relationships of SUA concentration with the prevalences of DR and albuminuria. Figure 1a shows the prevalence of DR according to SUA quartiles, which ranged from 26.32% (Q1) to 55.67% (Q4). A positive trend was observed between DR prevalence and SUA quartile (χ2 = 20.76, P < 0.001, crosstabs chi-squared test for trend). Further investigation revealed that DR prevalences were significantly higher in the third and fourth quartiles than in the first quartile (P = 0.001, P < 0.001 respectively). Compared with the second quartile, DR prevalence was also significantly higher in the fourth quartile (P = 0.006). Figure 1a also shows the prevalence of albuminuria according to SUA quartiles, which ranged from 11.58% (first quartile) to 55.67% (fourth quartile). A similar positive trend was observed between albuminuria prevalence and SUA quartile (χ2 = 56.64, P < 0.001, crosstabs chi-squared test for trend). Further analysis showed that albuminuria prevalences were significantly higher in the third and fourth quartiles than in the first quartile (both P < 0.001). Compared with the second quartile, albuminuria prevalences were also significantly higher in the third and fourth quartiles (both P < 0.001). However, there were no significant differences in the prevalences of DR or albuminuria between the third and fourth quartiles (Figure 1a).
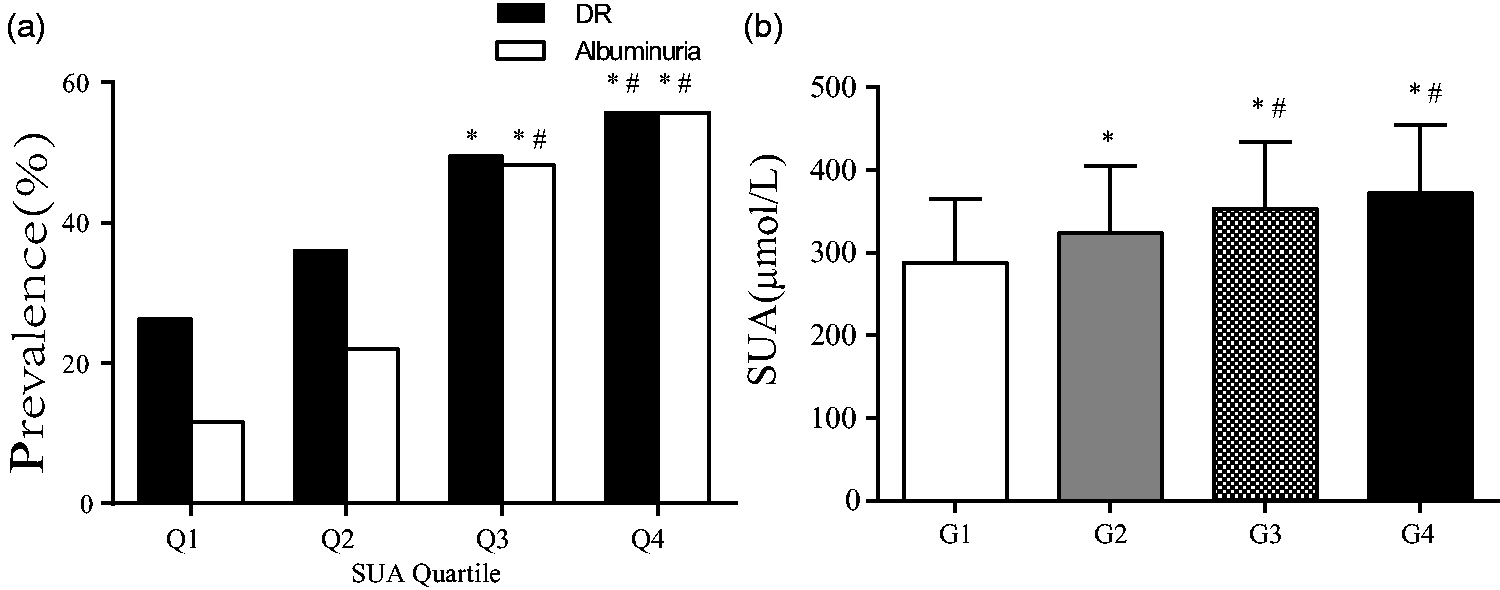
Relationships of serum uric acid level with the prevalences of diabetic retinopathy and albuminuria. (a): Prevalences of DR and albuminuria. Increasing prevalences of DR and albuminuria were observed with increasing SUA quartile. Chi-squared analysis showed a significant trend (χ2 = 20.76, P < 0.001, (χ2 = 56.64, P < 0.001). Quartiles of SUA were <264.00, 264.00–315.00, 315.00–378.00, and ≥378.00 μmol/L. *P < 0.05 compared with Q1, #P < 0.05 compared with Q2. (b): SUA levels in patients with diabetes, with or without DR or albuminuria. *P < 0.05 compared with G1, #P < 0.05 compared with G2.
Subsequent classification of all patients into four groups according to the presence of DR and/or albuminuria yielded the following numbers of patients: group 1, 176 patients without DR or albuminuria; group 2, 79 patients with DR alone; group 3, 50 patients with albuminuria alone; and group 4, 84 patients with both DR and albuminuria. SUA concentrations were significantly lower in group 1 than in the other groups (P < 0.05). SUA concentrations were significantly higher in groups 3 and 4 than in group 2 (P < 0.05). Although SUA concentrations tended to gradually increase between groups 3 and 4, this difference was not statistically significant (Figure 1b).
Associations of SUA with risk factors for DR and albuminuria
Multivariate regression logistic analysis to identify risk factors for DR showed that duration of DM, hemoglobin level, BMI, serum creatinine level, UACR, and SUA level were associated with DR (Table 2). Similar analysis to identify risk factors for albuminuria showed that sex, age, duration of DM, systolic blood pressure, estimated glomerular filtration rate, and SUA level were associated with albuminuria (Table 3).
Risk factors for diabetic retinopathy, according to multivariate logistic regression.

Values are expressed as odds ratios (ORs) and 95% confidence intervals (CIs).
BMI: body mass index, DM: diabetes mellitus, HbA1c: glycated hemoglobin, Scr: serum creatinine, SUA: serum uric acid, UACR: urinary albumin creatinine ratio.
Risk factors for albuminuria, according to multivariate logistic regression.
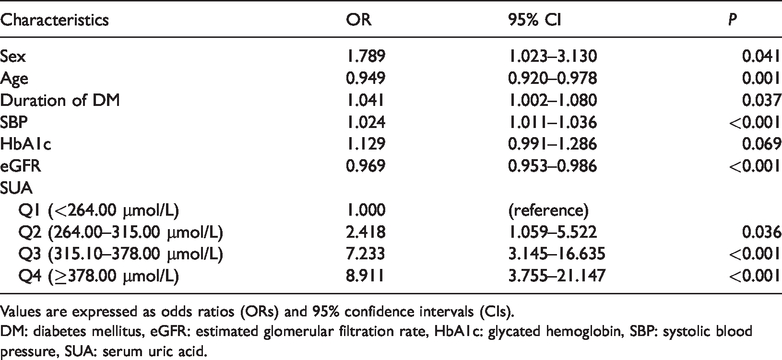
Values are expressed as odds ratios (ORs) and 95% confidence intervals (CIs).
DM: diabetes mellitus, eGFR: estimated glomerular filtration rate, HbA1c: glycated hemoglobin, SBP: systolic blood pressure, SUA: serum uric acid.
When SUA was used as a tertiary variable, groups with higher SUA levels (Q3 and Q4) showed threefold (P = 0.002 and P = 0.001, respectively) greater risk for DR, compared with the lower level (Q1). Moreover, groups with higher levels of SUA (Q2, Q3, and Q4) showed twofold (P = 0.036), sevenfold (P < 0.001), and ninefold (P < 0.001) greater risk for albuminuria, compared with the lower level (Q1), respectively.
Discussion
The main finding of this study was that SUA level was an independent risk factor for DR and albuminuria in a Chinese population of patients with DM. As shown in Figure 1a, with increasing SUA level, the prevalences of DR and albuminuria also increased. Moreover, SUA levels were higher in patients with type 2 DM who had DR and/or albuminuria, compared with patients who did not have DR or albuminuria. Multivariate analyses showed that patients with higher SUA levels had significantly greater ORs for the risk of DR and albuminuria, compared with patients who had lower SUA levels, despite adjustment for potential confounding factors. These findings suggested that an elevated SUA level may be closely associated with onset of DR and DN among patients with type 2 DM.
Hyperuricemia is a metabolic disturbance involving purine nucleotides, which is considered an important risk factor for most noncommunicable diseases (e.g., DM). Previous studies have quantitatively estimated the risks of SUA level associated with obesity and various components of metabolic syndrome in adult and elderly populations.13,14 In this study, we found that BMI and diastolic blood pressure were significantly higher, while high-density lipoprotein cholesterol was lower, in patients with higher SUA levels. However, specific relationships of SUA level with DM microvascular complications were not clearly established.
DR is an important microvascular complication of DM and a leading cause of vision loss in middle-aged and elderly people. 15 A previous study showed that the overall prevalence of any DR (in patients with types 1 or 2 DM) was 34.6% (95% CI: 34.5–34.8). 16 The present study showed that the frequency of DR was 41.9% among patients with type 2 DM; this was higher than the global prevalence, presumably because our study population consisted of inpatients, most of whom exhibited poor blood glucose control.
Some studies have suggested that DM duration, glycemia, blood pressure, and body weight are common risk factors for DR.17,18 However, it remains controversial whether SUA level is a risk factor for DR. A recent study revealed that SUA was not associated with DR after adjustment for DM duration in patients with type 1 DM. 19 Another study, involving 746 Chinese patients with type 2 DM, revealed elevated SUA levels in patients with more severe DR; however, it did not demonstrate that SUA was an independent risk factor for DR. 20 A previous epidemiological study showed a relationship between SUA level and DR risk, implying that SUA plays an important role in the development of DR; 7 several potential mechanisms might underlay this relationship. A study of Chinese patients with high risk of DM revealed that hyperuricemia was associated with smaller retinal arteriolar caliber and larger venular caliber, mainly in male patients. 21 Accordingly, elevated SUA level might lead to vascular constriction within the retina. Krizova et al. found that SUA levels in the vitreous were elevated in patients with DM. 22 In the present study, as SUA level increased, the prevalence of DR also increased. Furthermore, we observed that higher SUA level was significantly associated with a twofold greater risk of DR. These findings support the notion that higher SUA level is an independent risk factor for DR.
Elevated SUA levels occur in many renal diseases. The mechanisms underlying elevated SUA may involve reduction of the estimated glomerular filtration rate or dysfunctional management of filtered uric acid by proximal tubules. 23 Uric acid is an important contributor to the development of renal disease. 24 DN is the main cause of end-stage renal failure, which is also an important cause of death and disability in patients with DM. DN and DR are both microvascular complications of type 2 DM. Several studies have also focused on the relationship between SUA level and DN. Albuminuria indicates the presence of diabetic microvascular disease and is an early manifestation of DN. The detection of UACR in patients with DM is a common method for clinical screening of renal disease in such patients. Several studies have demonstrated that SUA level is associated with the progression of albuminuria in patients with DM and is an independent risk factor for more rapid progression of DN in such patients.25–29 Our findings are consistent with the previous results regarding the association of SUA level with albuminuria.
Kosugi et al. 30 found that the reduction of uric acid by allopurinol improved renal function, proteinuria, and tubulointerstitial damage in type 2 diabetic db/db mice. The mechanism for renal damage was presumably uric acid-induced intrarenal inflammation because renal injury was associated with enhanced macrophage infiltration. Serum monocyte chemoattractant protein-1 level and tubular intercellular adhesion molecule-1 expression were reduced in allopurinol-treated mice. The inflammatory effect of uric acid in tubular epithelial cells was also demonstrated in an in vitro study whereby uric acid directly induced the expression of intercellular adhesion molecule-1 in human proximal tubular cells. 30 In a clinical study, Wada et al. revealed that appropriate management of hyperuricemia at an early stage of diabetic kidney disease may contribute to renal protection. 31 They showed that compared with the placebo group, the level of UACR in the group receiving topiroxostat (a selective xanthine oxidoreductase inhibitor) did not tend to increase in patients with hyperuricemia and DN who exhibited microalbuminuria. These findings suggested that xanthine oxidase inhibitors might be beneficial for the treatment of DN; moreover, the mechanism might be involved in the prevention of uric acid-induced renal inflammation. 30
The present study also found that blood pressure and hemoglobin were significantly associated with albuminuria, as demonstrated in previous studies. 32 Pilemann-Lyberg et al. reported that SUA level was not significantly associated with the progression of kidney disease or other complications, following adjustment for traditional risk factors, in patients with type 1 DM. 33 A study of 385 Taiwanese patients with type 2 DM revealed that hyperuricemia was significantly associated with the severities of both DR and albuminuria. 34 To the best of our knowledge, no data were previously reported regarding the relationships of SUA level with DR or albuminuria in patients with type 2 DM in mainland China. Our findings in the present study imply that a high SUA level is closely associated with the risks of DR and albuminuria. DR and DN are two typical diabetic microvascular complications that may thus exhibit common etiologies.
Multiple studies have indicated that SUA level may play a role in diabetic peripheral neuropathy. A meta-analysis showed that elevated SUA level was independently associated with an increased risk of diabetic peripheral neuropathy in patients with type 2 DM. 35 Furthermore, Matheus et al. reported that an elevated SUA level was significantly associated with diabetic chronic micro/macrovascular complications. 36 Accordingly, SUA might contribute to the occurrence and development of diabetic microvascular complications. Potential mechanisms include onset of endothelial dysfunction, activation of the renin–angiotensin–aldosterone system, elevation of oxidative stress, and enhancement of inflammatory cascades. 37
There were some limitations in this study. First, the cross-sectional design prevented inferences regarding causality. Second, a nonmydriatic fundus camera was used for fundus photography. This was only a screening method for the presence of DR; thus, it could not determine the severity of DR in affected patients. However, a previous study showed that nonmydriatic images had sensitivity and specificity of 92% and 82%, respectively, for the diagnosis of DR. 38 Finally, we considered the albuminuria as a categorical variable; thus, we could not fully evaluate the relationship between SUA level and UACR. A more comprehensive study is needed to investigate the relationships of SUA level with diabetic microvascular complications.
Conclusion
Our data showed that the patients with an elevated SUA level were more likely to have high prevalences of DR and albuminuria, compared with patients who had a low SUA level. Therefore, even within the normal range of SUA, patients with relatively high SUA levels might be more likely to develop DR and DN. Thus, SUA level should be carefully monitored in patients with type 2 DM.
Footnotes
Acknowledgements
We thank all participants for their willingness to complete the study.
Authors’ Contributions
L.H. collected the clinical data, analyzed and interpreted data, and drafted, and critically revised the manuscript; Y.S. and S.W. analyzed and interpreted data, and critically revised the manuscript for intellectual content; Q.C. and Q.L. recruited the patients; M.Z. analyzed and interpreted data, and critically revised the manuscript for intellectual content; X.Z. is the guarantor of this research, conceived and designed the study, had full access to all the data in the study, and takes responsible for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shandong Key R&D Program (Grant No. 2017GSF18129), the National Key Research and Development Plan (Grant No. 2017YFC1309805), and the Special Fund for Clinical Medical Science Research of the Chinese Medical Association (Grant No. 12020330323).